Background: Adequacy and quality goals in dialysis units are mainly focused on laboratory targets, and although their clinical relevance is not questionable, they overlook the importance of patients' experiences and preferences. We aim to evaluate the health-related quality of life in peritoneal dialysis patients using the 5-level EQ-5D questionnaire and assess the relationship between the health state and the current standard criteria of quality in dialysis.
Methods: A cross-sectional, single-center study was conducted in 70 prevalent peritoneal dialysis patients, over 18-years-old, with follow-up in our peritoneal dialysis unit until 2019.
Results: The mean EQ-5D-index and EQ VAS were 0.896 and 67, respectively. No patient had a negative index. Older age and a previous cardiovascular event were associated with worst quality of life (EQ-5D index 0.821 vs. 0.864, p = 0.02 and 0.796 vs. 0.879, p = 0.05, respectively). Age and peritoneal dialysis vintage were the most significant predictors of quality of life [EQ VAS (r = -0.3, p = 0.03) and (r = -0.4, p < 0.01), respectively]. The levels of Kt/V, serum albumin, or hemoglobin did not affect health-related quality of life.
Conclusions: In our study, age and peritoneal dialysis vintage were the most significant predictors of quality of life, emphasizing the need for special attention for these patients. A better nutritional status was also associated with a higher quality of life. We found no link between the analytical factors used in standard criteria and EQ-5D, signaling that the perception of quality of life goes well beyond small solute clearance.
Chronic kidney disease (CKD) has a high clinical and socioeconomic burden that needs awareness and a plan of action [1]. Adequacy and quality goals in dialysis units are mainly focused on laboratory targets (serum hemoglobin, phosphate, Kt/V urea), and although their clinical relevance is not questionable, they overlook the importance of patients’ experiences and preferences. The evidence of the higher impact of these patient-reported outcome measures (PROMs) on mortality and morbidity, even when compared with other biologic factors, is increasing, including in dialysis patients [2,3]. Beyond disease-related outcomes, there is an urgent need for clinicians to focus on the implementation of validated PROMs in routine care practice.
Health-related quality of life (HRQOL) is widely accepted as an important outcome of healthcare, with a strong correlation with mortality, morbidity, and hospitalization in dialysis patients [2-5]. Moreover, it is a tool that provides information about the impact of the treatment on perceived well-being and allows for base treatment decisions [6]. Among the numerous HRQOL instruments currently available, the EuroQol-5 Dimensions tool (EQ-5D) is well-accepted for assessing HRQOL, is practical to use and has been applied to dialysis patients [7-10]. Additionally, it can be used to compute Quality Adjusted Life Years (QALY) in economic evaluations of healthcare [7].
We aimed to evaluate the HRQOL in peritoneal dialysis (PD) patients using EQ-5D and assess the relationship between the health state and the current standard criteria of quality in dialysis.
A cross-sectional, single-center observational study was performed on prevalent PD patients attending our tertiary center in 2019. The 5-level EQ-5D (EQ-5D-5L) questionnaire was used in a routine hospital visit. The study included patients over 18 years of age, without acute illness and/or cognitive impairment, that had been performing PD at least one month before the questionnaire and remained in PD until December 2019.
Demographic and clinical data were measured at the time of the questionnaire. Dialysis dose was calculated as the weekly KT/V urea from a 24-hour urinary and dialysate clearance. Residual renal function was measured through creatinine clearance (CrCl), calculated from a 24-hour urine collection, with the assessment of urine creatinine and serum creatinine. Nutritional status was presumed by the normalized protein catabolic rate (nPCR) and serum albumin.
The EQ-5D is a standardized measure of health status developed by the EuroQol Group to provide a simple, generic measure of health for clinical and economic appraisal [7]. It consists of a descriptive system questionnaire and a visual analogue scale (EQ VAS). It has five domains: Mobility, self-care, usual activities, pain/discomfort, and anxiety/depression; and five response levels: no problems, slight problems, moderate problems, severe problems, and unable to/extreme problems. The descriptive system can be represented by a single number (index value), which reflects how good or bad a health state is according to the preferences of the general population. In our study, we use the Portuguese version of the EQ-5D questionnaire [11], but to calculate the index value, we use the value set of the Spanish population due to an unavailable algorithm for the Portuguese population (i.e. EQ-5D-5L Crosswalk Index Value Calculator) [12]. The index value ranged from - 0.654 to 1 (full health) and negative values represented values as worse than dead (0). The EQ VAS is a vertical visual scale of 0 (worst) to 100 (best) and provides a quantitative measure of the patient’s perception of their overall health.
The quantitative variables were summarized as means ± standard deviations (SD). The Kolmogorov-Smirnov test was used to assess the normality of the distribution of data. Comparison between groups was performed using an independent Student’s t-test and one-way analysis of variance (ANOVA) for the normally distributed variables and the Mann-Whitney U test for the abnormally distributed variables. Pearson’s and Spearman’s rank correlation coefficients were used to test for the association between variables. Multiple linear regression was performed to investigate the association between the possible prognostic variables and the reported EQ-VAS scores and EQ-5D-5L index values. The significance level for all tests was defined as p < 0.05. Data were analyzed using SPSS version 28 (SPSS Inc., Chicago, IL, USA).
A total of 70 patients were included. One patient was excluded due to an acute exit-site infection at the time of the routine visit. Thirty-seven (52.9%) patients were male, and the mean age (SD) was 55.9 (15.4) years. Chronic glomerulonephritis was the CKD etiology most frequent (37%). Overall, 38 (54.3%) patients were overweight, nine (12.9%) patients had diabetes, and 23 (32.9%) had a previous cardiovascular event (ischemic heart disease, cerebrovascular disease, or peripheric vascular disease). The mean (SD) PD vintage was 55.7 (15.4) months, and 57.1% of patients were on continuous ambulatory peritoneal dialysis. The mean (SD) KT/V and CrCl were 1.93 (0.42) and 71.85 (24.6) L/week/1.73 m 2 , respectively. The socio-demographic and clinical characteristics are displayed in Table 1.
Table 1: Demographic and clinical characteristics of prevalent peritoneal dialysis patients. View Table 1
A total of 29 different health statuses were described, of which 24 (34.3%) patients had no problems in all five dimensions (i.e. index value of 1). No patient reported extreme problems in any dimension. EQ-5D frequencies and proportions are represented in Table 2. The mean (SD) EQ-5D-index was 0.896 (0.122). No patient had a negative index. There was a strong positive correlation between the EQ-5D index value and the EQ VAS (r = 0.52, p < 0.001). Patients older than 65 years had a lower EQ-5D index (0.821 vs. 0.864, p = 0.02), as did patients with a previous cardiovascular event (0.796 vs. 0.879, p = 0.05). Proportions of gender, overweight, diabetes, or the technique of PD were not significantly different between group patients.
Table 2: EQ-5D-5L frequencies and proportions reported by dimension and level. View Table 2
The mean EQ VAS score was 67 (16). Approximately 7% of patients had an EQ VAS of less than 50. The EQ VAS frequencies are shown in Figure 1. The nPCR (r = 0.4, p = 0.01) and albumin (r = 0.4, p = 0.02) had a positive correlation with the EQ VAS.
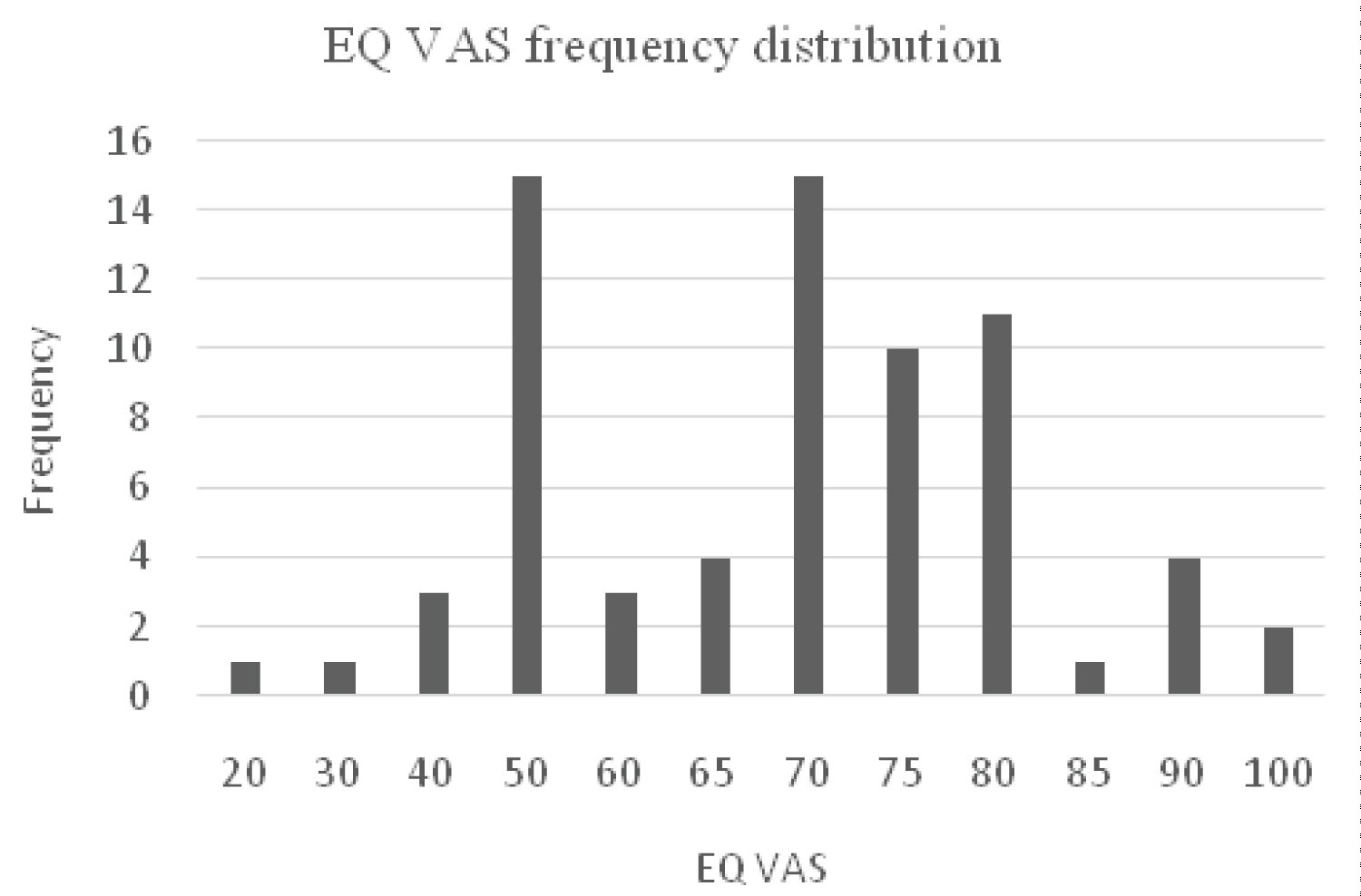 Figure 1: EQ-5D-5L VAS frequency distribution.
View Figure 1
Figure 1: EQ-5D-5L VAS frequency distribution.
View Figure 1
The EQ-5D-index (r = -0.3, p = 0.02) and EQ VAS (r = -0.4, p < 0.01) had a negative correlation with PD vintage as well as with age (r = -0.3, p = 0.03). There was no association between KT/V weekly, ClCr, or hemoglobin and EQ-5D-index or EQ VAS.
Age and PD vintage were the most significant predictors of quality of life (Table 3). This explained about 25% of the variance in EQ-5D scores. The levels of Kt/V, CrCl, serum albumin, or hemoglobin did not affect HRQOL.
Table 3: Multiple linear regression analysis of association between factors and EQ-5D score. View Table 3
In our study, HRQOL in PD patients was assessed through the EQ-5D. The relationship between HRQOL and demographic, clinical, and biochemical factors was also evaluated.
Several studies in end-stage renal disease (ESRD) patients used the EQ-5D as an HRQOL instrument and, its validity and responsiveness are well-recognized [9,10,13,14]. It is easy to apply compared with other generic tools, and EQ-5D seems to have a more favorable cost-effectiveness profile, leading to more attractive incremental cost-effectiveness ratios when compared to other instruments [9,15].
In our study, the mean EQ-5D index was 0.896 (0.122). When comparing with other studies in dialysis patients in Korea (0.704 ± 0.199) [15], Japan (0.75 ± 0.17) [16], Taiwan (0.65 ± 0.23) [17] or Australia 0.41 (0.42) [18] our index values were higher. Socioeconomic factors have an important effect on HRQOL and could explain this difference, but this is presumptive [10]. Moreover, the healthcare system and accessibility to medical care are more difficult in developing countries, which could delay the diagnosis and therapy and indirectly affect the patient’s HRQOL. On the other hand, we can hypothesize that organizational details in our unit, associated with proximity, favor patients´ perceptions of health status.
In our work, the EQ-5D-index and reported EQ VAS showed a strong correlation, in line with previous studies. Although the EQ VAS only uses one overall dimension of health status, the accuracy is equivalent to evaluation with the 5-dimension questionnaire [19,20].
Our results revealed age as one of the main negative predictors of HRQOL, with patients older than 65 years having the worst quality of life. A review of the literature indicated that age was a common factor of poorer quality of life. The longer duration of disease and more health complications could explain the lower index values [15,21]. However, these results may further signalize that tailoring elderly patients treatment demands a more accurate management of their priorities and expectations towards life, possibly addressing other dimensions of quality such as pain and mobility constraints, as examples.
According to our study, a previous cardiovascular event was also associated with lower HRQOL. Cardiovascular disease (CVD) is one of the main causes of death in dialysis patients [22]. It has been described, both in ESRD patients [23,24] and other populations, [25,26] as an important predictor of poorer quality of life. To our knowledge, there is still no study of HRQOL with EQ-5D in PD patients reporting the association between CVD and lower quality of life.
In terms of clinical parameters, dialysis vintage was the strongest negative predictor of quality of life. Our results are in line with previous studies, where longer time on dialysis is associated with lower HRQOL [27]. Preventive and supportive measures to mitigate burnout under therapy are desirable but presumably unable to efface the burden of chronic disease.
As for the analytical factors, higher levels of nPCR and serum albumin were positively associated with HRQOL. This either be linked to nutrition or comorbidity because these are interconnected. The assessment of nutritional status is complex and requires a multi-dimensional approach, including anthropometric measurements, bio-impedance, subjective global assessment, and laboratory parameters [28]. Although our study was not designed for a more complete nutritional assessment, in ESRD patients, lower levels of nPCR and serum albumin are common surrogates of malnutrition [28]. As described in similar studies, nutritional status has a strong correlation with HRQOL in dialysis patients, where poor nutrition is associated with lower quality of life, even adjusted for age and comorbidities [29,30].
This study did not find an association between weekly Kt/V urea and HRQOL. Adequacy in PD is focused on solute and fluid removal, mainly through weekly KT/V [31,32]. Most studies suggested that improved survival on PD therapy was associated with higher total small- and medium-molecules clearances, mainly due to the continuous schedules and residual renal protection [31]. Nevertheless, the association between improving solute removal and quality of life is not clearly established, and we may even argue that therapy adjustment to achieve adequacy targets may often be an incremental burden in the patient's day-to-day life. In fact, the ADEMEX trial, a prospective randomized controlled clinical trial, showed that improving small molecule clearances in chronic PD patients did not result in an improvement in HRQOL scores [33].
Residual renal function (RRF) is a powerful predictor of survival in PD patients [34,35]. There is conflicting evidence concerning the benefit of RRF on the quality of life of PD patients [34,36-38]. Recent research, however, has found that RRF has a positive impact on both physical and mental health [36,38-40]. In fact, Park HC, et al. described an independent correlation between lower RRF, depression and HRQOL in PD patients [37]. It is not unexpected that by sparing dialysis exchanges during the day and postponing more complex dialysis schedules, incremental PD certainly benefits patient independence and mitigates treatment intrusion. In our results, we found no link between ClCr and HRQOL, signaling that the perception of quality of life goes well beyond small solute clearance.
Beyond analytical targets, an updating of the concept of appropriate dialysis requires a focus on personal patient experiences using HRQOL metrics in the CKD circuit. In our study, the EQ-5D demonstrated poorer quality of life in the elderly and patients who had been on dialysis for a longer period, emphasizing the need for special attention for these patients. The nutritional status demands more accurate assessment and intervention since it has an important impact on the HRQOL of dialysis patients. The incorporation of HRQOL measures will raise awareness about the interventions that have a positive impact on quality of life and also individualize treatment targets.
The authors did not receive nay funding regarding this article.
Conception and design: Anabela Rodrigues. Patient selection, data collection and interpretation of results: Inês Sala, João P. Fernandes, Bruno Fraga Dias, Joana Tavares, Olívia Santos and Maria João Carvalho. Literature review and drafting of the article: Inês Sala. Critical revision of the article for important intellectual content and final approval: Joana Tavares and Anabela Rodrigues.