Severe acute respiratory syndrome coronavirus 2 (SARS-COV2) is a single stranded RNA virus and is the cause of the ongoing COVID-19 pandemic and although its main targets are the immune and respiratory systems, acute kidney injury (AKI) has been observed in a high percentage of cases. This is a syndrome which manifests morphologically with the hallmark being acute tubular injury/necrosis and also clinically with the appearing of proteinuria, hematuria, etc. However, this document will focus more in the morphological changes seen in kidneys of patients with, or have died from Covid-19 [1].
A theory as to why the kidney is a target organ for the virus is because the receptors for SARS-COV2, angiotensin-converting enzyme 2 (ACE2) is more abundant in the kidney than in the lung tissue. Viral particles can be detected on the renal tubular epithelial cells and podocytes, indicating that the virus infects the renal parenchymal cells. This causes collapsing glomerular disease (CG) [2].
Light microscopy reveal severe collapsing focal segmental glomerulo sclerosis (FSGS) which is characterized by segmental and global collapse of the glomerular capillaries and marked hypertrophy and hyperplasia of podocytes (Figure 1).
 Figure 1: Light microscopy study (Masson's trichrome stain, original magnification [b,d]*200 and [c]*400) showed the following: First, a severe collapsing glomerulopathy (focal segmental glomerulosclerosis) characterized by (b,c) the global collapse of shrinking capillary loops and the detachment from the basement membrane of (b) hypertrophic, proliferating podocytes (or "cobble stone pattern"), which contained numerous (c) protein reabsorption vacuoles. (d) Second, acute tubular lesions with focal tubular necrosis, dilatation, and the presence of intratubular reabsorption vacuoles.
View Figure 1
Figure 1: Light microscopy study (Masson's trichrome stain, original magnification [b,d]*200 and [c]*400) showed the following: First, a severe collapsing glomerulopathy (focal segmental glomerulosclerosis) characterized by (b,c) the global collapse of shrinking capillary loops and the detachment from the basement membrane of (b) hypertrophic, proliferating podocytes (or "cobble stone pattern"), which contained numerous (c) protein reabsorption vacuoles. (d) Second, acute tubular lesions with focal tubular necrosis, dilatation, and the presence of intratubular reabsorption vacuoles.
View Figure 1
In the proximal tubule, we can see acute tubular necrosis which is manifested as a loss of the brush border (Figure 2a), vacuolar degeneration, and dilation of the tubular lumen with cellular debris (Figure 2b). Hemosiderin in the tubular epithelium may also be present in patients with hematuria. The distal tubule and collecting ducts may show occasional swelling and edematous expansion of the interstitial space.
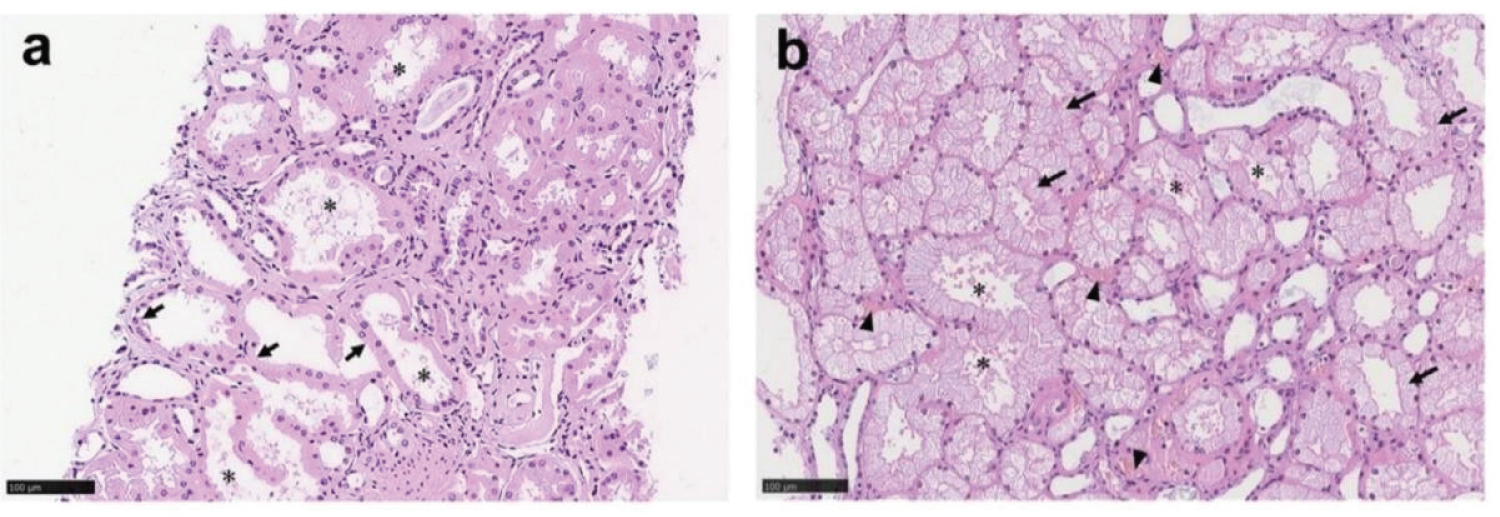 Figure 2: Proximal tubules showed (a) loss of brush border and (b) vacuolar degeneration (arrows), with debris composed of necrotic epitheliumin tubular lumens.
View Figure 2
Figure 2: Proximal tubules showed (a) loss of brush border and (b) vacuolar degeneration (arrows), with debris composed of necrotic epitheliumin tubular lumens.
View Figure 2
Finally, in patients with diabetes mellitus, on the electron microscope, changes such as nodular mesangial expansion, increased thickness of the basement membrane without deposits and hyalinosis of arterioles indicating diabetic nephropathy.