Major complications after TACE remain rare but deadly, the main complications can be vascular: within the access artery or the hepatic artery, or non-vascular: post-embolization syndrome (PES), biliary tract injuries, non-target regional or distant (cerebral or pulmonary) embolization, intra- or extra hepatic infection, TACE induced hepatic failure, hepatic rupture and many others.
We report 3 complications in 2 patients: hepatic abscess, portal thrombosis and hepatic failure. The 2 patients unfortunately died after severe hepatic failure. Both of the two patients developed portal thrombosis after chemoembolization. This is the first case report of portal thrombosis developed after TACE with an extended hepatic necrosis in the second case. This article reviews different aspects of liver abscess complicating TACE for HCC.
HCC, TACE, Complications
Major complications after TACE for HCC occur approximatively in 2.7 to 5% of patients [1,2]. The main complications can be vascular: Within the access artery or the hepatic artery, or non-vascular: Post-embolization syndrome (PES), biliary tract injuries, non-target regional or distant (cerebral or pulmonary) embolization, intra- or extrahepatic infection, TACE induced hepatic failure, hepatic rupture and many others [1].
The incidence of liver abscess in literature varies between 0.2% and 2% [1]. It is statistically discrepant among different institutions and regions, which is likely attributed to the heterogeneous populations, variation in chemoembolization technique, and number of patients studied.
We report 3 complications in 2 patients: Hepatic abscess, portal thrombosis and hepatic failure. The 2 patients unfortunately died after severe hepatic failure. Both of the two patients developed portal thrombosis after chemoembolization. This is the first case report of portal thrombosis developed after TACE with an extended hepatic necrosis in the second case. This article reviews different aspects of liver abscess complicating TACE for HCC.
Clinical history: A 46-years-old man followed for cirrhosis with hepatitis C virus (HCV) as an etiology. He was tabetic, under beta blockers, spironolactone and furosemide. A nodule was diagnosis on follow up US for his cirrhosis. An Angiographic computed tomography (ACT) was performed (Figure 1 and Figure 2) to characterize the nodule according to Barcelona clinic liver cancer (BCLC) criteria and recommendations. The table below resumes the main patient characteristics (Table 1).
Table 1: Main characteristics related to HCC of the two patients before TACE. View Table 1
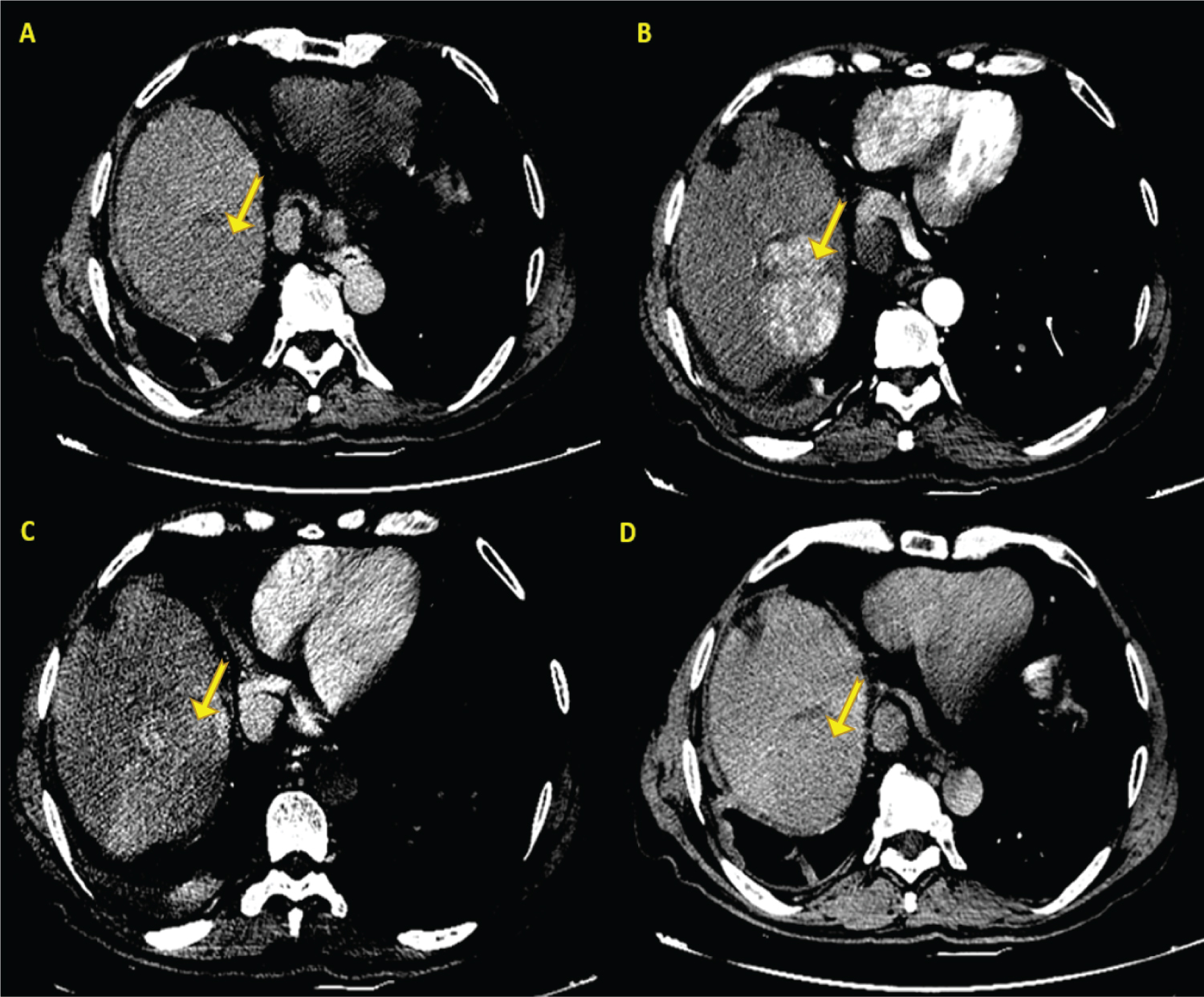 Figure 1: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. A nodule was diagnosis on follow up US for his cirrhosis. An ACT was performed to characterize the lesion according to BCLC criteria.
Figure 1: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. A nodule was diagnosis on follow up US for his cirrhosis. An ACT was performed to characterize the lesion according to BCLC criteria.
Technique: Non-enhanced, arterial, portal and late phase IV contrast enhanced (100 ml of Iopromide 300) axial acquisition 64 detector CT (GE Lightspeed VCT) of the liver acquired at 2.5 mm slice thickness, non-gated, 120 kVp and 200 mAs.
Findings: Axial images of abdominal CT shows a large tumor (arrows) localized on the VII and VIII segments, isodense on spontaneous contrast A) presenting an early enhancement on arterial acquisition B) with portal C) and late wash out D).
View Figure 1
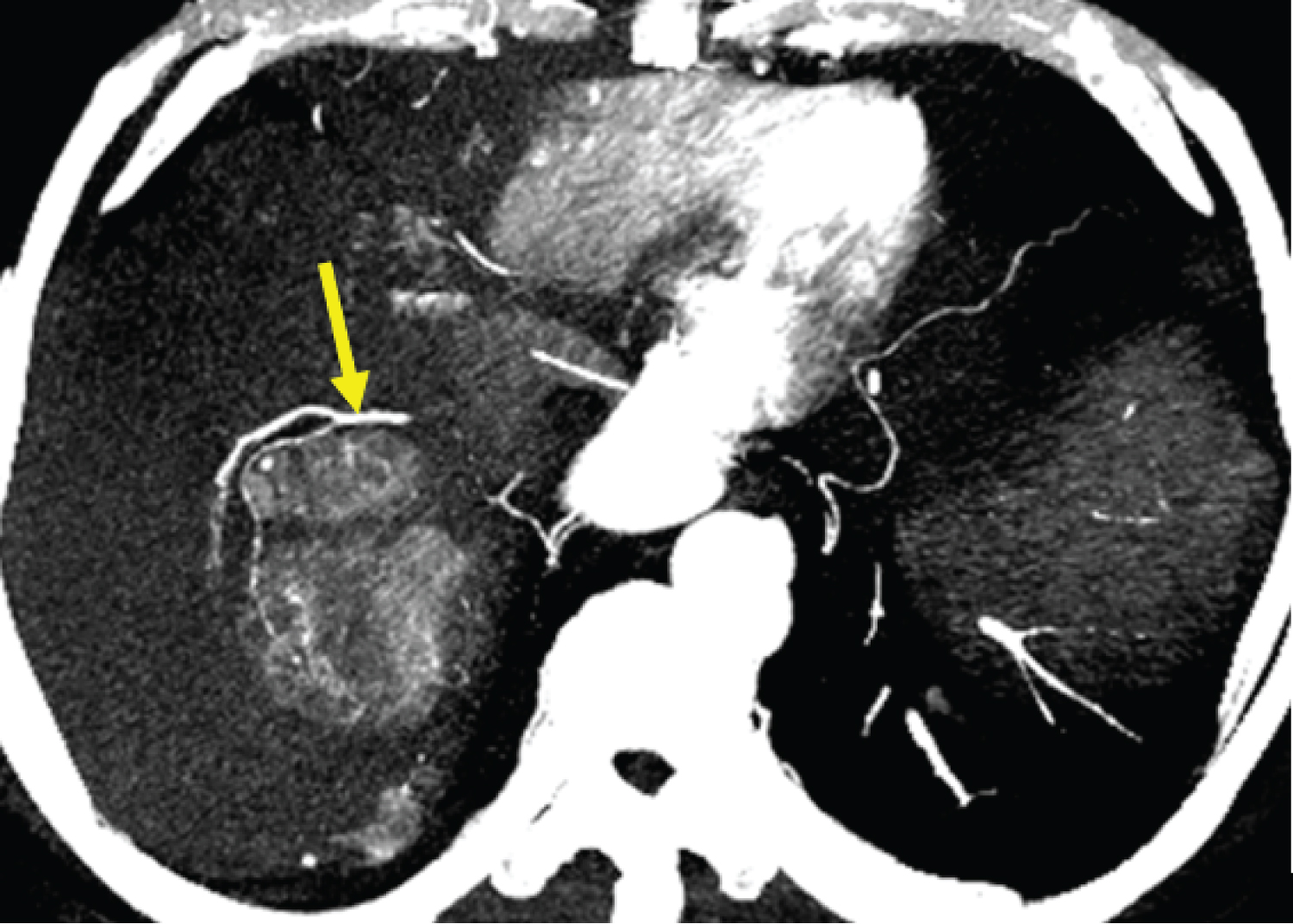 Figure 2: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. A nodule was diagnosis on follow up US for his cirrhosis. An ACT was performed to characterize the lesion according to BCLC criteria.
Figure 2: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. A nodule was diagnosis on follow up US for his cirrhosis. An ACT was performed to characterize the lesion according to BCLC criteria.
Technique: Arterial phase IV contrast enhanced (100 ml Iopromide 300) axial MIP reconstruction 64 detector CT (GE Lightspeed VCT) of the liver acquired at 2.5 mm slice thickness, non-gated, 120 kVp and 200 mAs.
Findings: Feeding artery (arrow) from the VII segmental branch emerging from the right accessory hepatic artery, it’s self-coming from the SMA (not shown).
View Figure 2
TACE procedure: We processed to the puncture of the right common femoral artery by a 5 F introducer according to Seldinger approach. Catheterization of the mesenteric superior artery (MSA) with a Cobra 4 F probe was performed and followed by catheterization of the arterial branches targeted to the segment VII and VIII with a Progreat 2.7 F microcatheter. Seriography shows the presence of an arterial blush (Figure 3).
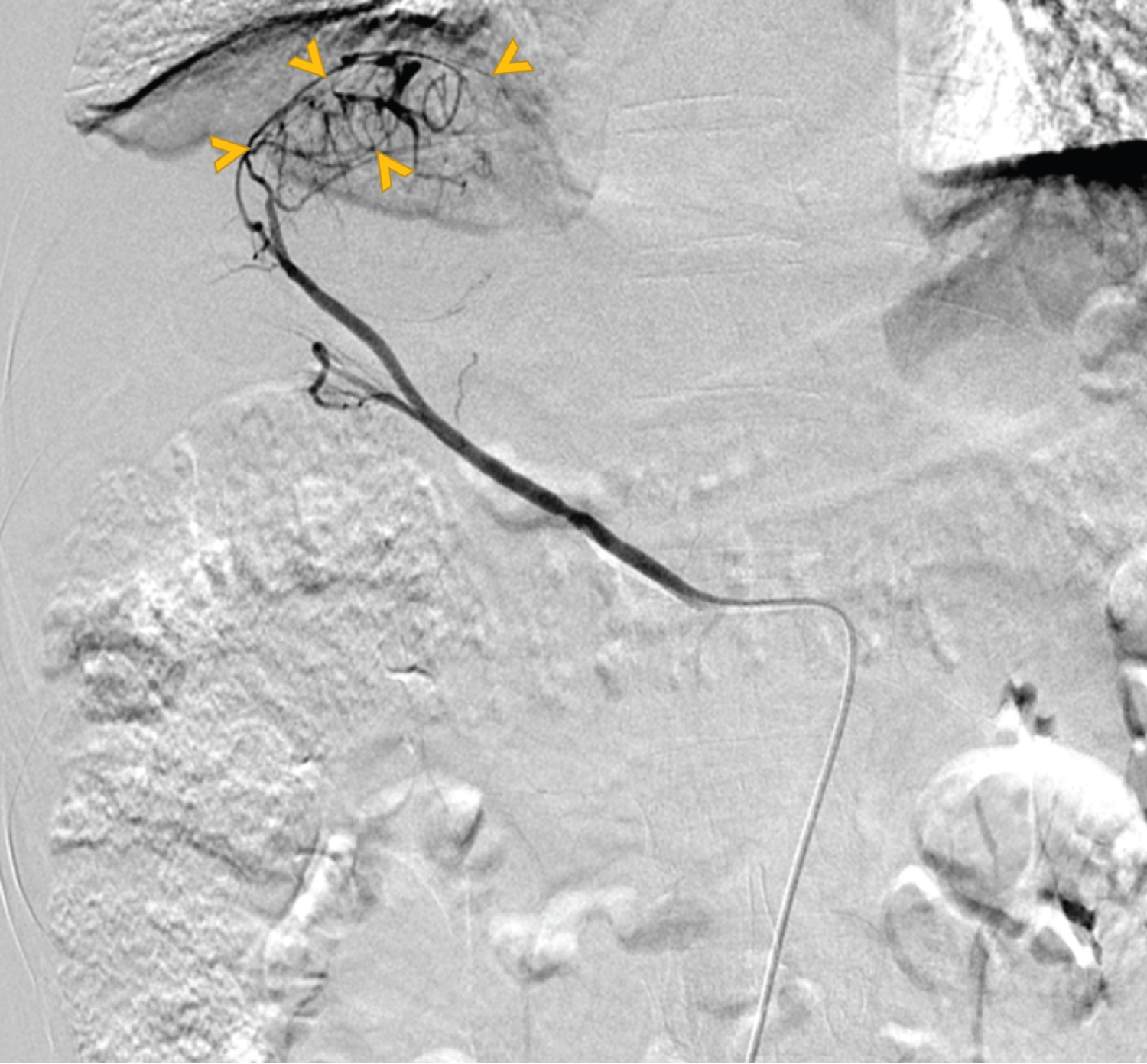 Figure 3: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. An HCC of the VII and VII segments was diagnosed on ACT and admitted later for TACE.
Figure 3: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. An HCC of the VII and VII segments was diagnosed on ACT and admitted later for TACE.
Technique: Arterial phase IV contrast (5 ml Iopromide 300 mixed with 5 ml of isotonic saline) front view biplane DSA (GE) of the liver.
Findings: SMA injection demonstrates large hypervascular tumor located in the projection of the VII and VIII segments.
View Figure 3
Embolization made by 120 mg of Doxorubicin, carried by 16 ml of Lipiodol ultra-fluid (UF). The mixture is made stable by the combination of 4 ml of Ultravist (Iopromide). The patient received 100% of the resulting emulsion. Embolization was completed with ¼ gelatin platelet.
The control seriography shows good Lipiodol fixation. Angiographic control showed total disappearance of the tumoral blush.
Evolution and management: The patient developed fever of 39.6° 3 weeks after transarterial chemoembolization (TACE), white blood count (WBC) count was elevated at 25720 elements per ml with 95.8% of neutrophils, C reactive protein CRP was about 210 mg/l compared to normal WBC and CRP counts before TACE. Important ascension of hepatic enzymes and decreased prothrombin time (PT) were identified.
An ACT was performed (Figure 4) immediately demonstrating decreased volume of the hepatic cell carcinoma (HCC) measuring 69 mm versus 76 mm with lipiodol fixation and liquefaction estimated at 90%. There was newly appearance of gaseous croissant in the lesion associated to adjacent pleural effusion.
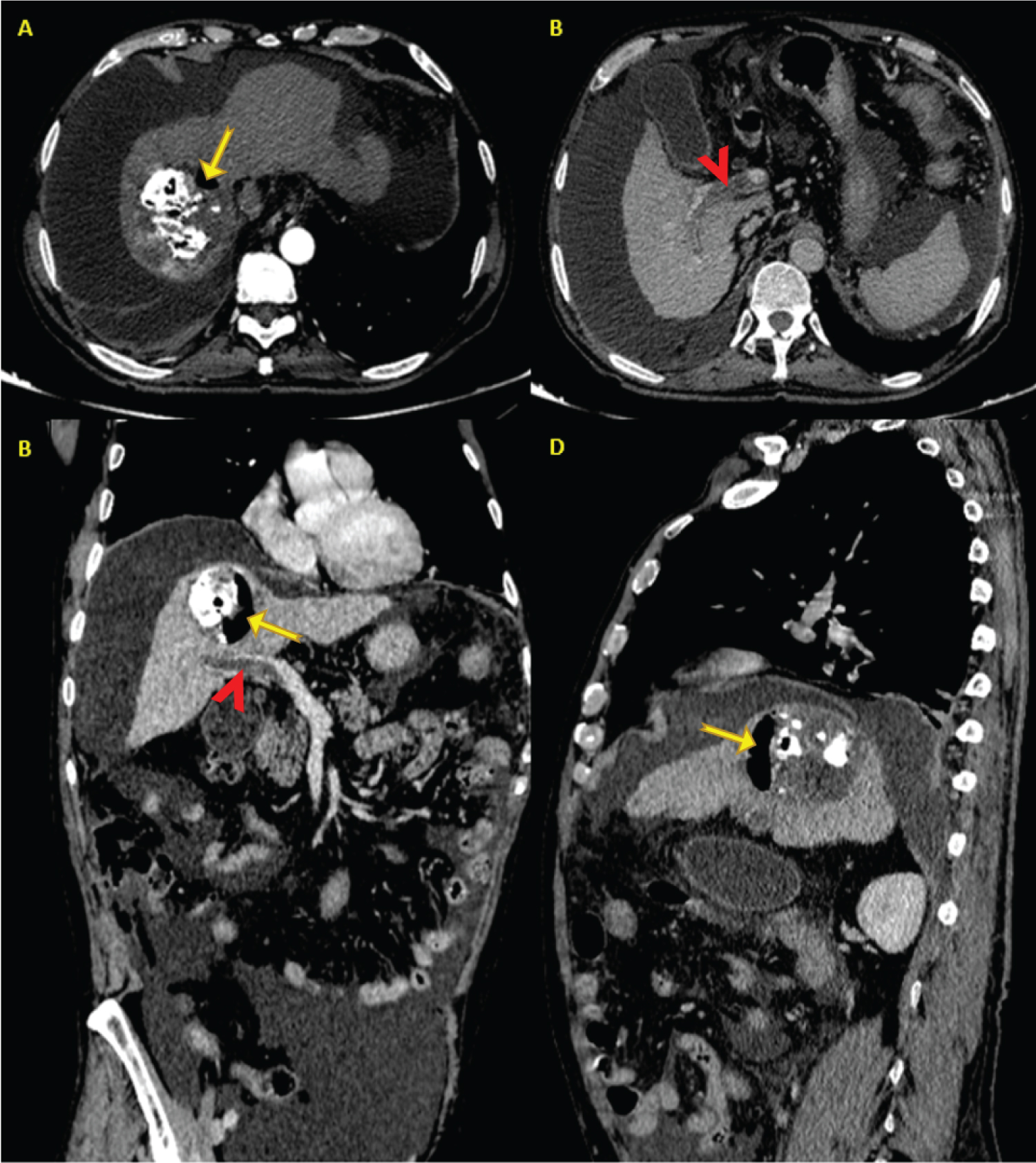 Figure 4: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. An HCC of the VII and VII segments was treated by TACE. ACT was performed 3 weeks later for hepatic abscess suspicion.
Figure 4: History: A 46-year-old man followed for cirrhosis with HCV as an etiology. An HCC of the VII and VII segments was treated by TACE. ACT was performed 3 weeks later for hepatic abscess suspicion.
Technique: Arterial and portal phase IV contrast enhanced (100 ml Iopromide 300) axial acquisition 64 detector CT (GE Lightspeed VCT) of the liver acquired at 2.5 mm slice thickness, non-gated, 120 kVp and 200 mAs.
Findings: Axial image in arterial phase (A) and portal phase: axial (B), coronal and oblique (C) and sagittal (D) reconstructions, show a dysmorphic liver with irregular contours. There is gaseous croissant (arrows) in the lesion with adjacent pleural effusion. Notice the sub-total thrombosis of portal vein extended to its right branch (arrow heads). The newly appearing important ascites which was not present on the ACT performed 6 weeks before is explained by the current acute hepatic failure.
View Figure 4
Curative anticoagulation associated to systemic antibiotic therapy was initiated and subsequently adapted to the results of blood culture which was positive to Escherichia Coli (EC) bacteria. In addition to this, we noticed a partial portal vein thrombosis extended to its right branch. The important ascites newly appeared suggest hepatic failure complicating. Patient undergoes severe hepatic failure and hepatic encephalopathy causing his death.
Clinical history: A 75-years-old man followed for cirrhosis of unknown cause, under treatment made from beta blockers, spironolactone and furosemide, was diagnosis with a nodule on follow up US. An ACT was performed to characterize the nodule according to BCLA criteria (Figure 5). The table below resumes the main patient characteristics (Table 1).
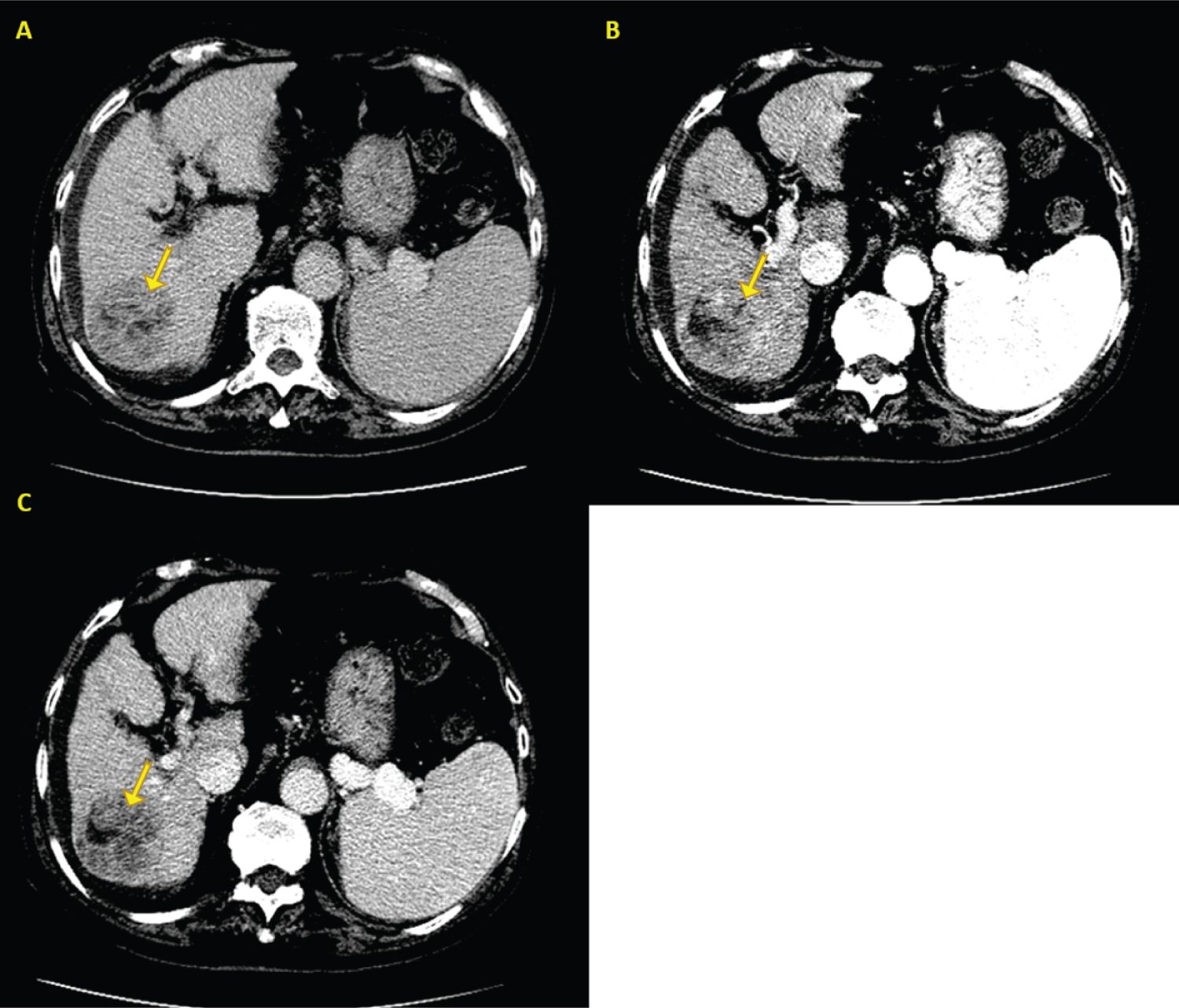 Figure 5: History: A 75-year-old man followed for cirrhosis with an unknown etiology. A nodule was diagnosis on follow up US for his cirrhosis. An ACT was performed to characterize the lesion according to BCLC criteria.
Figure 5: History: A 75-year-old man followed for cirrhosis with an unknown etiology. A nodule was diagnosis on follow up US for his cirrhosis. An ACT was performed to characterize the lesion according to BCLC criteria.
Technique: Non-enhanced, arterial, portal and late phase IV contrast enhanced (100 ml Iopromide 300) axial acquisition 64 detector CT (GE Lightspeed VCT) of the liver acquired at 2.5 mm slice thickness, non-gated, 120 kVp and 200 mAs.
Findings: Axial images of abdominal CT showing a well-defined, rounded, spontaneously hypodense and heterogenous lesion of the VI segment, sub-capsular (A), with slightly peripheral and heterogenous wash in (B) and an early wash out in portal phase (C).
View Figure 5
TACE procedure: A catheter was utilized to select the celiac artery followed by an angiogram which demonstrates a conventional celiac arterial anatomy. A microcatheter was advanced into the hepatic artery followed by an additional angiogram (Figure 6). A mixture of 100 mg of Doxorubicin and 15 ml of Ethiodol® was slowly infused into the left hepatic artery under fluoroscopic guidance. Two-thirds of the Doxorubicin/Ethiodol® mixture had been given. Control showed total extinction of tumoral blush.
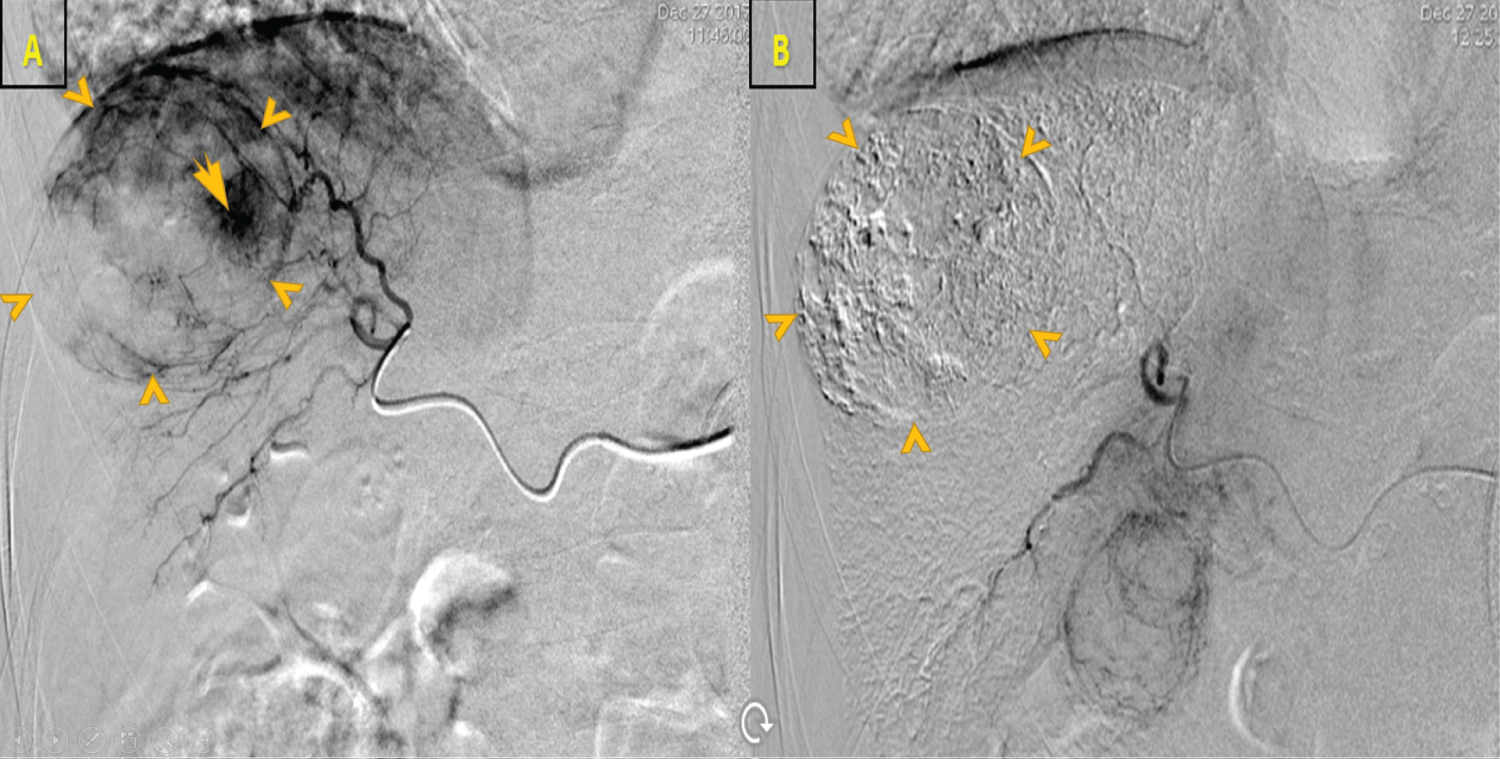 Figure 6: History: A 75-year-old man followed for cirrhosis with HCV as an etiology. An HCC of the VI segment was diagnosed on ACT and admitted later for TACE.
Figure 6: History: A 75-year-old man followed for cirrhosis with HCV as an etiology. An HCC of the VI segment was diagnosed on ACT and admitted later for TACE.
Technique: Arterial phase IV contrast (5 ml Iopromide 300 mixed with 5 ml of isotonic saline) front view biplane DSA (GE) of the liver.
Findings: Right hepatic arteriogram during TACE showing a large hypervascular HCC (arrow heads) of the right lobe (A). Control after embolization showing total extension (arrow heads) of the tumoral blush (B).
View Figure 6
Evolution and management: 2 weeks after TACE, the patient was admitted in emergency for acute pain in the right hypochondria associated to fever of 40°. Control of hepatic function shows important elevation of transaminases with ascension of the WBC count (21356 elements/ml), CRP (180 mg/l) and hepatic enzymes.
ACT performed few days later showed sub-total portal thrombosis causing hepatic necrosis of the segments V, VI and VII (Figure 7). Besides to this, there was appearance of air bubbles inside the tumor.
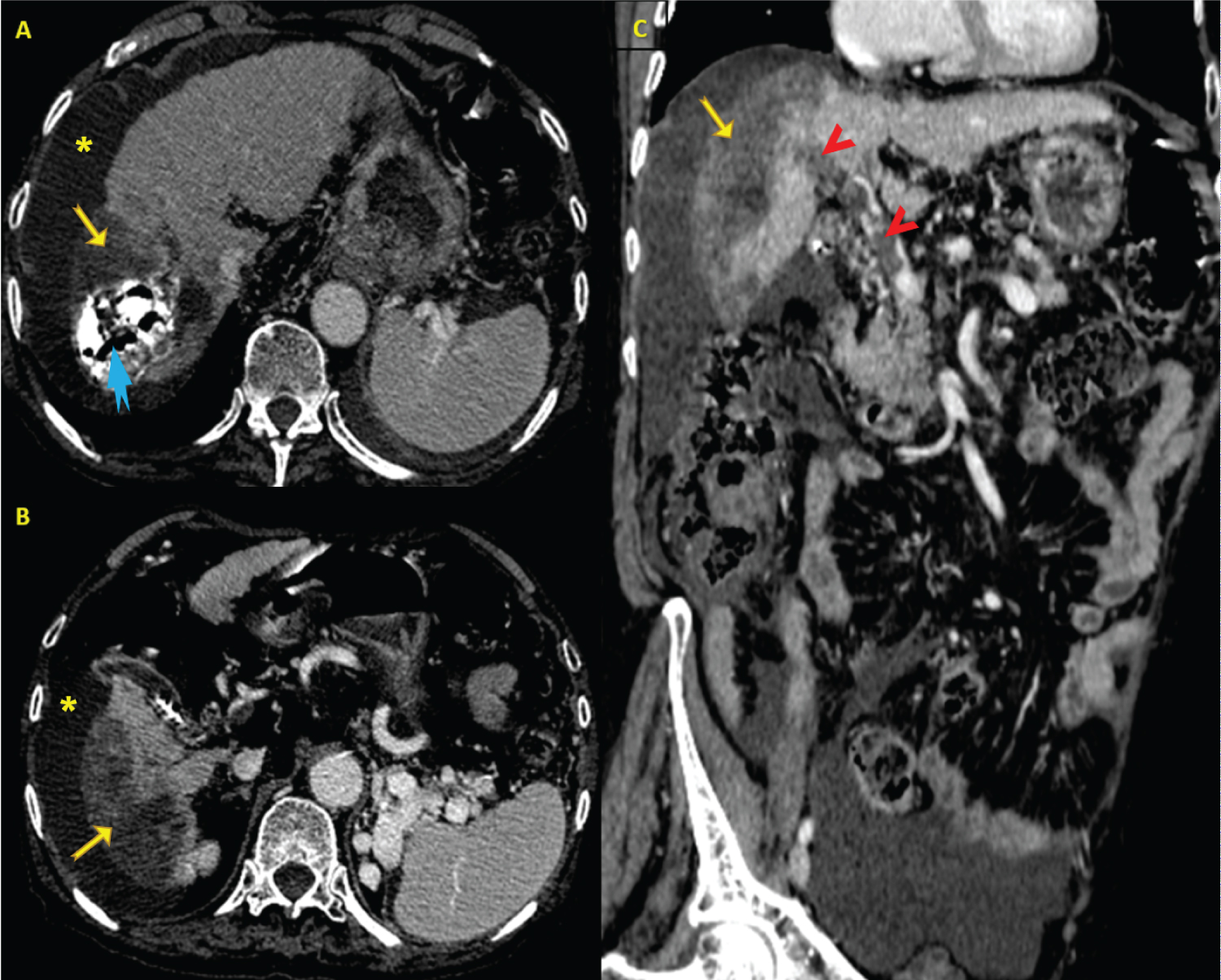 Figure 7: History: A 75-year-old man followed for cirrhosis with unknown etiology. An HCC of the segment VI was treated by TACE, ACT is performed 2 weeks later for hepatic abscess suspicion.
Figure 7: History: A 75-year-old man followed for cirrhosis with unknown etiology. An HCC of the segment VI was treated by TACE, ACT is performed 2 weeks later for hepatic abscess suspicion.
Technique: Arterial and portal phase IV contrast enhanced (100 ml Iopromide 300) axial acquisition 64 detector CT (GE Lightspeed VCT) of the liver acquired at 2.5 mm slice thickness, non-gated, 120 kVp and 200 mAs.
Findings: CT images in portal phase and axial plan (A, B) and oblique reconstruction (C) show enhancement defect of the segments VI and VII (yellow arrows) caused by sub-total portal thrombosis (arrow heads). Lipiodol fixation with liquefaction was estimated at 90% of the tumor volume. There are gaseous bubbles (blue arrow) in the lesion with adjacent pleural effusion (asterix). The newly appearing important ascites which was not present on the ACT performed 5 weeks before is explained by the current acute hepatic failure.
View Figure 7
Like the first case, patient received curative anticoagulation associated to systemic antibiotic EC bacteria identified on blood culture. Unfortunately, patient developed few days’ later severe hepatic failure and hepatic encephalopathy causing his death.
Etiology & demographics: TACE is the standard treatment option for patients with unresectable HCC and intermediate stage (BCLC B).
Major complications occur in 5% of patients, with 1% as risk of death [1]. According to a study conducted by Jianfei Tu, et al. incidence of major complication was 2% per patient and 0.8% per TACE procedure; the most frequently reported major complication was liver rupture; the mortality rate of major complications following TACE was 16% [3].
The incidence of liver abscess in literature varies between 0.2 and 2% per TACE and 0.6% to 4.5% per patient [4]. The mortality rates ranges from 13% to 50% [5,6]. The age range from 40 to 75 years, 70% of them are males [4]. In our experience, among 57 patients treated by TACE for HCC, 3 among them developped hepatic abcess (Incidence of 5.3%).
Intrahepatic abscess can be developed within the necrotic center of a devascularized hepatic tumor. The precise mechanism of abcess formation following TACE for HCC remain unclear, nut it seems that infection can be either iatrogneic during TACE procedure or non-iatrogenic in patients with specific conditions such as bilioenteric anastomosis. The bacterial infection is developped within the necrosis induced by embolization. The immunosuppressant effect of chemotherapeutic agents and diabetes mellitu lead to decreased immunity and promotes the abcess formation [7].
Clinical & imaging findings: The most common symptoms are right hypochondrium and/or epigastric abdominal pain followed by high-grade fever usually delayed beyond 7 days where is (Post-embolization syndrome) PES typically occurs before 7 days [4]. In this report, there were 2 and 3 weeks between TACE and the first symptoms related to the hepatic abcess.
Several risk factors are reported including: Old age, diabetes mellitus, large tumor size, portal vein occlusion and bilioenteric anastomosis or several biliary abnormalities [8]. In this study, one patient was 75-years-old, and the other one was tabetic without any other risk factor.
It is essential to carry out a bacteriological culture of the blood with an antibiogram. Gram-negative bacteria such as E coli and E cloacae are the most common [4].
Imaging findings: Diagnosis of an abscess following TACE can frequentelly be confused with tumor necrosis which is expected after embolization. Liquefactive necrosis of embolized tumor can demonstrate an area of low density on CT and can also contain gas [9]. However, Gas containing focal lesion found on CT and ultrasonogram remain the most valuable clue leading to the suspicion and early diagnosis of a liver abscess after TACE therapy, this sign is found up to 70% of patients [7].
The imaging diagnosis of liver abcess in these two reported cases was based effectivelly on the gas presence through the embolized HCC, no distinct abcess wall has been noted in portal time. In addition to this, there was sub-total thrombosis of the portal truck which wasn’t present on anterior CT and before or while performing TACE. We suppose that this thrombus can be septic and cruoric rather than neoplastic given the current context and its absence on CT performed few weeks before.
To the best of our knowledge, no case was reported before for portal vein thrombosis occurring after TACE. Proximal portal thrombosis diagnosed before TACE is an absolute contraindication of TACE because it is associated to a high risk of hepatic failure and infraction [10].
Treatment & prognosis: Liver abscess occurring after TACE for HCC ≤ 5 cm must undergo systemic antibiotic therapy, 3rd-generation cephalosporin and vancomycin should be used for obtaining a whole coverage of gram-positive and gram-negative bacteria, this antibiotic therapy must be subsequently adapted to the results of antibiogram of blood culture.
Percutaneous catheter drainage (PCD) is recommended as a first-line treatment because the abscess is usually ≥ 5 cm or multiloculated and frequently associated to surgical drainage contraindications: Worsening of performance status score, hypoalbuminemia and thrombocytopenia, liver and kidney dysfunction. Surgical intervention may be difficult due to the adhesion surrounding liver caused by TACE, it can also lead to tumor spread [4].
Liver abscess is a potentially fatal disease, the mortality rates ranges from 13% to 50% aneven after treatement [5,6]. Fast diagnosis establishment and treatment instauration are the cornerstones of good evolution. It seems that bowel preparation in addition to prophylactic antibiotics (3rd-generation cephalosporin intravenously infused 30 min before TACE) prevent abscess development especially in patient with risk factors [11].
Liver abscess remain a rare complication of TACE for HCC but potentially deadly as reported here. The portal vein thrombosis after TACE can be most likely septic and cruoric rather than neoplastic. The acute hepatic failure represents the natural evolution of the two.
With careful patient selection and evaluation, major complications following hepatic chemoembolization can be avoided or reduced by an adjustment of the TACE protocol and/or post-procedure monitoring. Awareness of these scenarios and their management are critical to perform TACE safely with optimal outcomes.