Rationale: Lupus nephritis, a complication of systemic lupus erythematosus, can progress to end-stage kidney disease, often portends a poor prognosis. A kidney biopsy is very essential in cases of symptom overlap as it guides in formulating an effective treatment regimen.
Patient concerns: Patient had generalized edema, difficulty with breathing, anemia, vomiting and hiccups.
Diagnosis: Histology-confirmed class VI lupus nephritis.
Interventions: She was managed using an overlapping treatment spanning classes IV-VI, with maintenance haemodialysis (MHD), mycophenolate mofetil, methylprednisolone and diuretics. This was based on the heightened disease activity and extrarenal manifestations which the World Health Organisation (WHO) and the International Society of Nephrology/Renal Pathology Society (ISN/RPS) revised guidelines classified as active disease, and for which the Kidney Disease Improving Global Outcome (KDIGO) guideline for glomerulonephritis recommended aggressive treatment for classes III and IV, and class V with nephrotic syndrome, with high dose corticosteroids, cyclophosphamide or MMF for induction therapy, with low dose corticosteroid and MMF for maintenance therapy. KDIGO also recommended that class VI disease (as in index patient) should be managed as an ESKD for which she commenced maintenance haemodialysis.
Outcome: Disease went remission, clinical symptom got resolved and she continued outpatient MHD.
Learning point: The case highlights the place of kidney biopsy in the management of LN, and possible complexities associated with disease staging, and the overlap of symptoms and signs, and how this should guide the treatment regimen to achieve optimal results.
Case report, Lupus nephritis, Systemic lupus erythematosus, Histology, Kidney biopsy, Remission, Relapse, Haemodialysis
Systemic lupus erythematosus (SLE) is aautoimmune, multisystemic clinically heterogeneous disease characterized by circulating autoantibodies directed against nuclear antigen [1]. The disease is more prevalent in women, Africans and in the reproductive age group, with more than 85% of victims being younger than 55 years. Males, children and the young tend to have more severe forms of disease [1]. The incidence and prevalence of SLE range from 0.3-8.7 per 100,000 persons and 3.2 to 159 per 100,000 persons, respectively [2]. A high concordance rate in monozygotic twins, the significantly high percentage (17%), of affectation of relatives, the higher frequency of HLA genotypes particularly, B8, DR 2 , DR 3 and DQW 1 , and the higher frequency of the disease in populations with deficiency of complements factors C1q, C 2 and C 4 all led credence to a genetic predisposition [3]. Hormonal and environmental factors have also been implicated in its aetiology [1-3].
Lupus nephritis (LN) frequently complicates SLE, often developing concurrently or shortly following the onset of SLE, and results from glomerular immune complexes deposition and often runs a protracted course with periods of remission and exacerbations, and clinical renal manifestations often correlates with the degree of glomerular involvement [4]. Progression to end-stage kidney disease (ESKD) requiring renal replacement therapy (RRT) is common [2,3]. We present the case management of a 45 year old woman with LN who successfully had class and symptom overlap treatment.
A 45-year-old woman presented at the emergency session with a 4 month history of recurrent difficulty with breathing, 2 month of leg swelling and a month of skin excoriation. Dyspnea was initially with physical activity but progressed to its occurrence at rest. She had orthopnoea, paroxysmal nocturnal dyspnea (PND) and cough productive of frothy sputum. She had no haemoptysis nor night sweats. Symptoms temporarily subsided with treatment at a peripheral hospital. She also had right hypochondrial pain with progressively worsening vomiting, anorexia and body weakness. She first had had non-pruritic skin excoriations at 30 years, and subsequently had scalding, and patchy hair loss. The facial rashes were worse and peppery outdoor, under the sun. She had recurrent episodes of low grade fever, arthralgia, without joint swellings, but had no urinary symptoms. She was diagnosed hypertensive at 35 years and had been on daily doses of amlodipine 10 mg, frusemide 40 mg and spironolactone 25 mg. She had a recent diagnosis of systemic lupus erythematosus (SLE) at a peripheral facility while being managed for pericardial and pleural effusion, for which she had chest tube insertion and pericardiocenthesis. She has had waxing and waning episodes in the course of the illness.
She was pale, not jaundiced, acyanosed, febrile (37.9 °C) and oedematous. She had a dark scaly rash over the bridge of the nose sparing the nasolabial folds, scarring alopecia with discoid patches, and hyperpigmented popular lesions on the limbs and trunk. Her blood pressure 119/82 mmHg, respiratory rate was 24/min, and oxygen saturation was 96% in room air. The breath sounds were reduced in both lung bases, but there were no significant findings on abdominal examination.
Lupus nephritis, complicated by anasarca with pleural effusion, with resolving serositis.
Bedside urinalysis showed protein 3+, nitrites 1+, and leucocytes 1+. 24 hour urine protein was 3.8g. Electrocardiogram (ECG) showed sinus rhythm with low voltage complexes (Table 1).
Table 1: Serum laboratory results all through admission. View Table 1
Echocardiogram showed pericardial effusion with severe concentric left ventricular hypertrophy (LVH). Chest X-ray showed cardiomegaly with right and left atrial enlargement. Urine culture yielded growth of E. coli sensitive to ceftriaxone, gentamycin andceftazidime. Blood culture yielded growth of Staphylococcus aureus sensitive to amoxicillin, clindamycin and erythromycin. Serological screenings were negative for HIV and hepatitis B, and C viruses. Antinuclear antibodies (ANA) were positive, with speckled pattern, and double stranded DNA (dsDNA) was negative. Antinuclear neutrophil cytoplasmic antibodies (ANCA) were both negative (cytoplasmic and perinuclear). Kidney scan showed right kidney (9.81 × 4.13), and left kidney (9.3 × 4.51), both showed obliterated cortico-medullary differentiation, and increased parenchymal echogenicity. The glomerular filtration rate (eGFR) at presentation 11.7 mL/min/1.73 2 . She had her first haemodialysis session via a central venous catheter, she received 2 units of blood, and was commenced on the following drugs:
Intravenous (IV) Methylprednisolone succinate 500 mg daily for 3 days then,
Tab Prednisolone 60 mg daily (from 4DOA); Tab Mycophenolatemofetil 1g bd;
Tab Hydroxychloroquine 400 mg daily; IV Ceftriaxone 1g bd;
Tab Frusemide 80 mg bd; Tab Amlodipine 10 mg daily, and Tab Lisinopril 10 mg daily.
The pericardial effusion was mild and did not require pericardiocentesis.
Her condition improved, an arterovenous fistula (AVF) was created, and she was subsequently discharged on her medications. At discharge, she was commenced on subcutaneous Erythropoietin 75 µg monthly. She is still being followed up at the nephrology outpatient clinic with twice weekly haemodialysis at the dialysis centre and has remained stable.
Advanced global glomerulosclerosis, with diffuse glomerulosclerosis (> 90% global sclerosis) representing healing of previously inflamed tissues. Advanced tubulointerstitial disease, with tubular atrophy and interstitial fibrosis. Atrophic tubules contain PAS-positive hyaline casts, some small atrophic tubules without prominent lumen. Marked interstitial inflammatory cellular infiltration.
Stage VI Lupus nephritis with resolving serositis (Figure 1).
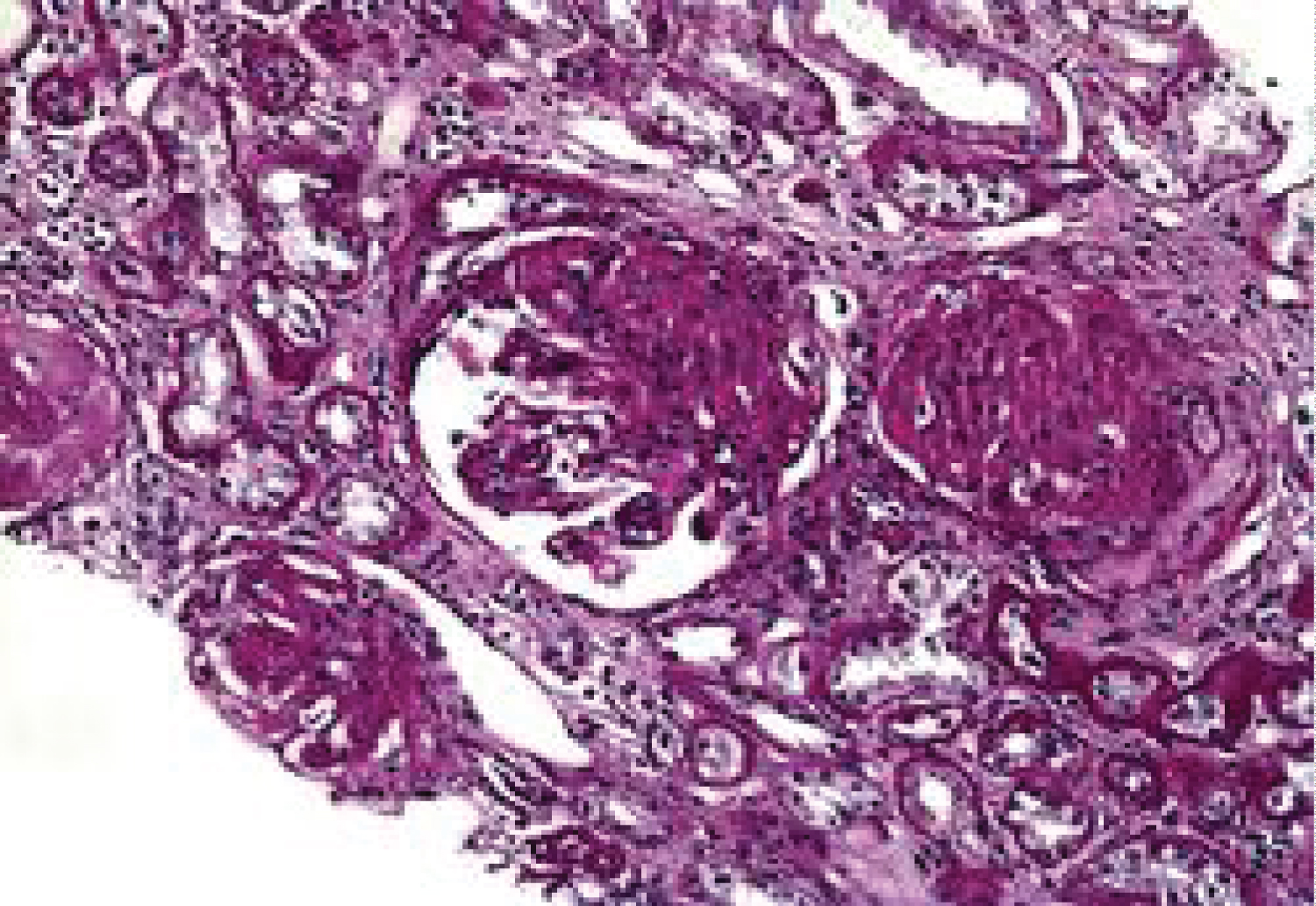 Figure 1: Photomicrograph showing lupus nephritis class VI with advanced sclerosing glomerular disease and tubular atrophy (x300).
View Figure 1
Figure 1: Photomicrograph showing lupus nephritis class VI with advanced sclerosing glomerular disease and tubular atrophy (x300).
View Figure 1
Systemic lupus erythematosus (SLE) is a multisystemic, autoimmune, clinically heterogeneous disease typified by circulating autoantibodies directed against nuclear antigen [1,2].
Lupus nephritis (LN) is a frequent and potentially serious complication of SLE [4]. The disease is more prevalent in women Africans and in the reproductive age group with more than 85% of victims being younger than 55 years, as was the case with index patient [1]. Lupus nephritis tends to be more severe in young adults than the elderly, as seen in the index case [1]. Adelowo, et al. [5] reported a prevalence of 5.28% with females constituting 95.5%, with a mean age of 33 years (17-55 years). The authors also reported a 25-50% of LN among the SLE population [5].
Abnormities of immune regulation with loss of self-tolerance and subsequent auto immune response characterizes SLE [1,3]. This is associated with reduced levels of circulating cytotoxic and T-Suppressor cells, increased helper T-Cells, polyclonal activating B cells, defective B-cell tolerance, dysfunctional T-cell signaling and abnormal Th1 and Th2 cytokine production [2,4].
Renal involvement often develops within 3-5 years onset of SLE and may follow a protracted course with periods of remission and exacerbations [4]. Clinical renal involvement usually correlates well with the degree of glomerular involvement [6].
Lupus nephritis exhibits a pleomorphic histopathologic pattern, and can transform between patterns spontaneously or with treatment [6]. The World health Organisation (WHO) and the International Society of Nephrology/Renal Pathology Society (ISN/RPS), in the revised form, classified LN into six stages: Class I as minimal mesangial immune complex deposition; class II as mesangial proliferative disease; class III as focal proliferative LN with < 50% of glomerular affectation; class IV as diffuse proliferative LN with > 50% of glomerular affectation; class V as membranous LN, and class VI as advanced sclerosing LN [7].
Considering the acute flare, the clinical state of the index patient, the possibility of an active disease was envisaged, hence she was managed empirically with methylprednisolone, mycophenolate mofetil (MMF) and haemodialysis prior to tissue diagnosis. The Kidney Disease Improving Global Outcome (KDIGO) guideline for glomerulonephritis recommended aggressive treatment for the active disease (classes III and IV), with high dose corticosteroids and cyclophosphamide or MMF for induction therapy, and low dose corticosteroid with azathioprine or MMF for maintenance therapy [8]. KDIGO recommended the same regimen for Class V disease persisting with nephrotic syndrome, but with an option of a calcineurin inhibitor (CNI). For classes I and II, KDIGO recommended conservative management, or with steroids or an immunosuppressant, as determined by extra renal manifestations. Its recommendation that class VI disease should be managed as an ESKD explains why the long term management plan for the index patient was by haemodialysis and a possible kidney transplant.
The patient presentation with nephrotic range proteinuria and ESKD (eGFR 11.7 mL/min/1.73 m 2 ) places her in KDIGO stage V or VI of the clinical practice guideline for glomerulonephritis [9]. We felt she had class V LN (membranous glomerulonephritis) on account of the anarsaca, with pericardial effusion that is more likely to be seen in this stage. Moreover, urinalysis showednephrotic range proteinuria. Her GFR of 11.7 mL/min with obvious uremic symptoms typifies her condition as class VI lupus (advanced sclerosis), hence in keeping with KDIGO guidelines, we commenced her on prednisolone 60 mg daily (high dose) and MMF 1g twice daily (induction phase), even though immunosuppressive drugs are commonly not used in stage VI lupus nephritis except with situations such as declining kidney function, presence of extra renal manifestations such as pericardial effusion(both present in index patient), or a histology-confirmed proliferative disease [9,10]. Hydroxychloroquine, as used in this case, have been documented to reduce flarerates, as reported from a prospective controlled trial where those who continued hydroxychloroquine had lower flare rates compared with those switched to placebo [5].
In conclusion, LN represents a major burden and cause of morbidity and mortality in patients with SLE. A high index of clinical suspicion is required to make an early diagnosis, and entails periodic screening for proteinuria and blood pressure measurement. Prompt treatment with corticosteroids or other immunosuppressive agents can be cost effective, achieve remission, and retard progression to ESKD. Though the biopsy showed advanced sclerosis, of which haemodialysis is the main stay of treatment, the presence of proteinuria, strengthened our use of corticosteroids and immunosuppressants to which our patient showed favorable clinical response. The case highlights the place of kidney biopsy in the optimal management of LN as it specified the disease class, and highlighted possible complexities that could arise in disease staging, and overlap of symptoms, signs and treatment.
All authors contributed equally to the study.
We thank the nurses for their contribution to patient’s management.
None.