Renal disease is an important non-communicable disease in India. Lack of awareness, late diagnosis, less accessibility and higher costs for renal replacement therapy have led to increased morbidity and mortality. Though the common view of no or less awareness among rural population of India is true to some extent, awareness about renal diseases is low even in urban people. We decided to address the 'kidney health' of urban population of Chennai on the occasion of World Kidney Day 2020 the theme of which was Kidney Health for Everyone Everywhere - from Prevention to Detection and Equitable Access to Care. We conducted a kidney health screening camp at Chetpet, Chennai on March 9th 2020 where we checked blood pressure, urine albumin, blood urea, serum creatinine and random blood sugar for 253 people who were regular walkers. The mean age of the population was 53.4 yrs in which the prevalence of diabetes mellitus was 29.2%, systemic hypertension in 26.1%. We also identified elevated serum creatinine in 0.9% of the subjects. The results of the study show the high prevalence of diabetes and hypertension which are the major risk factors for chronic kidney disease in seemingly "healthy" population. The study also points towards the need for screening the population for asymptomatic renal diseases by means of blood pressure monitoring, albuminuria and serum creatinine estimation which can be used as inexpensive tools for preventing major renal diseases. We also highlight the need for more public awareness regarding kidney health and the need to improve kidney health in India.
World kidney day, Kidney health screening, Urban population
The Declaration of Alma-Ata stated 'the need for urgent action by all governments, all health and development workers, and the world community to protect and promote the health of all the people of the world' [1]. Chronic kidney disease (CKD) belongs to the category of non-communicable diseases (NCDs) and according to World Health Organization NCDs kills 41 million people each year, equivalent to 71% of the deaths globally [2]. There is limited information available about the 'state of kidney health' in India. In western countries, diabetes and hypertension account for over 2/3rd of the cases of CKD [3]. In India too, diabetes and hypertension today account for 40-60% cases of CKD [4]. The age-adjusted incidence rate of end-stage renal disease (ESRD) in India was reported to be 150 per million population and > 100,000 new patients enter renal replacement programs annually in India [5]. In a recent multicentre study in India, the prevalence of CKD was observed to be 17.2%, with about 6% having CKD stage 3 or worse [6]. These reports suggest that much needs to be done to focus on kidney diseases in India. Effective screening and preventive strategies for NCDs especially diabetes and hypertension along with screening for asymptomatic renal diseases are cornerstones of success in achieving good kidney health.
Detection of CKD, particularly at early stages, is essential because therapeutic interventions are likely to be effective if they are implemented early in the course of the disease process [7]. At present prevention of CKD progression plays an important role across the globe in reducing economic impact. This can decrease the economic and social burden of kidney diseases and reduce the high morbidity and mortality associated with CKD. The prevalence of CKD in different populations, including the high-risk groups needs to be explored among various racial groups and in different environmental situations. There is an urgent need to draft preventive health policies and plan for the allocation of more resources to improve kidney health in India.
The objective of our study was to screen the apparently healthy urban population for asymptomatic renal diseases and to spread awareness regarding kidney health in this population.
This was a cross sectional observational study was conducted on March 9th, 2020 as a part of world kidney day (second thursday of march) in Eco Park, Chennai, India. Participants were informed about the kidney health screening program by means of pamphlets and banners prior to the proposed date. On the day of the camp all the walkers who came to the Eco park from 6 a.m. to 8 a.m. were screened by a team of 8 nephrologists by means of history taking - clinical questionnaire, clinical examination-weight, pulse rate, blood pressure measurements. Laboratory tests which included urine routine, random blood sugar, blood urea and serum creatinine were also done.
The aims of this study were:
1. To determine the prevalence of hypertension, diabetes mellitus among the healthy urban population,
2. To screen for asymptomatic renal diseases in this population and,
3. To spread awareness regarding kidney health in the urban population.
Blood pressure measurements were carried out by nephrologists using a mercury sphygmomanometer. Systolic blood pressure (SBP) was based on the 1st Korotkoff phase and diastolic (DBP) on the 5th Korotkoff phase. Mercury sphygmomanometer was used after checking for zero error. After rest for 5 minutes, BP was recorded in the sitting position in the right arm supported at heart level, with the feet on the floor, to the nearest 2 mm using mercury sphygmomanometer. An average of two readings was taken into consideration. Hypertension was defined as systolic blood pressure ≥ 140 mmHg and or diastolic blood pressure ≥ 90 mmHg as per the ESC/ESH (European society of cardiology/European society of hypertension) recommendations.
Urine samples were collected in sterile universal specimen bottles using the mid-stream clean catch urine sample collection method. Clear instructions were given all subjects on how to collect their urine sample. Men were instructed to clean the opening of the urethra (tip of the penis) with a wet swab containing chlorhexidine gluconate (disinfectant) provided by the researchers. Women were instructed to clean the area around the urethra in the perineum from the front to the back, with the disinfectant. Then they were asked to spread the labia of the external genitalia and wipe again from the front to the back. After the urethra has been properly cleaned, both male and female subjects were then asked to void the initial stream of urine into the toilet. While the process of urination continued uninterrupted, they were then asked to collect 10 ml of urine in the sterile specimen bottle. Once an adequate amount was collected, the remaining urine was voided into the toilet.
The urine dipstick is a semi-quantitative rapid method used to analyse urine. This was carried out using the Urinalysis Reagent Strips We tested specifically for proteinuria, glucosuria. The dipstick is a thin plastic strip which has several small squares of different colours attached to it with each square measuring about a quarter of an inch. The dipstick was inserted into the urine samples for 30-60s and then compared with the colour chart on the strip bottle for interpretation.
Protein: The test zone is buffered to a constant pH value and changes colour from yellow to greenish blue in the presence of albumin. A reading of trace,1+,2+ and 3+ correspond to albumin concentrations of around 30 mg/dl, 100 mg/dl, 300 mg/dl, 1000 mg/dl respectively.
Glucose: The detection is based on glucose-oxidase/peroxidase chromogen reaction.
Non-fasting blood samples were collected in the camps. Blood was analysed in renal lab, department of nephrology, government Kilpauk Medical College and Hospital, Chennai. Blood urea was measured using enzymatic UV kinetic test on an AUTORA ROBNIK analyser. Serum creatinine was measured using Jaffe kinetic method on an AUTORA ROBNIK analyser. Plasma glucose was measured by the glucose oxidase peroxidase method using AUTORA ROBNIK analyser.
High blood pressure was defined according to the ESC/ESH (European society of cardiology/European society of hypertension) as blood pressure of ≥ 140 mmHg systolic and/or ≥ 90 mmHg diastolic [8].
High random blood sugar values were according to the ADA (American Diabetes Association) criteria of random blood sugar value of ≥ 200 mg/dl [9].
Normal serum creatinine was taken to be the standard definition of 0.6-1.1 mg/dl in women and 0.7-1.3 mg/dl in males.
A total of 253 subjects, 194 (76.7%) males and 59 (23.3%) females were encountered in the study. The mean age of the study population was 53.4 yrs, with a mean age of 54.5 yrs in males and 49.9 yrs in females. The most common age group encountered was between 51-60 yrs -26.1%. The prevalence of diabetes mellitus in the study population was 74 (29.2%) and the prevalence of systemic hypertension was 66 (26.1%). Subjects with a previous history of diabetes mellitus alone was 43 (16.9%), subjects with previous hypertension alone was found to be 35 (13.8%), patients with both diabetes and hypertension was 31 (12.3%). We detected high blood pressure in 23 (9.1%) patients of which 10 (3.9%) had underlying diabetes mellitus (Figure 1, Figure 2 and Figure 3).
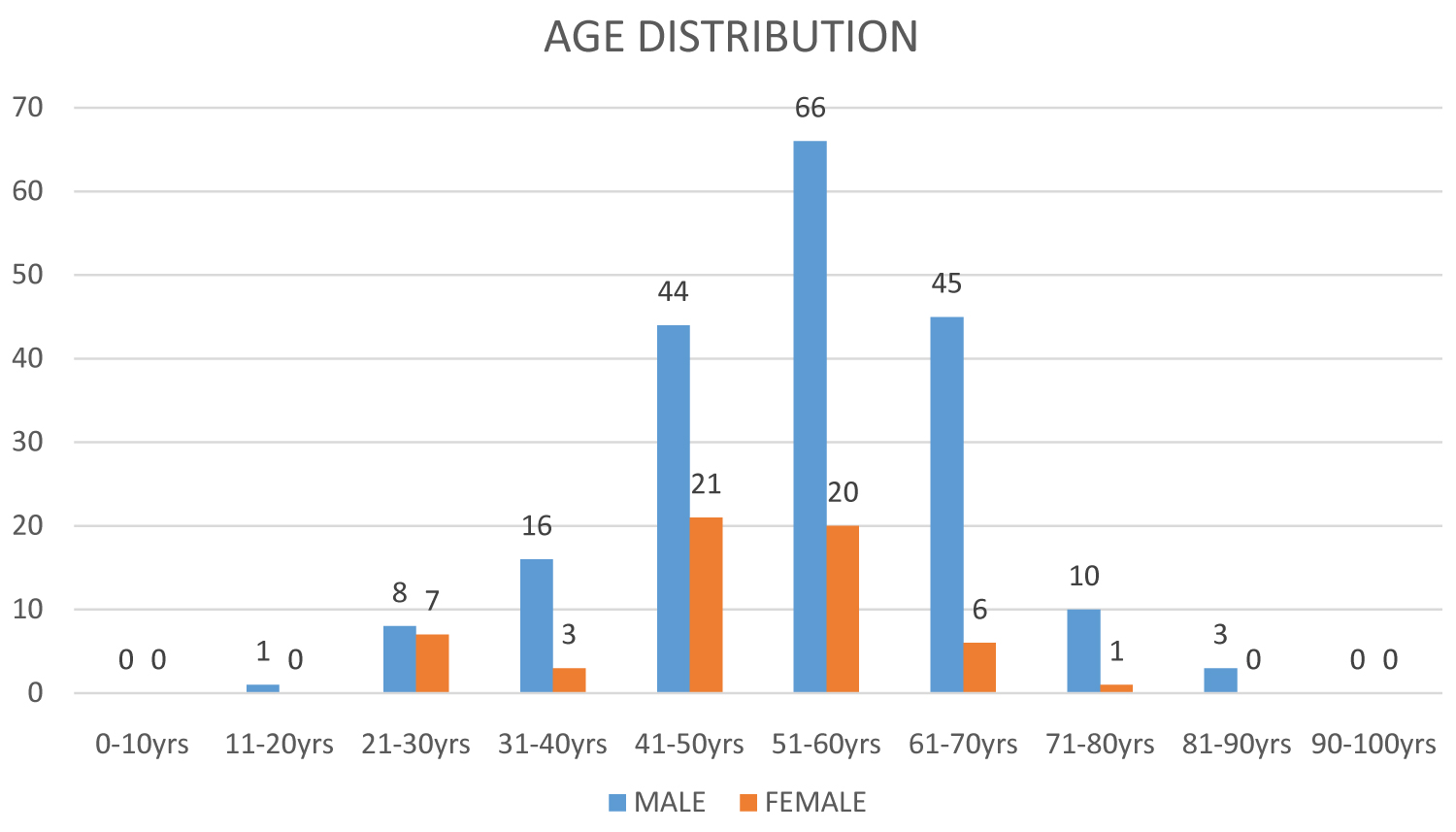 Figure 1: Age wise distribution of the study population.
View Figure 1
Figure 1: Age wise distribution of the study population.
View Figure 1
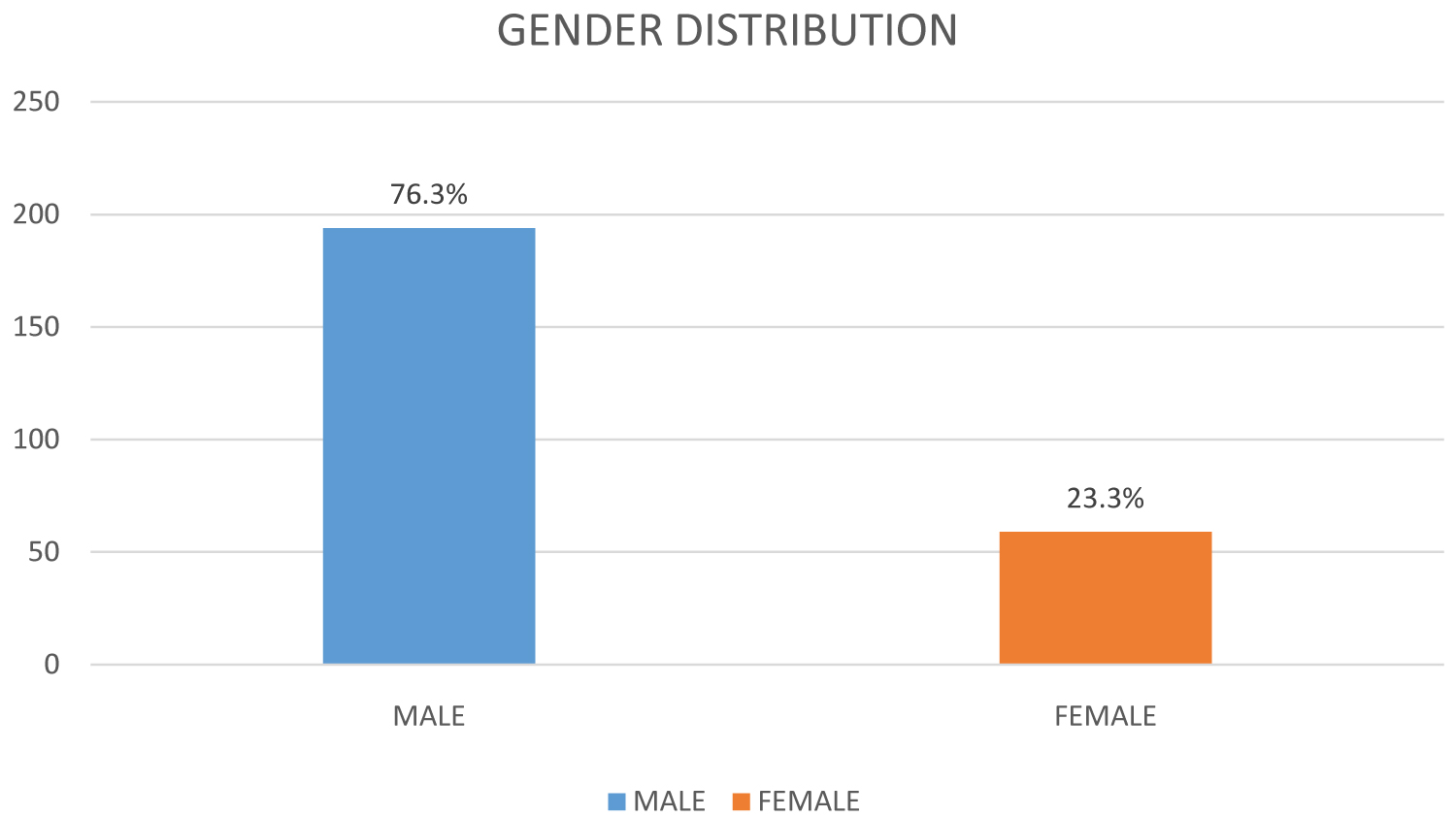 Figure 2: Gender wise distribution of the study population.
View Figure 2
Figure 2: Gender wise distribution of the study population.
View Figure 2
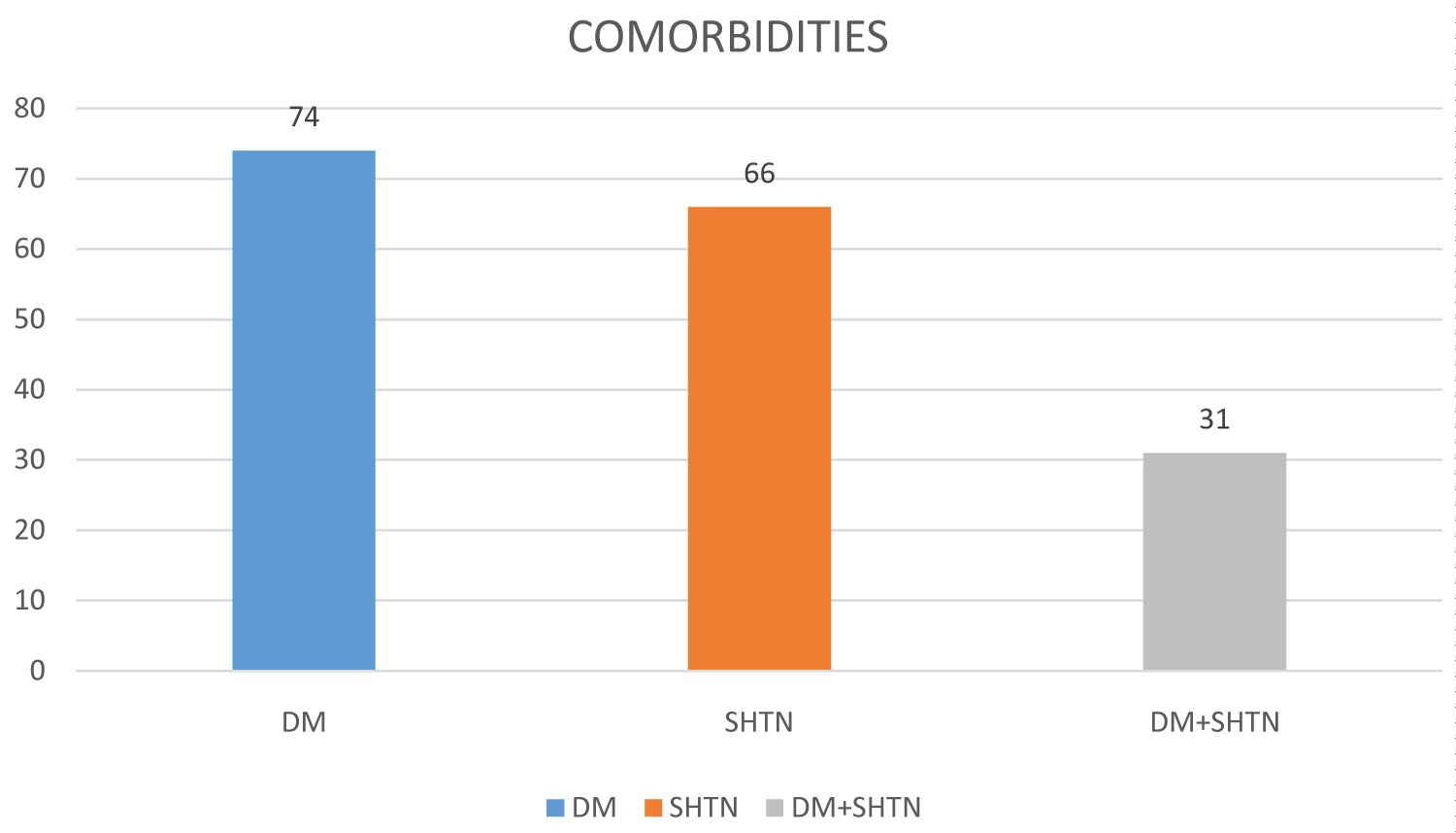 Figure 3: Comorbidities in the study population.
View Figure 3
Figure 3: Comorbidities in the study population.
View Figure 3
Systemic hypertension was seen in 66 (26.1%) of the study population, 31 (12.3%) subjects had systemic hypertension with diabetes mellitus. We were able to identify new onset of high blood pressure in 23 (9.1%) subjects in total 10 (3.9%) of whom had underlying diabetes mellitus.
Out of the 253 subjects studied, 11 patients refused blood and urine sample collection, 10 patients refused urine sample collection and 1 patient refused blood sample collection. So out of the 253 subjects studied, we have taken 232 urine samples and 236 blood samples.
Urinalysis revealed albuminuria in 3 (1.3%) subjects out of the 232 samples analysed. None of the subjects had any underlying diabetes or hypertension (Figure 4).
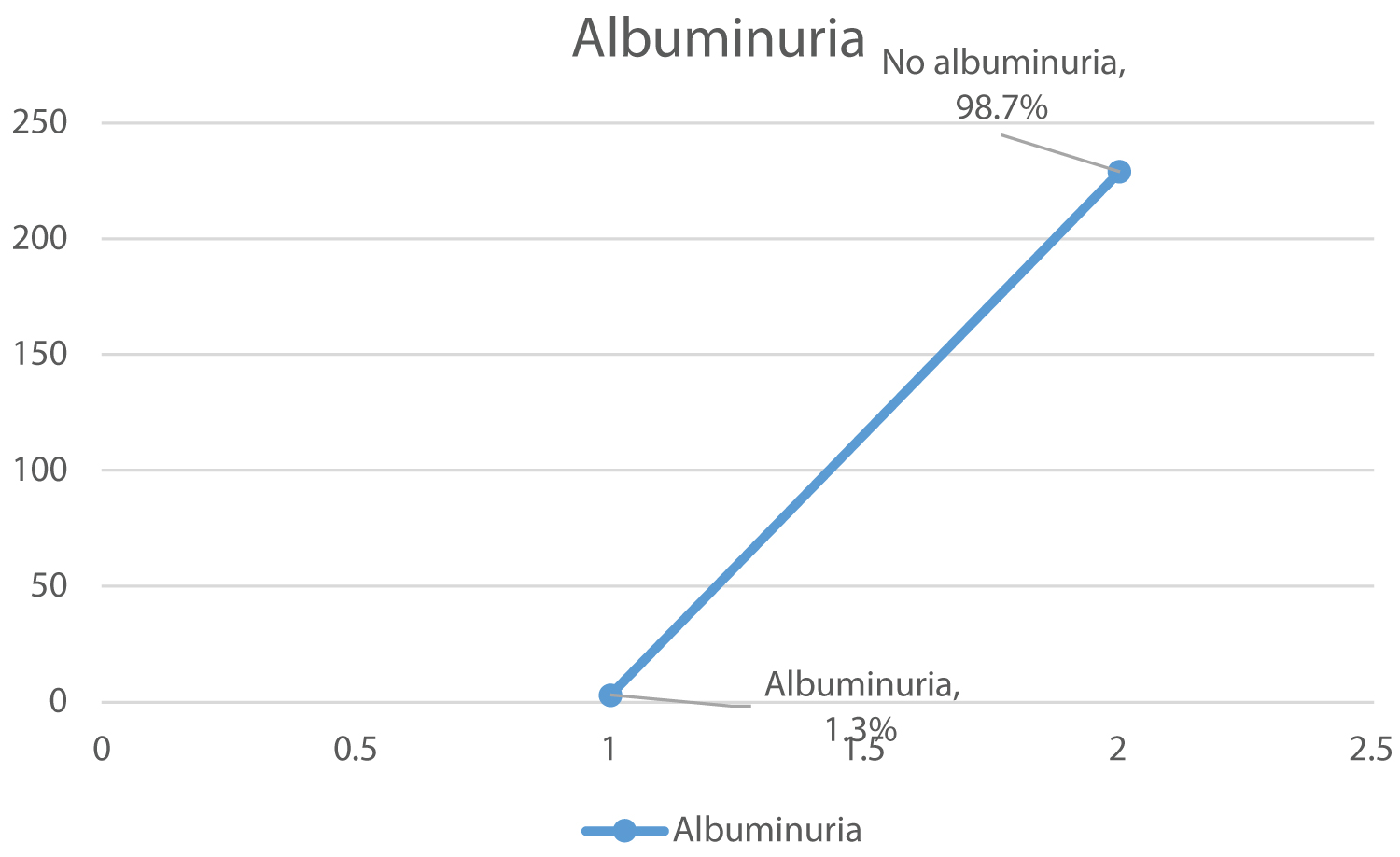 Figure 4: Albuminuria in the study population.
View Figure 4
Figure 4: Albuminuria in the study population.
View Figure 4
Glucosuria was identified in 15 (6.5%) subjects out of 232 samples tested, 3 (1.3%) of them were newly diagnosed without any underlying diabetes mellitus whereas 12 (5.2%) of them had underlying diabetes mellitus (Figure 5).
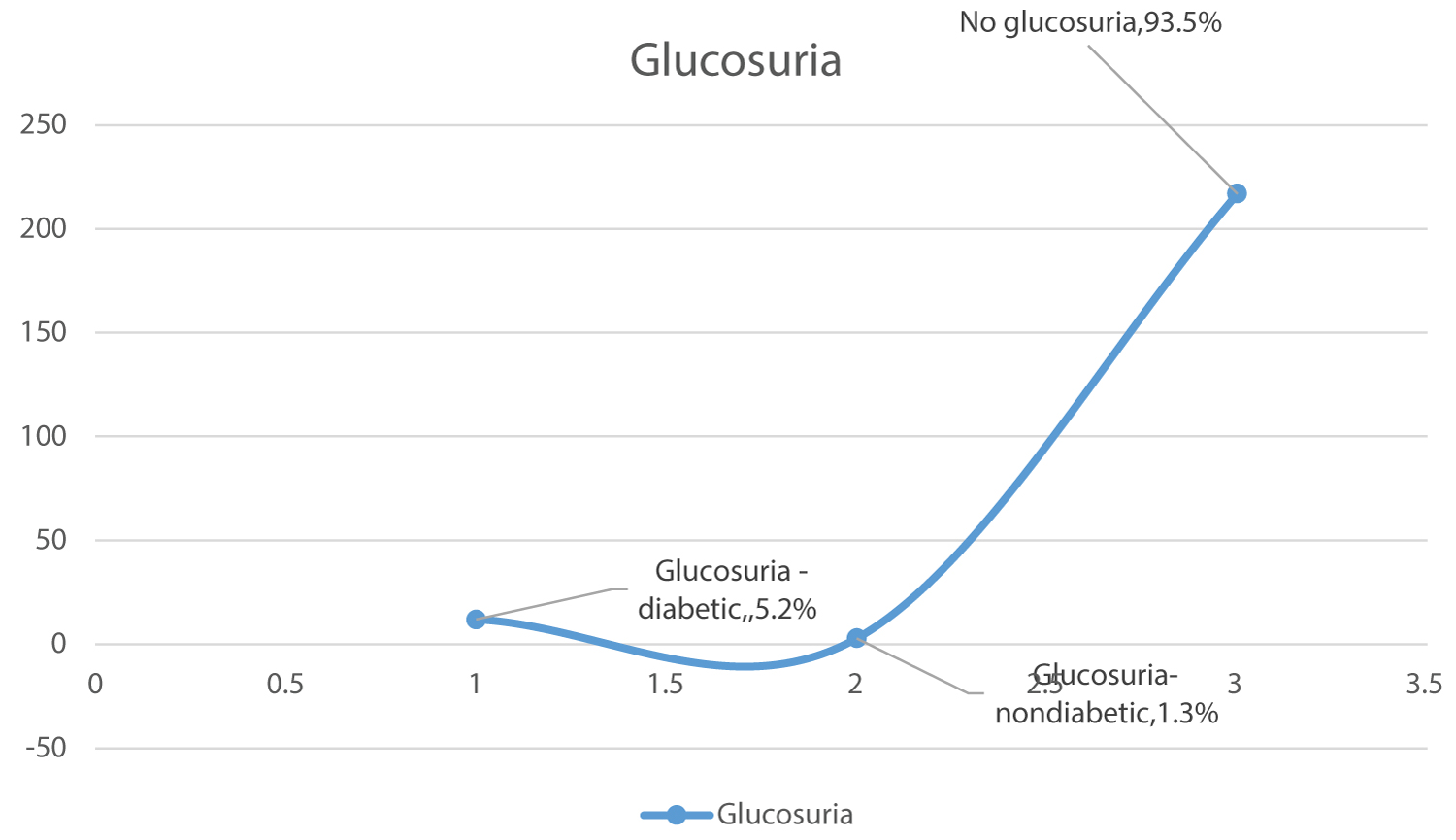 Figure 5: Glucosuria in the study population.
View Figure 5
Figure 5: Glucosuria in the study population.
View Figure 5
We identified high random blood sugar levels in 20 (8.5%) subjects out of the 236 samples analysed with 11 (4.7%) of them having previous history of diabetes mellitus (Figure 6).
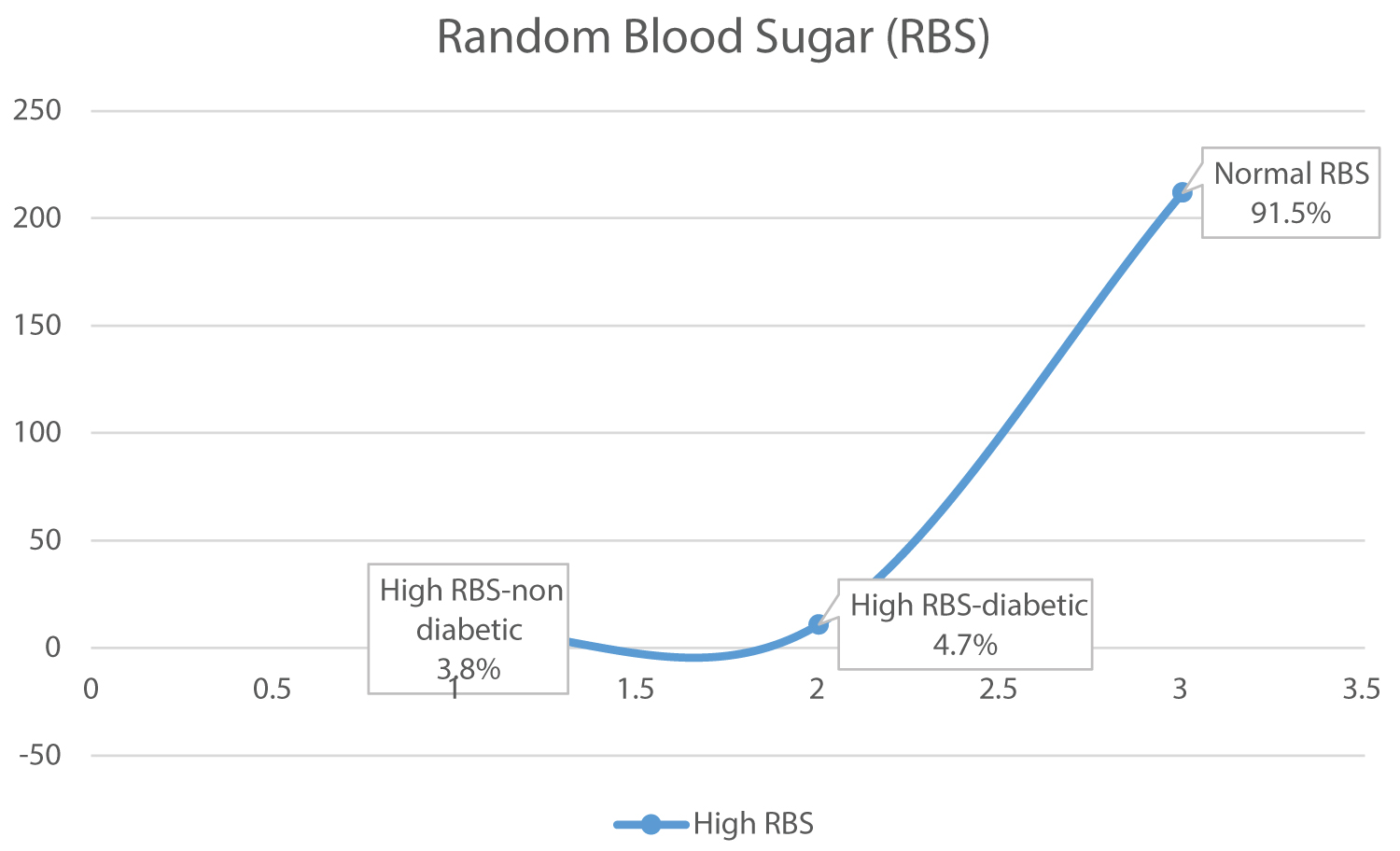 Figure 6: Random blood sugar levels in the study population.
View Figure 6
Figure 6: Random blood sugar levels in the study population.
View Figure 6
Elevated serum creatinine was found in 2 (0.9%) subjects out of the 236 samples studied with one subject having a previous history of diabetes mellitus (Figure 7).
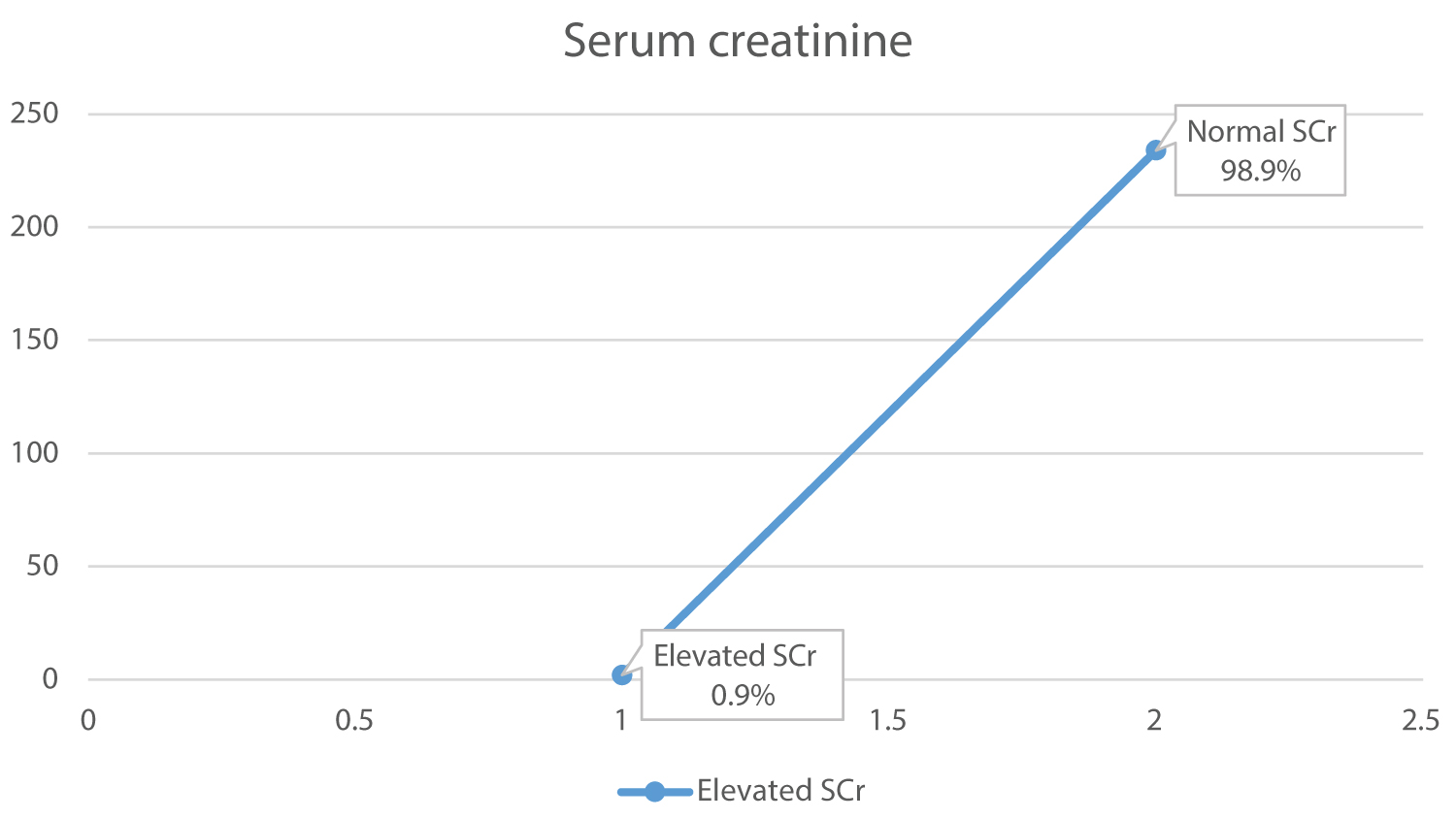 Figure 7: Serum creatinine levels in the study population.
View Figure 7
Figure 7: Serum creatinine levels in the study population.
View Figure 7
In developing countries renal diseases are a growing health problem, and it is important to develop a screening program for the early detection of renal impairment. This will make it possible to design population-oriented preventive measures that will limit the need for renal replacement therapy in the form of dialysis and transplantation. Prevention is important given the shortage of financial support, equipment, and trained personnel. End-stage renal disease (ESRD) is usually the result of slowly progressive renal damage. Due to the asymptomatic nature of renal disease, it is frequently undetected until late in the course, at which stage therapeutic interventions are often ineffective. In contrast, early detection and intervention may halt the decline toward ESRD. Among the various predictors of progression of chronic kidney disease to ESRD, proteinuria is the most potent factor. Data from the United States suggest that for every patient with ESRD, more than 200 have overt chronic kidney disease (stage 3 or 4) and almost 5000 have covert disease (stage 1 or 2) [10]. Unfortunately, this type of information is lacking for most other countries, so international comparisons must be based on ESRD, rather than chronic kidney disease. Also, it should be noted that when international comparisons of ESRD incidence rates are made, the actual comparisons are rates of treatment rather than incidence, since so many individuals with the disorder are neither identified nor treated in the majority of developing nations.
Chronic kidney disease (CKD) is increasingly recognized as a public health problem. Several studies have indicated that the prevalence of CKD is high throughout the world, and the incidence of end-stage renal disease (ESRD) has increased dramatically, imposing a heavy burden on healthy economies. Furthermore, CKD is associated with increased cardiovascular morbidity and even death. The general public lacks sufficient awareness that chronic kidney disease (CKD) is a serious and progressive medical condition. In the early stages, CKD is often asymptomatic, and often remains under diagnosed and undertreated. However, if CKD is detected and treated early, its widespread consequences may be prevented or delayed. Hence, screening for CKD has been increasingly advocated over the last few years.
The Third National Health and Nutrition Examination Survey (NHANES III) found diabetes, hypertension, old age, and male gender to have positive association with the increased risk of elevated serum creatinine levels [11]. Studies have also shown that CKD is associated with a two to threefold higher risk of death in addition to a higher risk of dialysis recruitment and development of congestive heart failure or other cardiovascular events. Several reports indicate that CKD is often undiagnosed and complications of later stages of CKD are often untreated. Detection of CKD, especially at early stages, is important because therapeutic interventions are likely to be effective if they are implemented early in the course of the disease process. This can decrease the economic and social burden of kidney diseases and reduce the high morbidity and mortality associated with CKD [12].
The prevalence of CKD in different populations, including the high-risk groups (e.g. older patients and patients with hypertension and/or diabetes), needs to be explored among various racial groups and in different environmental situations. Taking advantage of the observance of World Kidney Day recently, we conducted a kidney health camp to screen the urban adults for determinants of renal diseases. Understanding the burden of diabetes, hypertension as preventable diseases, and underlying risk factors by organizing population screening is the first step towards planning any effective preventive programs.
Urine testing is an essential component of medical examination and the basic dipstick method is the most common screening procedure for the early detection of renal or urinary tract diseases in apparently healthy or asymptomatic subjects [13]. An abnormal urine test may be the earliest warning of a significant renal disease. Because of its simplicity, routine urine analysis is the best way in early detection of most frequent conditions like proteinuria, haematuria or glucosuria at a very low cost. This is useful in selecting asymptomatic patients with renal diseases who may benefit from early treatment, counselling or who require long term follow-up. The basic dipstick method is the most rapid screening procedure that could be helpful in the early detection of renal or urinary tract diseases among apparently healthy or asymptomatic subjects in the hope of preventing and retarding progression to chronic renal failure.
In India, as in other developing nations that have adopted the lifestyle of developed nations, the population has started becoming more sedentary and eating a high fat and low fibre diet, giving rise to obesity and increase in BMI, which is associated with hypertension and diabetes [14]. In India itself, which has geographically varied areas, the prevalence of hypertension and diabetes are different in different areas, varying from 13 to 58% and 6 to 20%. In the SEEK-India study, hypertension was noted in 64.5% and DM was noted in 31.6% of the CKD group. As per recent Indian Council of Medical Research data, prevalence of diabetes in Indian adult population has risen to 7.1%, (varying from 5.8% in Jharkhand to 13.5% in Chandigarh) and in urban population (over the age of 40 years) the prevalence is as high as 28% [15,16]. Likewise the reported prevalence of hypertension in the adult population today is 17% (14.8% from rural and 21.4% from urban belt). Finding hypertension in 26.1% and diabetes in 29.2% of a population that is otherwise 'healthy' according to their own belief suggests that this population is living on the brink of CKD, warranting immediate measures to improve their health status. This population also had associated albuminuria of 1.3% and elevated serum creatinine of 0.9%.
The answer to this grave problem is timely intervention. In 2003, Mani reported that diabetes accounts for ~30% of chronic renal failure and hypertension for 10% of the patient load on waiting lists for kidney transplantation [16]. In a house-to house survey of 25,000 in South India, he found an incidence of 6% for hypertension and 4% for diabetes. This study suggests that early screening and intervention can control the progress of CKD in our population. This was a single-point cross-sectional study carried out to screen a population who was willing to participate. Hence the possibility of under-/overestimation cannot be ruled out. But larger studies involving more participants from other parts of the state as well as the country need to be carried out.
The main limitations of this screening program were that it had a small sample of study population, the participants were investigated only once and people participate voluntarily, so a selection bias may exist. It is also understood that persons who participate in screening programs tend to be those who are health conscious and better educated or aware. This study did not address the specific cause of proteinuria in individual subjects and it needs further clarification. In the KDIGO 2012 guidelines, the definition of CKD requires the persistence of kidney damage for at least three months. Hence, the single measurement of proteinuria or elevated serum creatinine in our study may not be an accurate predictor of CKD risk.
In conclusion, in an urban population of India that even though has all the facilities for screening and early intervention for kidney diseases, the prevalence of risk factors for renal diseases was higher than that reported in developed nations. This study may represent the tip of the iceberg since participants considered themselves healthy and individuals with other risk factors were excluded. A relatively high prevalence of hypertension, diabetes indicates that a larger population is likely to develop CKD if timely intervention is not provided. There is an urgent need to draft preventive health policies and plan for the allocation of more resources to improve kidney health in India. Finally the aim of the study is to impose the need for better awareness for renal health in the general population which may be accomplished through such initiatives.
None.