Dengue fever is a common mosquito borne disease in India. Dengue fever in liver transplant recipient has rarely been described. We report here 3 cases of dengue fever in our liver transplant patients.
Case presentation: We report 3 cases of dengue fever in our liver transplant patients.
Case 1: Presented 3 months after transplantation with history of febrile illness with myalgia, arthralgia, thrombocytopenia, leukopenia. His low platelet and WBC counts were initially attributed to hypersplenism. Dengue was diagnosed using NS1antigen test and he was managed conservatively as for dengue fever. He recovered well and his graft is functioning well till last follow up.
Case 2: Presented 2 years after transplantation with a history of fever, thrombocytopenia, mildly elevated liver enzymes. He had history of biliary stenting for post op anastomotic stricture. Initial diagnosis was suspected to be stent block cholangitis. Dengue Ig M antibody test was negative but NS1 antigen test was positive. Final diagnosis of dengue fever was made. He improved well with conservative management. He is also doing well till last follow up.
Case 3: Presented 8 months after transplant, with fever, myalgia, thrombocytopenia, raised liver enzymes. He was diagnosed as dengue fever - NS1 Ag +, IgM antibody +. He did not required hospitalisation & was managed symptomatically at home, recovered well.
Conclusion: Reports of dengue fever in liver transplant recipients are limited. The presentation may be atypical. It should be suspected when patient present with febrile illness with thrombocytopenia, along with other possible causes. NS1 antigen has better sensitivity than IgM Elisa. Both should be included in diagnostic work up. Dengue fever usually follows a mild course in primary infection and most patients recover well. Dengue fever does not affect graft function in long term.
Dengue fever is a common mosquito borne disease in India. Dengue fever in liver transplant recipient has rarely been described. We report here 2 cases of dengue fever in our liver transplant patients.
A 37-year-old man, who has undergone deceased donor liver transplantation on 26.05.2015, presented again to us with history of high grade fever, 3 months after liver transplantation.
He underwent liver transplantation for hepatitis B virus related cirrhosis with HCC, with added decompensation in form of ascites and intermittent jaundice.
His initial post op course was complicated by intra-abdominal bleeding, for which he was re-explored on post op day 1 and haemostasis was achieved. He received platelet transfusions and inj filgrastim in view of low platelet counts. He recovered satisfactorily and was discharged on 11.07.2015.
1 month later, now, he presented with 1 day history of high grade fever (103 degree), continuous, not associated with chills or rigor, nor rashes/petechiae but associated with myalgia, headache and lethargy. There was no history of jaundice, abdominal pain, pulmonary, bladder or bowel symptoms.
On examination, he was febrile, anicteric, having mild splenomegaly (which was present preoperatively also. He was investigated with hemogram, LFT/KFT, INR, blood culture, urine routine microscopy and culture, malaria and dengue antigen tests, ultrasonography of abdomen and chest radiograph.
His platelets counts were low previous to this febrile illness also, that was attributed to be due to hypersplenism. His last platelets count at previous discharge was 44,000. During this illness, he had further drop in platelets counts, as trend shown in Figure 1.
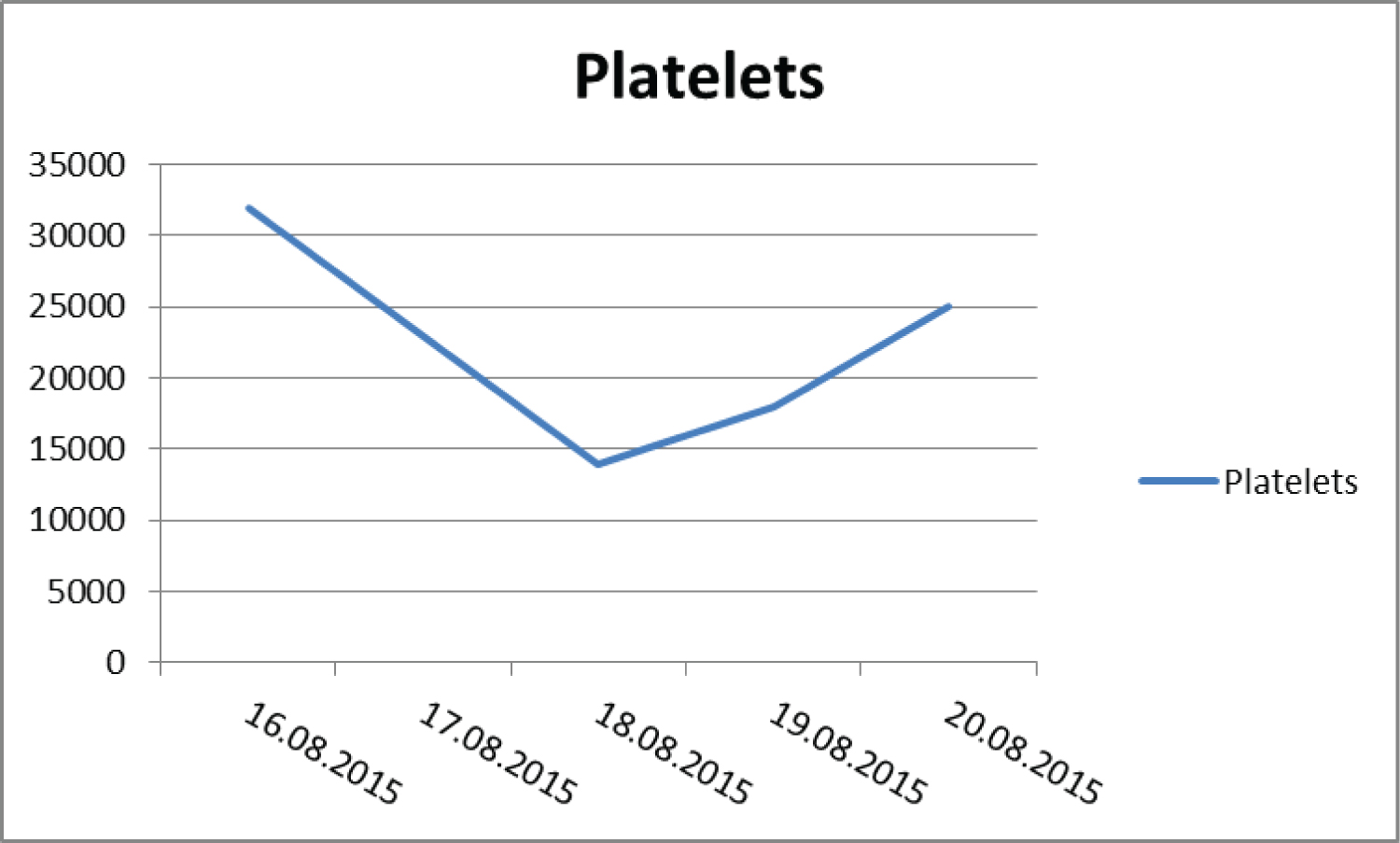 Figure 1: Trend of platelets of case 1.
View Figure 1
Figure 1: Trend of platelets of case 1.
View Figure 1
His TLC was also low (range-1900 to 2600). His LFT showed mildly raised liver enzymes, trend shown in Figure 2.
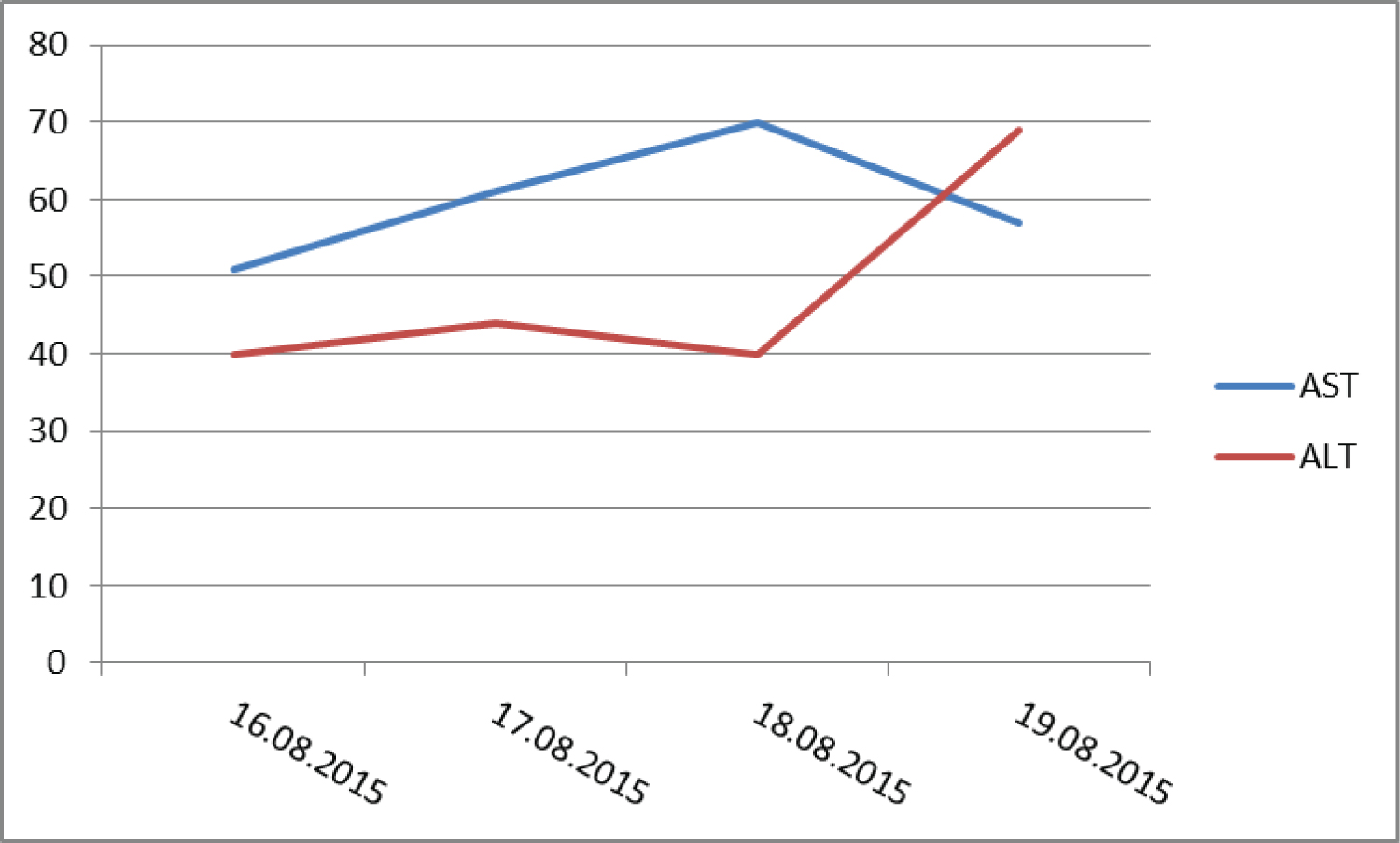 Figure 2: LFT trend of case 1.
View Figure 2
Figure 2: LFT trend of case 1.
View Figure 2
His KFT became mildly deranged. Blood and urine culture was sterile. Chest X-ray was normal. Ultrasound abdomen revealed mildly enlarged liver, no IHBR dilatation, no free fluid in abdomen and normal vascular flow in liver. Mild right pleural effusion was present. His blood for malaria antigen was negative. Dengue NS1 Antigen was positive by ELISA.
He was managed aggressively as per dengue fever protocol. He recovered well and was discharged in 2 weeks.
A 26-year-old man, who had undergone deceased donor liver transplantation in December 2017, for congenital hepatic fibrosis, presented 2 years after ( in October 2019), with history of fever for 5 days. He had high grade continuous fever, relieved with medications, not associated with chills or rigor, not associated with rash, arthralgia. He had mild body ache. He had no history of jaundice. He had no history of cough, cold, burning micturition, frequency of micturition or any pustule/boil.
Examination did not reveal any jaundice, rash or boil. He did not have any abdominal signs or significant finding on chest examination.
He had uneventful post op course after liver transplant. But he developed anastomotic biliary stricture 7 months post transplantation and underwent biliary stent placement.
So, when he presented this time with fever, initial suspicion was of stent block cholangitis and treatment with broad spectrum antibiotic (Magnex, Metronidazole) was started.
On blood investigations, his initial TLC count was 3300 and platelet count was 24000. Serum bilirubin was 0.8 and alkaline phosphatase, AST & ALT was 167, 59 & 36 respectively. KFT was normal. His ultrasonography of the abdomen also showed mild intrahepatic biliary radicals dilatation with pneumobilia.
Initial clinical diagnosis was of acute febrile illness with thrombocytopenia, likely dengue fever or stent block cholangitis with sepsis.
His blood and urine cultures were sterile. Blood work up for malarial parasite was negative. IgM Elisa for dengue was negative but NS-1 antigen for dengue was positive. So, final diagnosis of Dengue fever was made. Stent exchange was deferred. His platelet counts and LFT showed the trend shown in the Figure 3 and Figure 4 respectively.
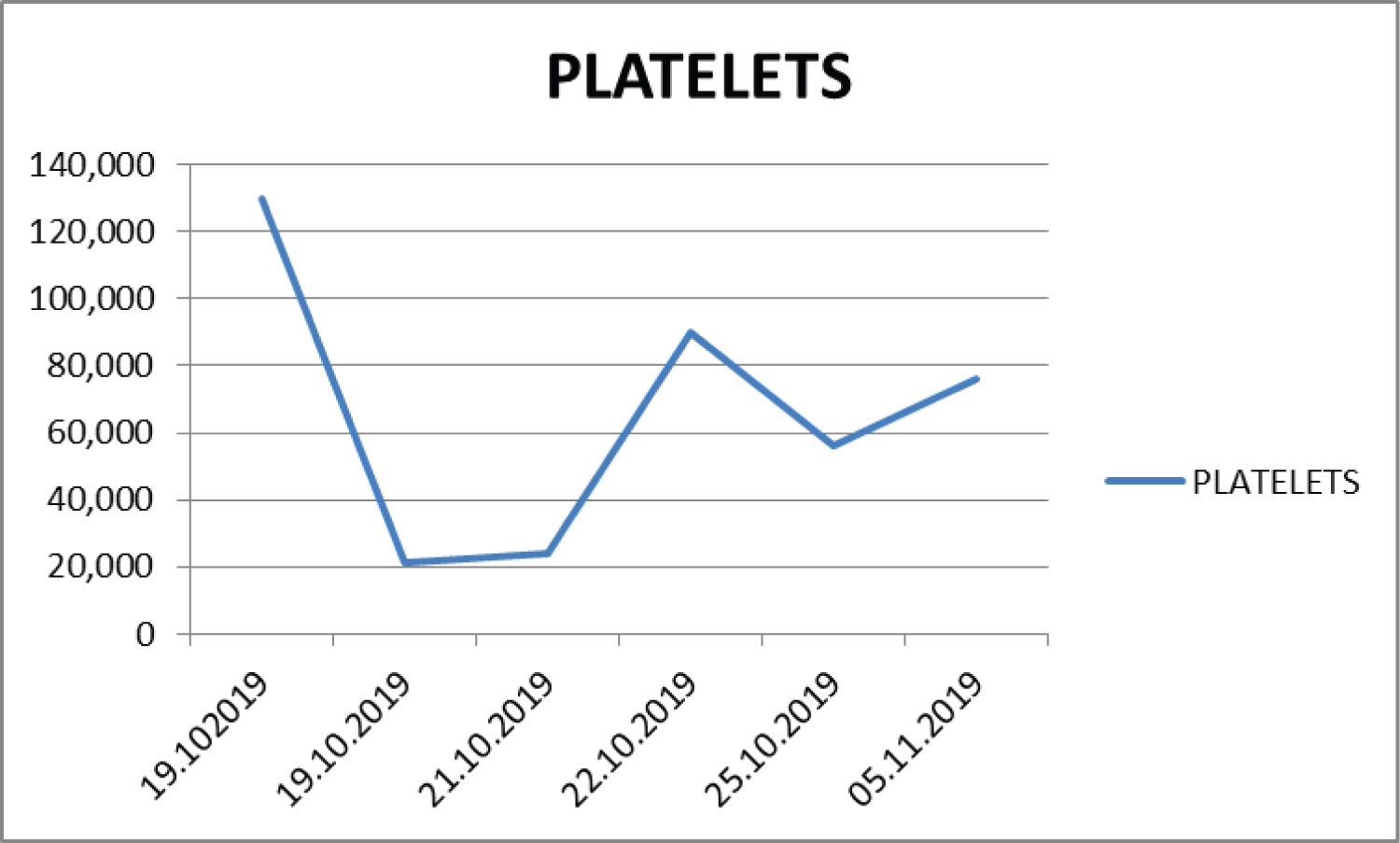 Figure 3: Trend of platelets of case 2.
View Figure 3
Figure 3: Trend of platelets of case 2.
View Figure 3
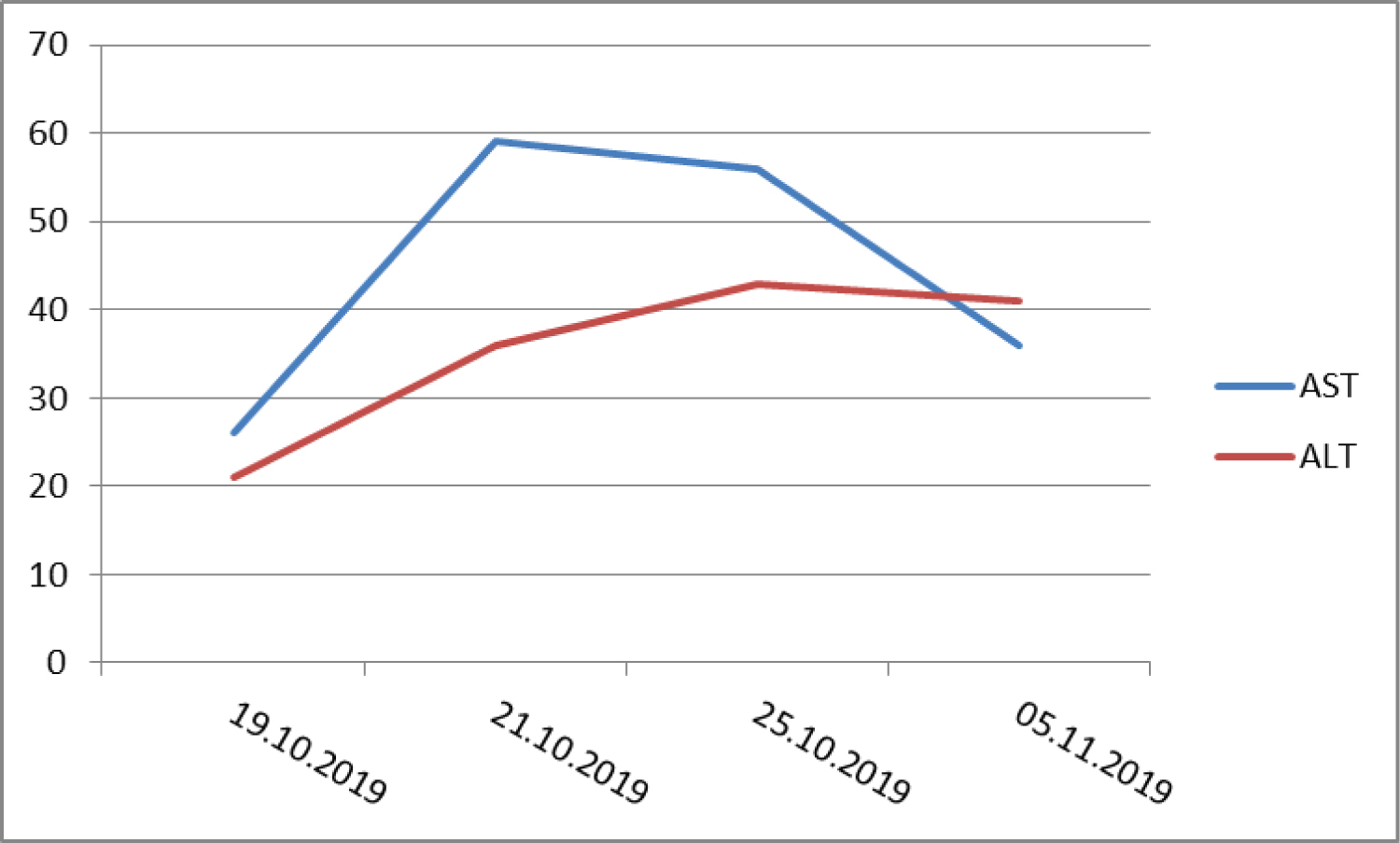 Figure 4: LFT trend of case 2.
View Figure 4
Figure 4: LFT trend of case 2.
View Figure 4
He improved symptomatically with conservative management as standard for dengue fever.
Case 3- A 44 y/male pt, underwent DDLT on 16.02.2020, for alcohol related CLD (MELD- 19), had uneventful post of course, discharged on 21.03.2020. he was maintained on immunosuppression- Tacrolimus 4 mg BD & mycofenolate mofetil 720 mg BD. He had myalgia, malaise with fever on 26.10.20, fever workup was sent (blood & urine cultures, CBC, Lft, Dengue NS1 Ag & IgM antibody, Malaria work up). He was diagnosed as dengue fever- NS1 Ag +, IgM antibody for dengue +.
MMF was stopped in view of decreasing platelet counts; tacrolimus was continued 3.5 mg BD. He was managed as symptomatically as for dengue fever, did not required hospitalisation. His platelet counts trend & liver enzymes trend was as shown below in Figure 5 and Figure 6 respectively.
 Figure 5: Trend of platelets of case 3.
View Figure 5
Figure 5: Trend of platelets of case 3.
View Figure 5
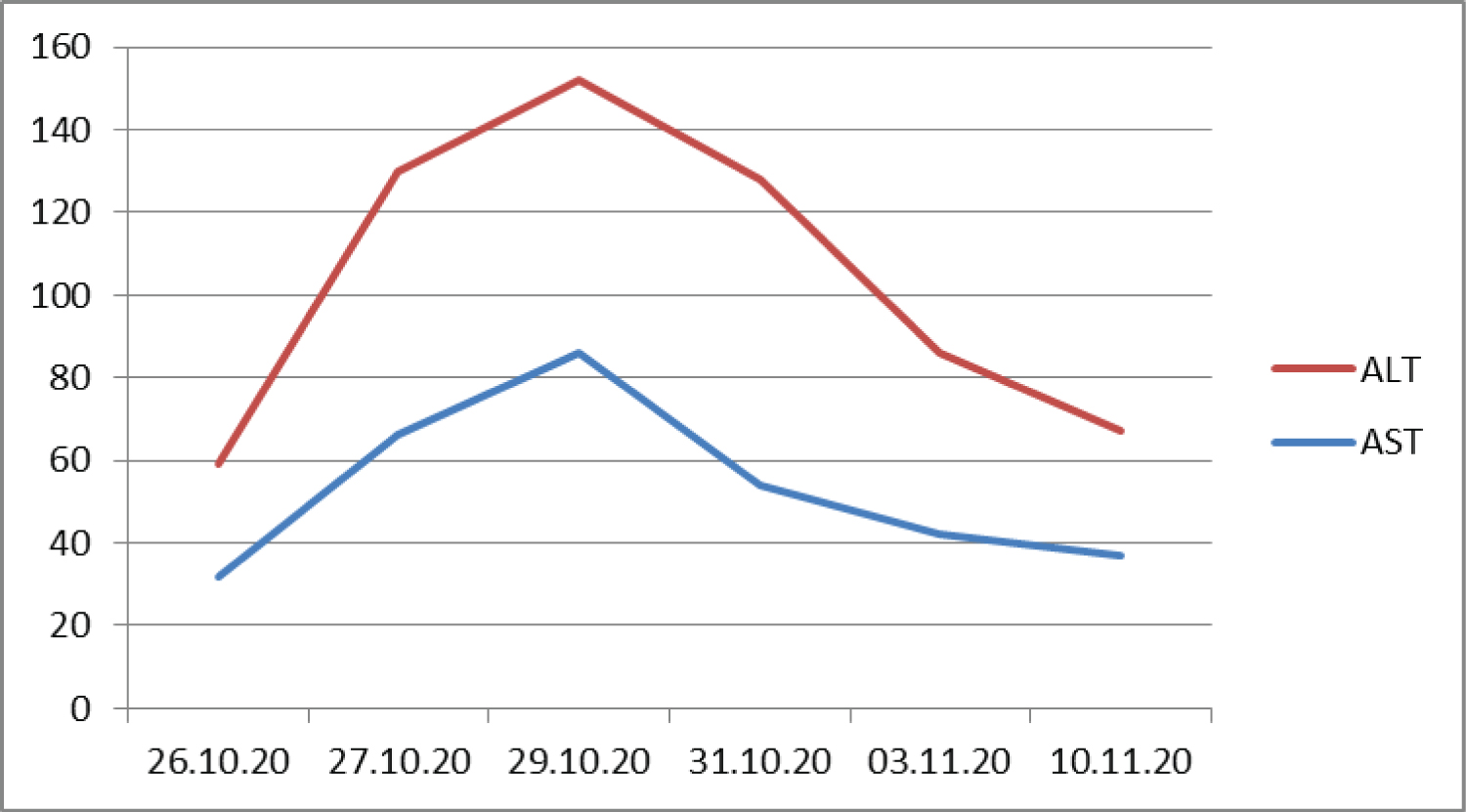 Figure 6: LFT trend of case 3.
View Figure 6
Figure 6: LFT trend of case 3.
View Figure 6
He recovered well & his graft function is also normal till last follow up.
Dengue fever is endemic in India, having a seroprevalence of almost 57% among general population [1]. It is one of
It has been reported rarely in patients who have received organ transplantation, and data of such cases in liver transplant recipients is even more limited. Immunosuppressed transplant recipients have reduced T-cell responses and are thus, at a low risk for DHF and this may account for less clinical reports in such patients [2-4].
The presentation may also be atypical in organ transplant recipients, with resulting low suspicion. Thus, diagnosis may be delayed in these patients and management complicated owing to drug toxicity and interactions [3].
The diagnosis may also be challenging as fever and thrombocytopenia may be initially attributed to more common etiologies like sepsis or CMV infection or early rejection.
Dengue infection follows the same course in transplant recipients as in general population. The incubation period of the virus ranges from 4-10 days [5]. The classic dengue fever (DF) is characterized by the acute onset of high fever, weakness, malaise, headache, myalgia, arthralgia, retro-orbital pain, nausea, and vomiting. The symptoms usually last 1 week. Laboratory findings are nonspecific: Leukopenia, lymphopenia, thrombocytopenia, and slight elevations of hepatic aminotransferases. The severe form of the infection is dengue hemorrhagic fever (DHF), which occurs on a second dengue infection episode with a different virus serotype, characterized initially by the same manifestations and later capillary leakage and shock.
In our cases, one patient had these classical findings while other had only fever and thrombocytopenia. None of the patients had hypotension and both recovered well.
The source of dengue virus is mostly vector borne (mosquito bite), but non-vector borne sources such as transmission from donor organ or through blood transfusion [6] have also been reported, albeit rare. Transmission of dengue virus through donor organ has been reported in live related liver transplantation [7-9] as well as from deceased donor liver transplant.
Thus, in endemic regions, it is important to suspect and screen for dengue in febrile and thrombocytopenic recipients in the postoperative period.
Rosso, et al. [10] has described a series of 4 patients documenting dengue transmission through organ transplantation. All patients develop symptoms during the first week post-transplant. Fever and thrombocytopenia were the most frequent findings. There are no reports of graft rejection among dengue infected cases.
But donor organ or blood as a source were excluded in both our patients as they presented 3 months and 2 years after transplant respectively. The likely source is thus vector borne only.
The commonly used diagnostic tests to diagnose dengue include IgM Elisa Antibody test, NS1 antigen test and RTPCR. NS1 is essential for viral replication [11], and the amount of secreted NS1 (sNS1) in the serum has been shown to directly correlate with viremia [12], NS1 antigen is detectable as early as day 1 of fever by enzyme-linked immunosorbent assay (ELISA), and the detection is not affected by the presence of anti-dengue immunoglobulin M (IgM) antibodies. NS1-based ELISAs may be an important diagnostic tool for those samples in which IgM is not detectable and for which PCR is not available [13-15].
In our patient also, we detected dengue on NS1 antigen test, while IgM ELISA was negative in two.
DF seems to cause no long-term damage to the patient and to the graft. Both our patients recovered well and are doing fine till date.
Reports of dengue fever in liver transplant recipients are limited. The presentation may be atypical. It should be suspected when patient present with febrile illness with thrombocytopenia, along with other possible causes. NS1 antigen has better sensitivity than IgM Elisa. Both should be included in diagnostic work up. Dengue fever usually follows a mild course in primary infection and most patients recover well. Dengue fever does not affect graft function in long term.