The study aim was to study the histological picture of damaged kidneys in patients who died from COVID-19, as well as to attempt to find the objective causes of renal pathology at COVID-19.
Kidney damage in this disease is still considered mainly secondary and associated with multiple organ failure, hypoxia, ischemia, disseminated intravascular coagulation (DIC) at severe and extremely severe disease.
At the same time, it was found that the initial clinical and laboratory signs of renal pathology (in the form of an increase in the level of creatinine and urea in the blood, the presence of proteinuria, cylindruria in the form of granular cylinders, and then oliguria) coincide with time (by 5-7 - 10-12 days of the disease) and are in a parallel progress with lung damage or coronavirus "pneumonia", which, both pathogenetically and clinically, is initially interstitial, and then alveolar hemorrhagic pulmonary edema (as in influenza lung disease). A characteristic feature of this "pneumonia" (pulmonary edema) and kidney damage is their "deferred" and gradual, rather slow, but steady development.
Based on the study of macro- and microscopic preparations of damaged kidneys, the conclusion is that with COVID-19 this lesion with an outcome of acute total nephronecrosis is a consequence of a direct combined viral-drug cytotoxic effect on the renal epithelium, which manifests itself pathomorphologically as total nephronecrosis, and clinically, as a form of acute renal failure, usually with a lethal outcome.
COVID-19, Kidney damage, Pathomorphology
CT: Computed Tomography; DIC: Disseminated Intravascular Coagulation; ARDS: Acute Respiratory Distress Syndrome; SIRS: Systemic Inflammatory Response Syndrome; MOFS: Multiple Organ Failure Syndrome; IMF: Immunofluorescence Analysis
In connection with the COVID-19 pandemic, which began in 2019, the world community has finally recognized that the era of viral infections not only has come, but also entered into full force. This situation has already begun to radically change the scientific and, most importantly, practical approaches to the prevention, diagnosis and treatment of infectious diseases of viral etiology. The experience of the coronavirus pandemic has shown that none of the world countries, regardless of the level of economic and medical development, various opportunities for mass anti-epidemic measures, either independently or in cooperation, have been able to provide adequate protection of their population from COVID-19. All countries turned out to be absolutely unprepared for such a pandemic and remain virtually completely defenseless against a new viral attack.
Despite the relatively low mortality rate in COVID-19 (2.5% in the world; 2.4% in Europe and 1.8% in Ukraine), this disease poses a serious threat to certain categories of the world's population: people over 50 years, patients with diabetes mellitus and persons with concomitant lung diseases. For a couple of years of acquaintance with the "new" coronavirus infection, it became known that the clinical picture of COVID-19 does not have any pathognomonic symptoms and syndromes and does not differ significantly from the clinic of a conventional acute respiratory viral infection.
Clinically and pathogenetically, COVID-19 is similar to influenza. This is especially true for severe forms of the disease. However, pathogenetically COVID-19 "pneumonia" and influenza "pneumonia", in fact and in essence, are not of a such kind. In both cases, it is not pneumonia, but hemorrhagic pulmonary edema, at first interstitial, and then, with further progression - alveolar [1-5]. The only significant difference is the speed and rate of development of this edema. As for flu, it develops early - on days 1-3 of the disease and proceeds quite quickly, even often with lightning speed, which extremely complicates effective therapy. In case of COVID-19, on the contrary, the same hemorrhagic pulmonary edema, which is called "pneumonia", develops, as a rule, quite late - on 5-7, and sometimes later - on the 10-12th days of the disease and also proceeds rather slowly, with a gradual, but a steady increase in respiratory failure. These data are fully confirmed by pathomorphological studies, which were analyzed by us earlier [5]. This is also fully confirmed by instrumental studies in the form of various types of computed tomography (CT), which for COVID-19 has already become practically mandatory and widespread, and soon it may even turn into a routine examination, even in Ukraine. The already universally regulated tomographic syndrome in the form of "frosted glass", positioned by many clinicians as "pathognomonic", in fact is not at all as one, occurs not only in various lung pathologies, but can also be detected in healthy obese people in the exhalation phase. In addition, this syndrome can be detected, as a rule, only if the tomographic "cut" of the lung tissue is less than 4 mm [6]. For lung damage with COVID-19, this syndrome once again confirms the fact that the pathology of the lungs in this disease is not "pneumonia", but pulmonary edema.
Often, the patient is given a conventional X-ray and if no changes are detected via the X-ray, but the patient already has clinical and laboratory signs of respiratory failure (for example, shortness of breath and a decrease in saturation less than 95% with pulse oximetry) is only when a CT is ordered. In this situation, the "frosted glass" symptom is revealed on CT in the form of increased density of lung tissue to X-rays. Obviously, there is a clear contradiction between the data of conventional X-ray and CT in the same patient at the same time and with the same pathology. However, there really is no contradiction as all the differences are understandable. The intensity of X-ray radiation in conventional X-ray diffraction is significantly higher than in CT. Therefore, changes in the interstitium of the lungs in the form of its increased density will be seen, as a rule, only in CT scans, and with conventional X-ray imaging, radiation passes through such a weak barrier almost unhindered. Therefore, a darkening of the lung tissue with CT is seen, but not with an X-ray, since the sensitivity of the CT is much higher, and therefore it is with the CT that even insignificant changes in the lung tissue will be captured.
Several basic morphological changes in the lung tissue led to the formation of a tomographic picture of the lungs in the form of "frosted glass". This is the accumulation of fluid in the interstitial space while maintaining the airiness of the alveoli and bronchioles; partial slight filling of the alveolar apparatus with fluid (exudate, transudate) and cellular elements (damaged epithelium, leukocytes or erythrocytes in hemorrhagic edema). If the alveoli are completely filled, and therefore airless, CT will form a tomographic "consolidation" syndrome, but at this stage these changes will be available for visualization in conventional radiography [6].
Therefore, in the case of interstitial pneumonia, interstitial pulmonary edema, when detecting pathology using CT, detecting of practically anything with a conventional X-ray examination is not be possible. This can also be confirmed clinically by auscultation of the lungs. So, with interstitial pneumonia and interstitial pulmonary edema, we cannot rely on anything to diagnose pneumonia. We will not be able to listen to fine bubbly wet and often dry wheezes (there is no content in the alveoli). Even a weakening of breathing, an increase in "voice tremor" and "bronchophonia" cannot be determined, since the process is diffuse, and these methods use the principle of comparing the indicator over different parts of the lungs. That is why we cannot detect processes in the interstitium of the lungs either clinically or radiologically (with conventional radiography). These methods are very crude in comparison with CT and this is what proves that in COVID-19 the main pathology of the lungs is progressive pulmonary edema, and not "covid pneumonia".
This is also confirmed by the previously proposed (back in April 2020) tactics for therapy of influenza and covid pneumonia, which gave an expressed clinical effect [1-5], but at first it was not only denied, but also categorically prohibited by our official Ukrainian, and earlier - world medicine. This applies to the successful use of dexamethasone in the treatment of COVID-19, and only in June 2020, almost six months after the start of the pandemic, was dexamethasone successfully used as an "innovation". It is the use of dexamethasone, which among glucocorticoid drugs has the most decongestant effect, that gave an expressed clinical effect in influenza and COVID pneumonia, and therefore this once again convincingly confirms the fact that we deal with not pneumonia, but interstitial pulmonary edema, and so approaches to its treatment should be essentially different from those for pneumonia.
This understanding is extremely important, since the term "pneumonia" itself, and also with a rather severe course, as well as a serious prognosis in terms of possibility of mortality, in the mind of a practitioner is associated with the need for massive, multicomponent, intensive and long-term antibiotic therapy. However, the same doctors are well aware that antibiotics do not work on viruses, and their prophylactic prescription is not only unjustified and unpromising, but also fraught with serious threats in the form of toxic side effects, as well as associated complications. Despite this, in most cases in the treatment of patients with COVID-19 pneumonia there is polypharmacy with antibiotics.
At first, it was not very noticeable, especially at the first stages of the formation of treatment tactics and strategies. The main focus was the development and further analysis of therapy for COVID-19 pneumonia. Therefore, much attention was not paid to damage of other organs and systems (kidneys, liver, etc.), since these were associated not with the direct cytotoxic effect of the pathogen or the toxic effects of drug therapy, but with the syndrome of multiple organ failure, which often forms as a result of severe underlying primary pathology. However, after some time, clinicians began to pay attention to the clinical and laboratory signs of liver, kidney and heart damage that were increasingly appearing in patients, which were already difficult to associate with the syndrome of multiple organ failure. The problem of cardiac pathology in COVID-19 was dealt with quite quickly, directly and logically linking it with the use of chloroquine and hydroxychloroquine derivatives, individual macrolides and fluoroquinolones, the cardiotoxicity of which was already well known. This made it possible to quickly abandon the use of antimalarial drugs, which showed a complete lack of effectiveness in COVID-19. The problem of subclinical manifestation of liver damage in the form of an increase in serum transaminases was also associated with drug hepatotoxicity. This assumption turned out to be true, since the increase in transaminases was transient and gradually disappeared after the drug was discontinued.
At first, it was not very noticeable, especially at the first stages of the formation of treatment tactics and strategies. The main focus was the development and further analysis of therapy for COVID-19 pneumonia. Therefore, much attention was not paid to damage of other organs and systems (kidneys, liver, etc.), since these were associated not with the direct cytotoxic effect of the pathogen or the toxic effects of drug therapy, but with the syndrome of multiple organ failure, which often forms as a result of severe underlying primary pathology. However, after some time, clinicians began to pay attention to the clinical and laboratory signs of liver, kidney and heart damage that were increasingly appearing in patients, which were already difficult to associate with the syndrome of multiple organ failure. The problem of cardiac pathology in COVID-19 was dealt with quite quickly, directly and logically linking it with the use of chloroquine and hydroxychloroquine derivatives, individual macrolides and fluoroquinolones, the cardiotoxicity of which was already well known. This made it possible to quickly abandon the use of antimalarial drugs, which showed a complete lack of effectiveness in COVID-19. The problem of subclinical manifestation of liver damage in the form of an increase in serum transaminases was also associated with drug hepatotoxicity. This assumption turned out to be true, since the increase in transaminases was transient and gradually disappeared after the drug was discontinued.
It was found that the first clinical and laboratory symptoms of renal pathology were observed in patients with COVID-19 on days 5-7 - 10-12 of the disease. They manifested themselves in the form of an increase in serum creatinine and urea levels, the presence of minor proteinuria, cylindruria (in the form of granular casts). Later, with the progression of the disease and an increase in the level of creatinine and urea, oliguria was observed in patients followed by anuria. Moreover, nephropathy occurred in patients almost in parallel with COVID-19 pneumonia and also steadily progressed with it.
The etiology of kidney damage in patients with COVID-19 has not yet been fully elucidated, but nevertheless, despite the above facts, most clinicians associate it with multiple organ failure syndrome, ischemia and disseminated intravascular coagulation DIC. Almost no one explains kidney damage by the direct cytotoxic effect of the causative agent COVID-19 or the toxic effect of drugs on nephrocytes, except at the level of a hypothesis or a remote assumption. Also, there is no sufficient and objective data on the pathomorphological histological picture of kidney damage during COVID-19 infection [7-9].
The purpose of this research was to study the histological picture of damaged kidneys in patients who died of COVID-19, as well as to attempt to find the objective causes of renal pathology at COVID-19.
Macroscopically, the kidneys have a deep reddish-brown color (full-blooded). Their dimensions are not increased, correspond to the sex and age of the deceased, and on average are: length - 10-12 cm; width - about 5 cm; thickness - about 3.5 cm. The surface of the kidneys is covered with crater-like depressions, the bottom of which is filled with bloody masses. These formations are not associated with nephrosclerosis. The depth of these formations is from 2 to 5 mm, the diameter ranges from 3 to 6 mm. The fibrous capsule can be easily removed. There is no subcapsular bleeding (Figure 1).
 Figure 1: Macrodrug of the kidney with COVID-19. Crater-like depressions on the surface of the kidney. The bottom of these depressions is filled with bloody masses.
View Figure 1
Figure 1: Macrodrug of the kidney with COVID-19. Crater-like depressions on the surface of the kidney. The bottom of these depressions is filled with bloody masses.
View Figure 1
On the section, the boundaries of the layers (cortical and medullary) are smeared, the depth of crater-like formations is determined at the level of the cortical layer, without going beyond it. On the cut, these formations outwardly resemble "infarctions" of the cortical layer, but infarctions are not detected histologically. The pelvis and calyx are without macroscopic features and changes (Figure 2).
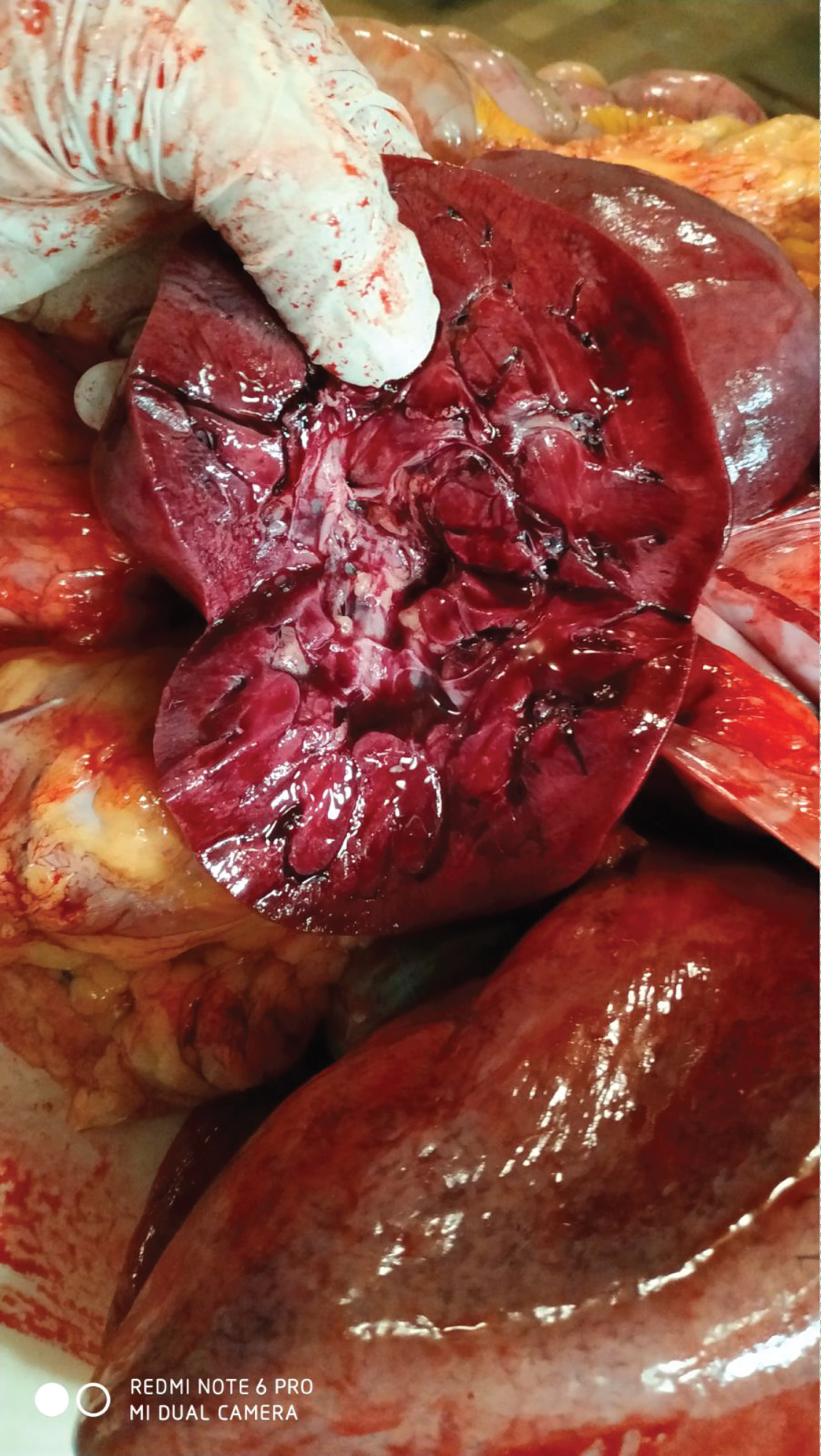 Figure 2: The same kidney in the section. The boundaries of the cortical and medullary layers are blurred, the depth of the crater-like formations is determined at the level of the cortical layer, without going beyond it.
View Figure 2
Figure 2: The same kidney in the section. The boundaries of the cortical and medullary layers are blurred, the depth of the crater-like formations is determined at the level of the cortical layer, without going beyond it.
View Figure 2
Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7 below shows micrographs of histological samples of the cortex and medulla of the kidneys of patients who died from COVID-19.
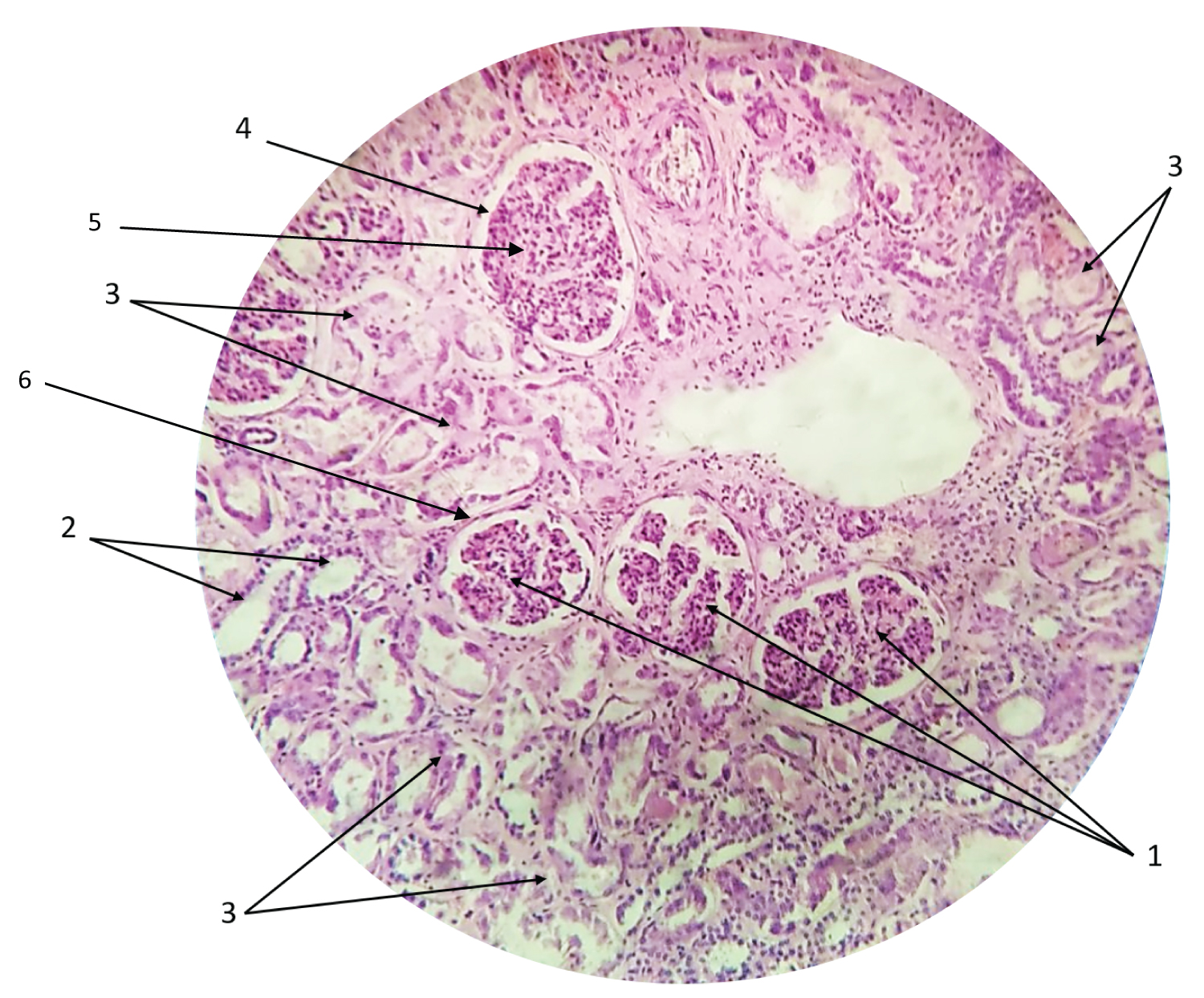 Figure 3: Renal cortex (light microscopy, magnification 40 × 10).
Figure 3: Renal cortex (light microscopy, magnification 40 × 10).
1 - Capillary net of the nephron glomerulus;
2 - Convoluted distal renal tubules;
3 - Expressed dystrophic and necrobiotic changes in the epithelium of the convoluted proximal renal tubules;
4 - Outer capsule of the nephron;
5 - Visceral capsule of the nephron;
6 - Epithelium of the renal tubule.
View Figure 3
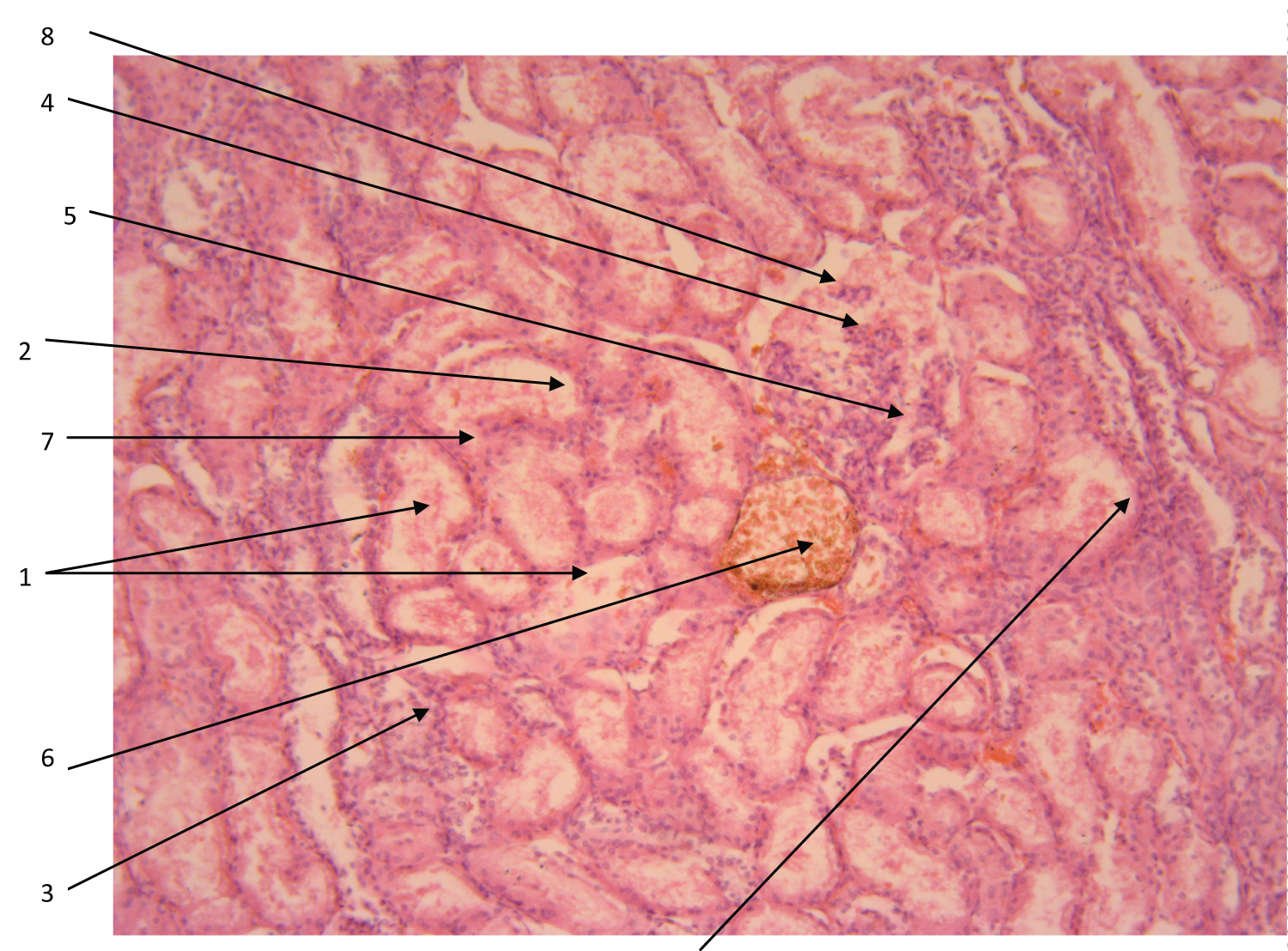 Figure 4: Renal cortex (light microscopy, magnification 40 × 10).
Figure 4: Renal cortex (light microscopy, magnification 40 × 10).
1 - Proximal convoluted tubules;
2 - Tubule contents - degrading desquamated epithelium inside the tubule (granular casts);
3 - Mononuclear infiltration;
4 - Deformed renal glomerulus with deformed capillary net;
5 - Damaged capillary net of the renal glomerulus;
6 - Enlarged vein of the cortical part of the kidney;
7 - Necrosis and degeneration of the epithelium of the renal tubule;
8 - Enlarged cavity of the deformed renal glomerulus.
View Figure 4
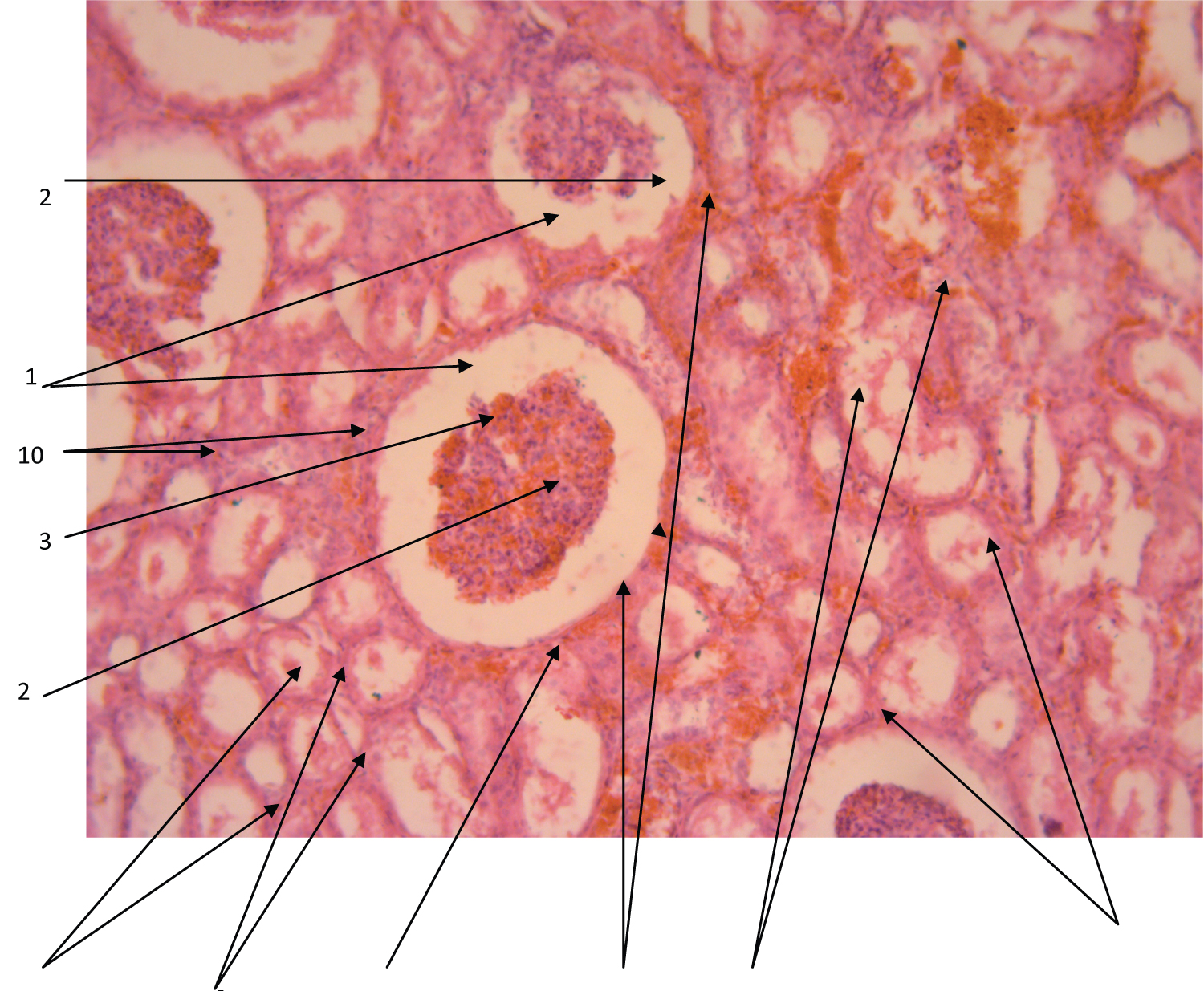 Figure 5: Renal cortex (light microscopy, magnification 40 × 10).
Figure 5: Renal cortex (light microscopy, magnification 40 × 10).
1 - Deformed renal glomerulus;
2 - Deformed and condensed capillary net of the renal glomerulus;
3 - Enlarged cavity of the renal glomerulus;
4 - Outer capsule of the renal glomerulus;
5 - The contents of the cavity of the renal glomerulus;
6 - Proxymal sections of the convoluted renal tubules;
7 - Necrosis and degeneration of the epithelium of the renal tubule;
8 - Granular cylinders in the tubule cavity;
9 - Microthrombi and hemorrhages;
10 - Mononuclear infiltration.
View Figure 5
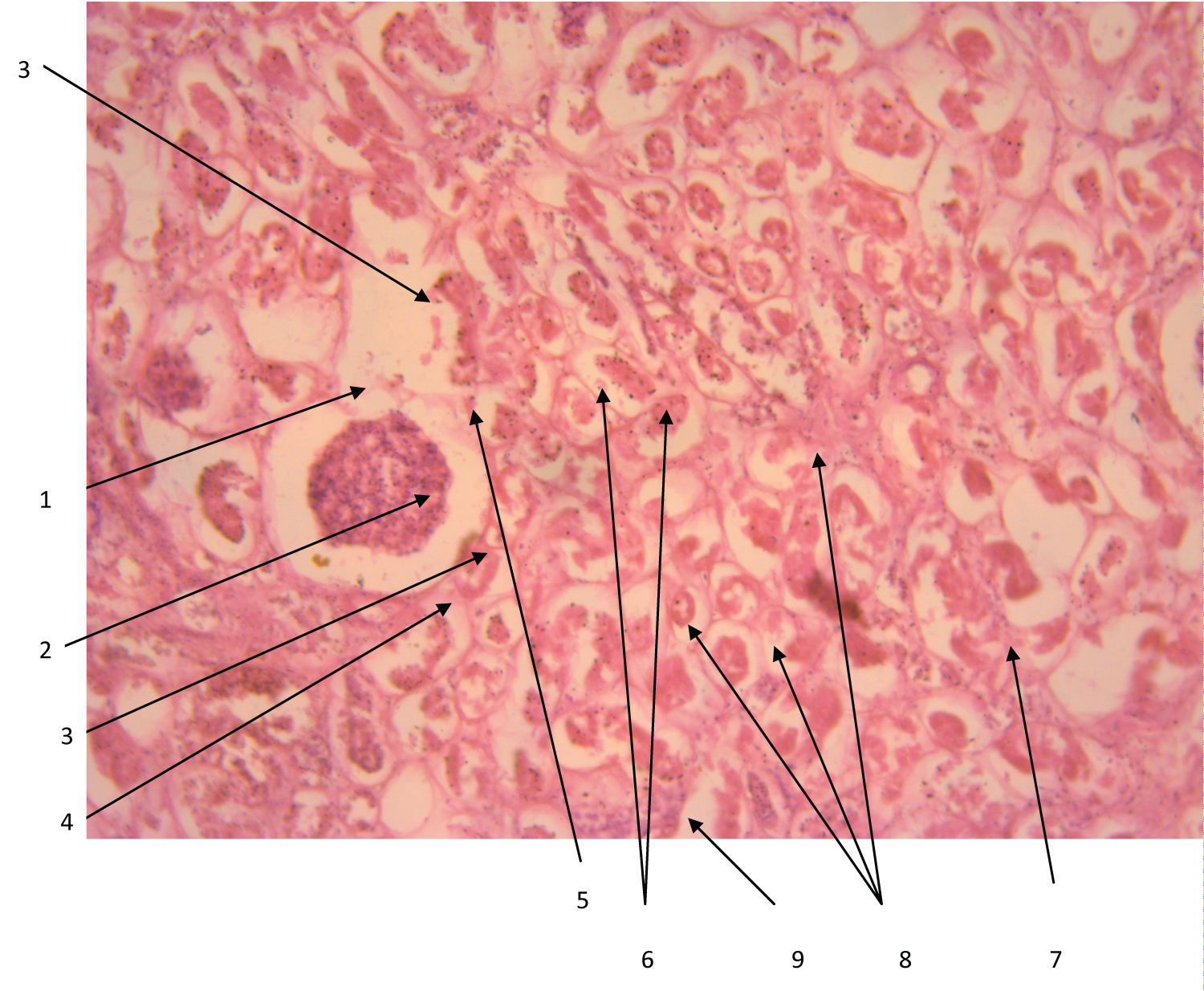 Figure 6: Renal cortex (light microscopy, magnification 40 × 10).
Figure 6: Renal cortex (light microscopy, magnification 40 × 10).
1 - Deformed renal glomerulus;
2 - Deformed and condensed capillary net of the renal glomerulus;
3 - Enlarged cavity of the renal glomerulus;
4 - Outer capsule of the renal glomerulus;
5 - The contents of the cavity of the renal glomerulus;
6 - Proxymal sections of the convoluted renal tubules;
7 - Necrosis and degeneration of the epithelium of the renal tubule;
8 - Granular cylinders in the tubule cavity;
9 - Mononuclear infiltration.
View Figure 6
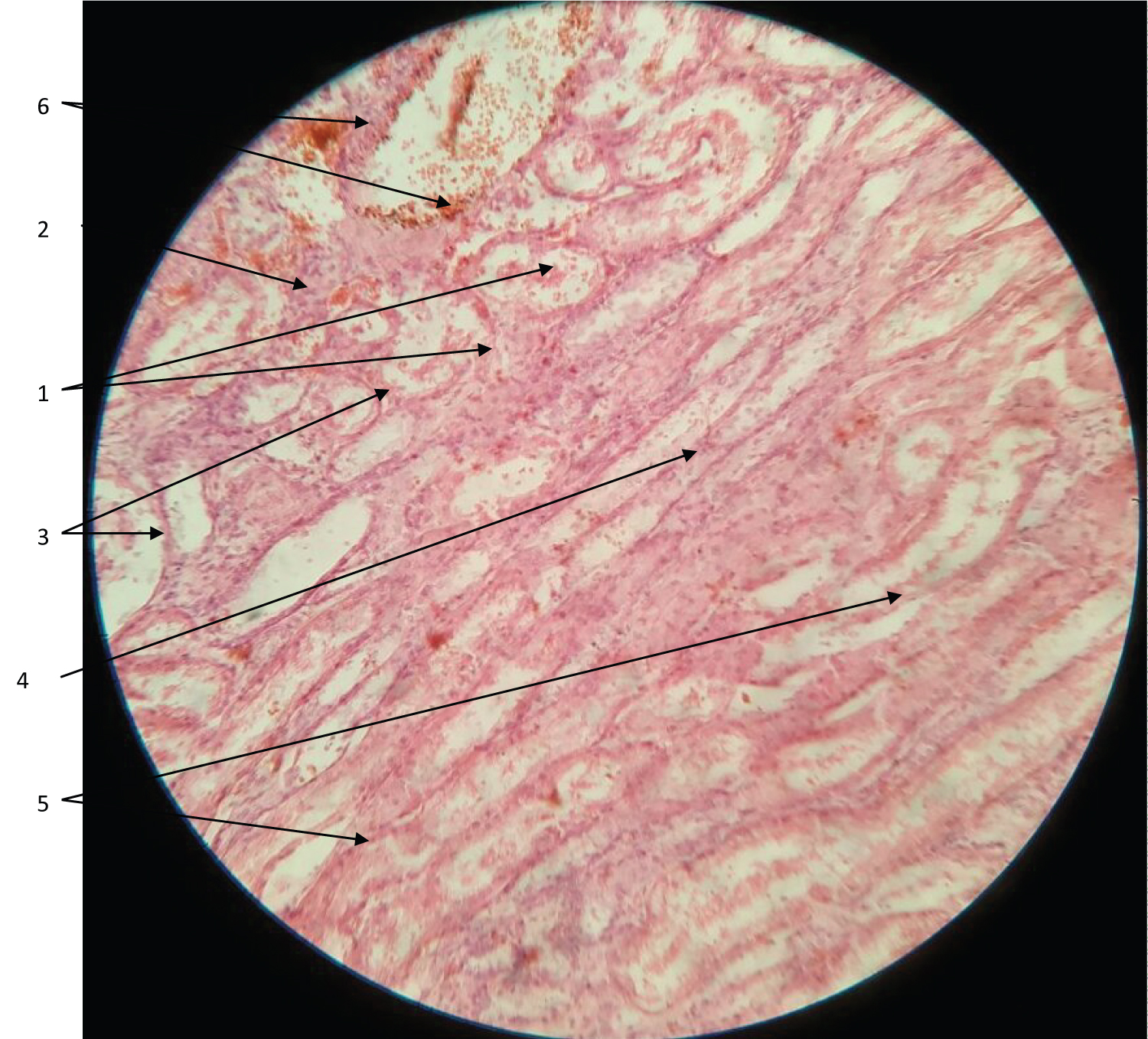 Figure 7: Cerebral and cortical and kidney tissue (light microscopy, magnification 40 × 10).
Figure 7: Cerebral and cortical and kidney tissue (light microscopy, magnification 40 × 10).
1 - Proxymal sections of the convoluted renal tubules;
2 - Necrosis and degeneration of the epithelium of the renal tubule;
3 - Granular cylinders in the tubule cavity;
4 - Thin parts of the nephron tubules;
5 - Collecting ducts;
6 - Hemorrhages.
View Figure 7
The pathohistological picture of kidney damage in most pathological processes is characterized by a fairly uniform and universal picture, in particular, damage to the tubular apparatus of the kidneys, expressed in varying degrees and different types of dystrophy (protein, fat, vacuole), and often by necrosis of the epithelium of the renal tubules of the cortical part of the nephron. Most often, changes are noted precisely in the proximal tubules, both convoluted and straight. Such a picture does not actually depend on the etiology of damage (except for traumatic) and is equally observed: With direct toxic; immune, including autoimmune, as well as toxic-allergic kidney damage; circulatory (ischemic) injury, including acute respiratory distress syndrome (ARDs), systemic inflammatory response syndrome (SIRS), and DIC; multiple organ failure syndrome (MOFS); as well as with direct viral damage to renal cells [8-11]. In all of the above listed etiological factors, the glomerular apparatus of the kidneys practically does not suffer. Apparently, this versatility of the histological picture is due to the higher sensitivity of the tubular epithelium to the effects of direct and indirect damaging factors, as well as a significant difference in the blood supply system of the glomerular and tubular renal apparatus. Thus, more than 50 capillaries are involved in the vascularization of one renal corpuscle (glomerulus), and the capillary net of tubules is already in fact secondary, since it is formed and fed from the efferent arteriole of the glomerulus, and in almost all parts of the renal tubule. Thus, the tubular apparatus, in comparison with the glomerular apparatus, has a lower degree of hemodynamic and metabolic support. It should be pointed out that visual macrohistological changes (ultrastructural changes in cells are not available with light microscopy) of the tubular apparatus are mainly observed in the cortical sections of the tubular apparatus (proximal and distal convoluted tubules) and are rarely observed in the straight sections and the thin part of the tubular apparatus.
This situation has leads to the fact that both, in routine work and in most scientific research, practical pathologists mainly examine the cortex of the kidneys and very rarely take its medulla into consideration. Therefore, in the overwhelming number of studies, the visualization of microscopy (micrographs) of histological samples of the cortical part of the kidneys can be seen.
Next, it is vital to discuss the micrographs of the kidneys in those who died from COVID-19 in a more detailed manner. The micrographs clearly show venous plethora, minor changes in the epithelium of the tubules, focal epithelium of the tubules in a state of proteinaceous, fatty or vacuolar degeneration. The lumens of the tubules are unevenly expanded, contain granular cylinders in places. Epithelial cells are non-nucleated, tiny or granular lumps that retain their cell shape.
A characteristic kidney damage in COVID-19, in contrast to direct toxic, direct drug toxic or mediated drug toxic-allergic, ischemic damage in DIC and MOFS, as well as direct viral damage, is damage not only to the tubular apparatus of the renal nephron (most often the proximal tubule and convoluted tubule), as the most sensitive part of the nephron to various damaging factors. However, significant damage to the glomerular apparatus of the kidney, despite the high level of its vascularization, also takes place.
Pathohistological changes in the renal cortex in COVID-19 patients are manifested in the form of venous plethora, a moderate increase in the size of the renal corpuscles (renal glomeruli), significant expansion and deformation of the cavity under the outer capsule of the renal glomeruli with the presence of tissue detritus in these cavities in the form of degrading glomerular epithelial cells (podocytes, possibly mesangium and capillary endothelium), as well as condensation and wrinkling of the vascular capillary apparatus of the renal glomerulus (Pictures 3-6). Nevertheless, the most expressed changes are noted in the region of the proximal and less often distal convoluted tubules of the nephrons of the renal cortex in the form of their expansion and focal necrosis of the epithelium of the tubules. The cells of the tubular epithelium are in foci at different stages of degradation in a state of protein, fatty or vacuolar degeneration. Epithelial cells are often nuclear-free, retaining the shape of a cell, with contents in the form of crumbs or granular lumps. The lumens of the procystic tubules are unevenly expanded, and in some places contain mainly granular cylinders.
Patients who died from COVID-19 also have acute lesions of the renal tubular apparatus with the same universal histological picture, but still with significant distinctive features. So, dystrophic and necrobiotic processes are noted in the epithelium of the convoluted proximal and distal tubules, but with the formation of granular casts inside them, mainly in the proximal tubules. In the straight part of the tubules (including the loops of Henle), in the medulla of the kidneys, granular casts are practically absent. Also, a significant difference is dystrophic and necrobiotic changes in the epithelium of the glomerulus, particularly its visceral part (epithelium of the visceral part of the capsule of the renal corpuscle) with condensation and wrinkling of the vascular capillary apparatus of the renal glomerulus, significant expansion and deformation of the cavity of the renal glomeruli with the presence of tissue in these cavities degrading glomerular epithelial cells.
A characteristic sign of pathological changes in the kidneys in COVID-19 is an expressed lesion of the proximal convoluted tubules in the cortex with the accumulation of granular casts in their lumen (degrading epithelium of the tubules) and the almost total absence of granular casts in the straight part of the tubules (including in the Henle loops) in the brain substance of the kidneys (Figure 7). Thus, pathohistologically, the picture of kidney damage in COVID-19 can be considered as total nephronecrosis. The few studies previously conducted in patients with COVID-19 almost coincided with the results of this study. Also, light microscopy revealed a picture of acute tubular damage in the form of the disappearance of the brush border, vacuolar degeneration and obvious necrosis of the tubular epithelium with exposure of the basement membrane, expansion of the lumen of the tubules and the accumulation of degrading epithelium in the form of granular cylinders. Diffuse aggregation of erythrocytes in the peritubular and glomerular capillaries was also observed; at times microbes in the vasculature of the glomeruli were without obvious destruction of erythrocytes, without platelets and without fibrin thrombi. A feature of the aggregation of erythrocytes in the microvasculature of the renal capillaries was that such aggregation was without platelets, fragments of erythrocytes, fibrin thrombi or fibrinoid necrosis. Changes in the nephron glomeruli in the form of segmental damage to the endothelium (foamy degeneration) and epithelium (vacuolization) were also noted [8, 9]. The illustration (Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7) depicts precisely acute total nephronecrosis, in contrast to the most common acute tubular nephronecrosis. However, despite this distinctive feature, the reasons for such special kidney damage and any etiology of kidney damage in COVID-19, still remain unclear and incomprehensible.
All possible causes of kidney damage have been given above. With COVID-19, they are all possible. Indeed, with this disease, there is ARDS, and DIC syndrome, ischemia with massive microbial formation, hyperactivity of the immune system, and severe hypoxia. A direct or indirect toxic effect on the kidneys of the drugs themselves is also possible, but there is no direct evidence for this. However, it should be noted that in the histological picture with these types of pathology; there is practically no damage to the glomerular apparatus and this can already be considered a distinctive feature of kidney damage in COVID-19. This does not, however, give us an answer to the question of the reason for such a situation. The only logical assumption about the etiology of such a feature (if for all types of pathology of the above causes of kidney damage it is not observed) is that it can only be either direct viral damage to kidney cells, or the combined effect of these factors, and possibly in combination with the direct cytotoxic effect of the causative agent of COVID-19 on nephrocytes (nephron epithelium).
It is known that with a direct cytopathic viral action on kidney cells of polyomaviruses, herpes viruses, adenoviruses, etc., the following morphological picture can be observed - acute tubular, tubulo-interstitial nephritis with a predominant lesion of the collecting ducts, distal sections and a thin part (Henle loop) of the tubular apparatus of the kidney [12]. Replication of viruses in the epithelium of the renal tubules leads to cell lysis and exposure of the basic membranes, which is expressed in varying degrees of acute tubular necrosis. The glomerular apparatus is practically not damaged and its changes, as a rule, are limited to damage to the parietal epithelial cells of the outer capsule of the renal corpuscle. According to information sources, replication of the virus in podocytes (epithelium of the visceral part of the glomerulus) is extremely rare. Viral replication is also extremely rare, and, consequently, has a direct cytopathic effect on the endothelium of renal vessels, primarily capillaries [12-14].
These changes in the histological picture in the kidneys are associated with the direct cytopathic effect of polyomaviruses, herpesviruses and adenoviruses, and there are still no works illustrating and proving the direct effect of the causative agent of COVID-19 on the nephron epithelium in the available information space. Indeed, there is a sufficient number of studies that indicate that with COVID-19, kidney damage occurs, but they associate it not only with the possible direct cytopathic effect of the pathogen on nephrocytes, but with a number of other possible causes, which were mentioned earlier – hypoxia, ischemia, SIRS, ARDS, DIC, immune, autoimmune, toxic-allergic and direct toxic drug damage to the kidneys [9,15,16].
All these reasons take place in COVID-19 and may possibly be the cause of kidney damage, but we should not forget that the cellular membrane receptor for the COVID-19 virus in the form of ACE-2 (angiotensin-converting enzyme) is also present on the renal epithelium of nephrons (more - in the epithelium of the proximal tubules, less - on podocytes and is practically absent on the renal endothelium), and therefore, given the tropism of the virus to ACE-2 and the use of this particular receptor by the virus for attachment and invasion into the cell, there is a very high probability of SARS-CoV-2 replication in epithelium of the nephrons, both in its glomeruli and in the tubular apparatus [9,15,16].
Direct evidence of this can be a combined lesion of both the epithelium of the glomeruli and the epithelium of the tubules in the form of total nephronecrosis, which practically does not occur with the other causes of acute kidney damage mentioned above. An indirect, but still quite weighty proof of this can be the fact that the initial clinical and laboratory signs of renal pathology (in the form of an increase in the level of creatinine and urea in the blood, the presence of proteinuria, cylindruria in the form of granular cylinders, and then oliguria) coincide in time (on 5-7 - 10-12 days of illness) and in parallel progress with lung damage or coronavirus "pneumonia", which, both pathogenetically and clinically, is at first interstitial, and then alveolar hemorrhagic pulmonary edema (as with influenza pulmonary disease). A characteristic feature of this "pneumonia" (pulmonary edema) and kidney damage is their "deferred" and gradual, rather slow, but steady development.
The clinical feature of kidney damage in COVID-19 is that it, as a rule, develops in patients with diabetes mellitus, often not only compensated, but also latent, already revealed by indirect signs during pathological and morphological examination at sections (this is mainly characteristic for diabetes mellitus angiopathy). Nevertheless, the above arguments in favor of COVID-19 replication in nephrocytes and their direct damage by the COVID-19 virus, although extremely significant, still remain only an assumption. The final solution to the issue can only be the detection of the virus or its components in the nephron epithelium using immunofluorescence analysis (IMF) in the form of immunofluorescence microscopy or electron microscopy. However, today for IMF there are still no necessary antibody diagnostics (monoclonal, fluorochrome-labeled antibodies to COVID-19 proteins), and electron microscopy is still an inaccessible and rather technically difficult research method, even at the stage of preparation of preparations for this microscopy. Therefore, evidence of the affinity for kidney tissue and the direct cytopathic effect of COVID-19 on nephrocytes remains promising research. Despite this, studies have already appeared showing that in the epithelium of the glomeruli (podocytes) with electron and IMF microscopy of kidney tissues of the patients who died from COVID-19, the replication of a virus morphologically and genetically very similar to SARS-CoV-2 is registered, but this finding is not yet finalized [7-9].
Now it is necessary to turn to the analysis of other possible causes of kidney damage in COVID-19. Given the presence of a proven hyperimmune component in the pathogenesis of COVID-19, requiring the use of immunosuppressive therapy, which proved to be quite effective, which once again confirms one of the leading roles of this component in the development of pathomechanisms of COVID-19, it would be logical to assume an immune or autoimmune mechanism of kidney damage by COVID-19. Indeed, there is every reason for this. However, in the histological picture of the damaged renal tissue there is no lymphocytic and macrophage infiltration of the kidney tissues, which is obligatory for such pathomechanisms [10,11]. Perhaps these pathomechanisms take place in COVID-19, but their severity and tropism to the kidney tissues is most likely insignificant being low in severity and activity.
There remains one more important and very promising candidate in terms of direct negative toxic effects on the kidneys - this is direct drug damage to nephrocytes. It is well known that many drugs have nephrotoxic effects to varying degrees. Models of acute renal failure (animal models) used in experimental practice are often created precisely due to the administration of nephrotoxic pharmacological drugs to animals [17]. Also in clinical practice, there are frequent cases of complications and side effects of drug therapy in the form of nephrotoxic action. Most often, clinicians encounter the nephrotoxic effect of antibiotics, for example, such widespread ones as the group of aminoglycosides, certain representatives of fluoroquinolones, most antifungal drugs for systemic use, etc [17].
An analysis of the therapeutic practice of treating coronavirus "pneumonia" with COVID-19 shows that at both the outpatient and inpatient stages, there is serious polypharmacy, which is expressed in the unjustified prescription of several antibiotics to the patient at the same time, the toxic effects of which can not only add up, but when interacting with other drugs, often exhibit paradoxical reactions. The most commonly used are cephalosporins, fluoroquinolones and macrolides, often in the maximum allowed doses, given the "severity" of the patient’s condition and the "severity" of the prognosis in COVID-19. Both cephalosporins and fluoroquinolones have a fairly expressed dose-dependent nephrotoxicity, and some representatives of these groups together with macrodids and hepatotoxicity. Therefore, quite often in patients with COVID-19 receiving such massive therapy without visible clinical manifestations of kidney and liver damage, there is a moderate or even significant increase in hepatic transaminases, as well as in the level of creatinine and urea, but at first without a significant decrease in the level of creatinine clearance. However, with the progression of kidney tissue damage in such patients, clinical signs of acute renal failure appear in the form of oliguria, and then anuria. Often, as already described above, signs of significant and severe renal failure appear already with significant progression of coronavirus "pneumonia" (interstitial, and then alveolar pulmonary edema).
The histological picture of acute drug damage to the kidneys (for example, with the toxic effect of aminoglycosides and cephalosporins) does not actually differ from the universal described above and is expressed as acute dystrophy and/or necrosis of the epithelium of the nephron tubules or tubular necrosis [17, 18]. The most frequent pathomechanism in acute drug-induced tubulonecrosis is actually the direct interaction of the pharmacological drug with the epithelium of the proximal tubules, the accumulation of the drug inside the epithelium of this part of the tubules and often binding to individual cell organelles, which disrupts its metabolism, vital activity (varying degrees of dystrophy) and ultimately leads to death (necrosis) [17]. For example, gentamicin, binding to ribosomes, disrupts cellular protein synthesis, reduces phospholipase activity, reduces phospholipid production, and blocks mitochondrial respiration in the cell. Cephalosporins also damage the proximal renal tubule epithelium. Villi, cytoplasmic vesicles in the cytoplasm and mitochondria disappear from these cells. Indeed, different pharmaceuticals have different molecular mechanisms of nephrotoxicity, but pathomorphologically and clinically they have an almost identical picture [19].
Analyzing the material presented, it can most likely be argued that total necrosis with damage to both the glomerular and tubular nephron apparatus has a complex etiology and is a combined pathology associated with both the direct cytotoxic effect of the COVID-19 pathogen during its replication in the renal epithelium, and with direct cytotoxic effect on nephrocytes of pharmacological drugs (most often antibiotics). This is fully consistent with the fact that the renal epithelium has membrane receptors (in the form of ACE-2) to the capsid structures of the COVID-19 virus, and therefore, the probability of COVID-19 virus replication in the renal epithelium is very high. This is also combined with the fact that a distinctive feature of the pathomorphological picture of the kidneys in COVID-19 is damage not only to the tubular, but also to the glomerular apparatus of the renal nephrons. Acute tubulonecrosis in COVID-19 completely repeats the picture of drug damage to the kidneys when using nephrotoxic drugs. This is also consistent with the fact that nephrotoxicity of pharmaceuticals is more expressed in patients with diabetes mellitus. In particular, this is true for a significant number of patients who died from COVID-19, and it is in this group of patients that kidney damage is the most common at COVID-19.
Thus, it can be concluded that in COVID-19, kidney damage with an outcome in acute total nephronecrosis is a consequence of a direct combined viral-drug cytotoxic effect on the renal epithelium, manifested pathomorphologically as total nephronecrosis, and clinically - in the form of acute renal failure, usually fatal. However, the final answer about the coronavirus etiology of kidney damage in COVID-19 and the direct viral cytotoxicity of COVID-19 can only be given by virological and immunological studies of damaged kidney tissues, which will be carried out in further studies.
It is necessary to honor the deceased patients, whose tissues and organs gave us material for the research, which brought us one step closer to solving the problems of the COVID-19 pandemic.