An evaluation of the implementation of smoke-free commercial outdoor dining was carried out to evaluate proprietors' awareness and preparedness for the implementation of Smoke-Free Outdoor Dining regulations in Liverpool, Australia.
A pre-post assessment of the awareness and preparedness for smoke-free Commercial Outdoor Dining (COD) bans commencing in NSW on the 6 July 2015 was carried out at 19 COD premises in Liverpool's Macquarie Mall by the Public Health Unit.
The study found limited effectiveness of the smoking bans in the area, despite a high level of awareness of key changes required and high level of preparedness for the smoke-free COD regulations. The majority of COD operators chose to provide a designated smoking area to allow patrons to continue to smoke legally. Over two thirds (69%) of operators were concerned/somewhat concerned about the impact of the bans on their business before the bans but decreased to 55% (10) after the bans.
Loopholes in COD regulations have resulted in consumers being increasingly exposed to smoke. A multi-sectoral approach is needed to review the legislation and protect consumers.
Loopholes in COD regulations have resulted in consumers being increasingly exposed to smoke. A multi-sectoral approach is needed to review the legislation and protect consumers.
Tobacco use is the leading cause of death and disease in Australia. Each year nearly 20,000 Australians die and more than 150,000 are hospitalised due to tobacco related illness [1]. Smoking increases the risk of many cancers, and is a major cause of chronic obstructive pulmonary disease and ischaemic heart disease [2]. Exposure to environmental tobacco smoke is also responsible for a wide array of detrimental health effects. In children, breathing environmental tobacco smoke can lead to bronchitis, pneumonia, asthma and other illnesses [3]. Research shows there is no safe level of exposure to smoking or second-hand smoke (SHS) [2,4]. Early respiratory damage has been linked to low levels of SHS exposure or occasional smoking [4]. There is compelling scientific evidence that environmental tobacco smoke has detrimental effect upon exposed non-smoking adults and children [5]. Regardless of location, exposure to smoking and second hand smoke has negatively impacted people's wellbeing and increase the likelihood of psychological distress [6].
The Australian Federal Government has been instrumental by introducing legislation to control smoking in public places to reduce environmental tobacco smoke (also known as second hand smoke or passive smoking) [1].
The New South Wales (NSW) Smoke Free Environment Act 2000 came into force prohibiting smoking in Smoke Free Enclosed Public Places. Examples of Smoke Free Enclosed Public Places include:
Shopping centres, malls and plazas, restaurants, cafes, cafeterias, dining areas and other eating places, schools, colleges and universities, professional, trade, commercial and other business premises, community centres or halls and places of public worship, theatres, cinemas, libraries and galleries, trains, buses, trams, aeroplanes, taxis and hire cars, and ferries and other vessels, hostels, motels, fitness centres, bowling alleys and other sporting and recreational facilities, childcare facilities, hospitals, casinos, hotels, clubs and nightclubs [7].
Following the introduction of the Act 2000, businesses voiced concerns about potential revenue loss. A survey carried out shortly after introducing smoke-free dining, revealed that 76% of proprietors surveyed reported normal patronage and 14% reported increased patronage [8].
The NSW Smoke-Free Environment Regulation 2007 was introduced to prevent smoking in enclosed public spaces where 75% of the ceiling/wall area is not open to the outside [9].
In 2012, the NSW Ministry of Health (NSW Health) developed the NSW Tobacco Strategy 2012-2017, to educate communities, businesses and agencies about changes to legislation with the aim to reduce smoking, combat chronic disease and rising health costs [3]. Amendments to the Smoke Free Environment Act 2000 in 2013, made it an offence to smoke in certain outdoor areas, including train station platforms, bus stops, taxi ranks, light rail stops, ferry wharfs, spectator areas of sporting events, within 10 metres of children's playground equipment, and within 4 metres of pedestrian public access points [7]. These bans were implemented to protect people from harmful second-hand tobacco smoke.
Provisions were made in the Tobacco Legislation Amendment Act 2012, to delay the implementation of smoking restrictions in commercial outdoor dining areas until 6 July 2015. From the 6 July 2015, the Smoke Free Environment Act 2000, also prevented smoking in the following areas:
a) Within 4 metres of a pedestrian entrance or exit from a licensed venue, restaurant or café; and
b) Commercial Outdoor Dining (COD) Areas, defined as a public place that is a seated dining area, or (a) within 4 metres of a seated dining area on premises that are licensed premises under the Liquor Act 2007 or the premises of a restaurant, or (b) within 10 metres of a place at a food fair where food is sold or supplied for consumption at the event [7].
The regulations defined a seated dining area as 'an area in which seating is provided and in which food that has been purchased and served on plates or packaged for immediate consumption is consumed. The seating must have been provided by the occupier of the premises where the food is purchased or by the operator of the business from which the food is purchased. An area is only a seated dining area when food is being consumed there or is available to be purchased and consumed there'[7].
The staged approach to banning smoking was to allow the community and businesses enough time to prepare for and adapt to the bans and has reportedly resulted in high levels of compliance with the bans. Owners and managers of smoke-free dining venues in South Australia reported very high levels of customer compliance following the introduction of laws [10]. Compliance increased over time from 88.2-92.3% at five months to 95.7-99.6% after 18 months after the commencement of the laws, with either none or few customer breaching the smoking ban and only 4.4% of customers refusing to comply with this requests to leave smoke-free areas [11].
In NSW Australia, Environmental Health Officers (EHOs) are appointed and authorised by the Ministry of Health under section 126 of the Public Health Act 2010 to carry out inspections under the Public Health (Tobacco) Act 2008, and to conduct various functions under section 14 of the Smoke-free Environment Act 2000 [3]. EHOs employed by Public Health Units in NSW were responsible for enforcing the new smoke-free COD requirements. EHOs were initially involved in visiting premises to monitor compliance and provide education to proprietors and consumers to assist with compliance.
In 2014, South Western Sydney Local Health District (SWSLHD) was described as having the second highest smoking rate in NSW [12]. Leading up to the introduction of smoke-free COD in 2015, the SWSLHD Public Health Unit (PHU) and Health Promotion Service (HPS) collaborated to raise awareness among COD businesses to the pending changes, provide resources to assist in assessment of premises and regulated signage to comply with the regulations. Health Promotion activities were carried out from 15th June in 12 locations in SWSLHD known to have a high incidence of smoking. Public education campaigns were also carried out by NSW Health.
There has been no systematic approach to evaluate proprietors' level of awareness of and preparedness for the smoking bans, and how this influences their levels of compliance with smoke-free requirements. This information would assist public health and health promotion practitioners to understand the effectiveness of preparedness activities and to identify areas for development of targeted interventions. In the context of this study, preparedness implies the operators' level of readiness to implement appropriate non-smoking signage, maintain appropriate distance, appropriate use/dis-use of smoking paraphernalia and readiness to inform patrons about their need to comply with smoking regulations once the changes took effect. Compliance implies the proprietor's willingness to and actual implementation of the requirements of the regulations. A case study was carried out of the implementation of smoke-free commercial outdoor dining to evaluate proprietors' awareness and preparedness for the implementation of Smoke-Free Outdoor Dining regulations and its impact on proprietors' and consumers' compliance with the regulations, in Liverpool, New South Wales. The objectives were to determine proprietors': (i) Level of awareness of their responsibilities, (ii) Level of preparedness for and (iii) Level of compliance with the regulations. Baseline smoking levels in commercial outdoor dining areas before and after the bans were also evaluated.
The Macquarie Street Mall and Elizabeth Street food precinct (Figure 1) located between Moore Street and Elizabeth Street in the Liverpool Local Government Area was selected because it was: (i) Included in the awareness raising activities carried out by HPS; (ii) Availability of several outdoor dining areas before implementation; (iii) A clientele that is representative of the cultural diversity of the LHD's population; (iv) A variety of dining activities occurring mainly during day time hours; and (v) Convenience of access due to its proximity to the Public Health Unit.
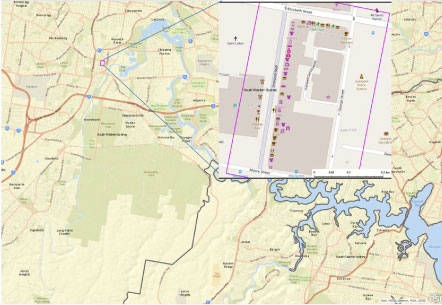 Figure 1: Map of a section of south western Sydney with Macquarie Street Mall (inset). View Figure 1
Figure 1: Map of a section of south western Sydney with Macquarie Street Mall (inset). View Figure 1
All Nineteen (19) commercial food operators present in the locality that were inspected were invited to participate in the study. Enhanced inspection of outdoor dining premises was carried out as part of routine environmental tobacco compliance and monitoring inspections, by authorised EHOs before (in June 2015) and after the implementation of the bans on 6 July 2015.
Data was collected using a modified survey and observation tool informed by New South Wales Health Smoke-Free Commercial Dining Checklist. The surveys were completed by EHOs from the Public Health Unit during routine inspections, with verbal informed consent obtained from proprietors for the additional questions about their awareness, preparedness and compliance with regulations.
Observation data, including premises layout and seating capacity, services provided, estimated number of patrons, presence of smoking signage, presence of smoking paraphernalia and smoking volume were collected from the premises in the study area, during routine compliance and monitoring inspections using the modified checklist. Retrospective data collected during routine compliance and monitoring inspections in June 2015 were reviewed to provide a baseline estimate (before) of the pre-implementation period. Observations made at the monitoring visit in October 2015, was used for the post-implementation (after) comparison.
The pre- and post-implementation survey was conducted from 19 - 20 October 2015; three months after the bans came into effect on 6 July 2015. All commercial dining premises in the Macquarie Street Mall and Elizabeth Street food precinct in Liverpool were included.
Odds ratios, 95%CI and P-values were calculated for differences in proportions using the bans as the exposure variable, with the assistance of the MedCalc Software bvba © 2019.
The South Western Sydney Local Health District Human Research Ethics Committee (HREC) approved this project.
Nineteen (19) commercial food operators in the locality were visited and all consented to participate in the study. One of the premises had closed at post-implementation leaving 18. All premises sold food and drink before the introduction of the new smoking regulations.
Proprietors' level of awareness of the legislation before and after implementation is presented in Figure 2. At the baseline, some proprietors were already aware of the 4-metre rule; and nearly a third of proprietors had some knowledge of fines and signage, but only provided those response after the interviewer provided a list to choose from. Most proprietors indicated that they had obtained information that smoking was going to be banned in COD areas from advertising, mail outs and provision of postcards and fact sheets, but had limited knowledge of signage and penalties (Figure 2a). In comparison, at post-implementation, proprietors were able to identify the changes in the regulations without being provided with a list. Significantly more participants than at baseline were aware of the 4 metre rule (OR 4.46; 95% CI 1.11 -17.90), potential fines for non-compliance by businesses (OR 90.0; 95% CI 8.46 - 957.65) and smokers (OR 68.0; 95% CI 8.54 - 541.86), requirements for 'No smoking' (OR 90.0; 95% CI 8.46 - 957.65) and 'No food to be eaten' (OR 39.0; 95% CI 2.05 - 743.42) signage requirements for COD areas (Figure 2b).
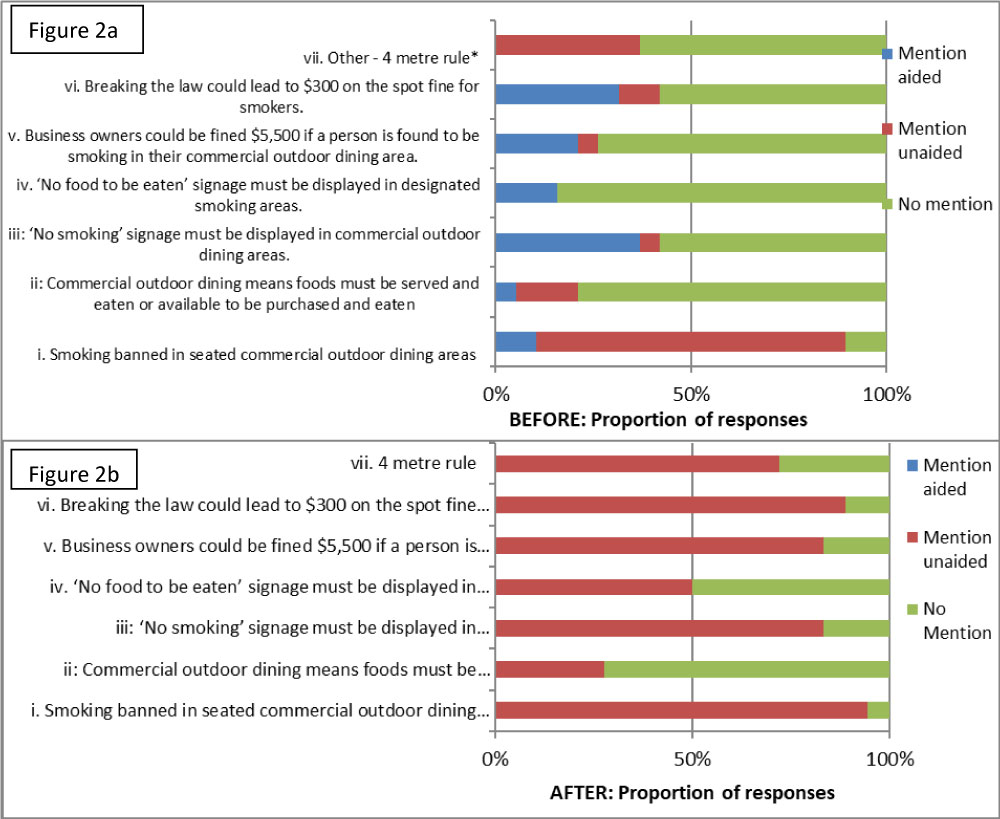 Figure 2: Proprietors awareness of smoke free legislation requirements. View Figure 2
Figure 2: Proprietors awareness of smoke free legislation requirements. View Figure 2
Proprietors identified some steps taken in relation to their COD areas at baseline and post-implementation.
Prior to the new requirements taking effect, 21% of proprietors were unsure what they would do with their food operations, but the majority (58%) indicated they intended to implement smoke-free dining and 21% said they would convert to non-dining services such as offering coffee only, which was allowed under the new regulations (Figure 3). During the survey some proprietors reported that, prior to the bans, they had not realised that they could have designated smoking areas if only drinks and coffee were provided. As a result, only 6 (33.3%) of proprietors had exclusively implemented smoke-free COD, with an additional 17% of proprietors choosing to go part-time smoke-free COD during peak periods and part-time smoking at other times.
 Figure 3: Proprietors intentions prior to new smoking regulations. View Figure 3
Figure 3: Proprietors intentions prior to new smoking regulations. View Figure 3
Two thirds of all the operators, including 6 operators that only did drinks and an additional 6 (50%) of operators that also provided COD areas, provided a designated smoking area. This was because, while 9% more premises actually continued to provide COD areas after the implementation of smoking restrictions compared with those who said they wouldn't, it should be noted that approximately half (6/12 or 50%) of operators that provided COD areas, were also providing a separate designated smoking area.
When proprietors were asked specifically if they planned to have a designated smoking area, about 58% said this was their intention before compared with 67% who said they did implement a designated smoking area after the implementation of the bans. Only two of the 12 operators who had implemented a designated smoking area did not have appropriate signage in place at the post-implementation visit.
The majority of proprietors (84% before and 89% after) indicated that they were aware of the bans coming into effect. After the bans came into effect, there was a decrease in the number of proprietors who said they intended to erect non-mandatory signs at pedestrian entrance/exits. The majority (75% before vs. 83% after) of proprietors felt they had been given adequate time to implement changes for the smoking bans. Prior to the bans, 69% [13] operators had indicated they were either concerned or somewhat concerned about the impact of the bans on their business. This proportion of those who were concerned decreased by 14% (55% or 10) after the bans but was not significant (P = 0.422). The majority of those who were unconcerned continued to provide a COD area with no smoking.
Several proprietors also reported that there had been some confusion about what was required under the bans. Owners and operators initially did not understand that they had the option of choosing to designate a smoking area where drinks could be allowed. This information had become clearer to them during the health promotional visits and through information provided by EHOs about the regulations.
Ten premises overall reported a loss of business since the implementation of the new laws, with premises that chose to have a dedicated smoking area reporting the largest losses in patronage. Two operators, one offering smoke-free dining and the other providing mixed smoke-free and designated smoking area on a part time basis, reported that their businesses had lost up to 50% of business. The losses were reportedly associated with loss from food sales; and with customers choosing to utilise dedicated smoking areas to drink and smoke.
Observations of activities and the layout of COD revealed a reduction in the number of patrons from 158 to 38, with significant reductions in the number of smokers from 28 to 0 (P < 0.05), smoking paraphernalia such as ash trays from 68 to 28 (P < 0.05) and shisha/hookah (from 21 to 11) in the study area after the changes took effect. In comparison, the number of tables and chairs increased, and the vast majority had appropriate signage placed in appropriate locations (P < 0.05) (Table 1).
Table 1: Observations of smoke-free COD layout and activities. View Table 1
The aim of this evaluation was to determine COD proprietors' awareness and preparedness for the implementation of smoke-free COD regulations and its impact on proprietors' and consumers' compliance after the implementation of the new regulations. Through the process of evaluating proprietors' level of preparedness and compliance, enforcement officers were able to provide accurate information, deal with any misconceptions that owners and operators had, and to assess the level of compliance with the new smoke-free COD regulations.
Information gained on preparedness and compliance and compliance of customers with smoke-free requirements can assist public health and health promotion practitioners to understand the effectiveness of preparedness activities. This identifies areas for development of targeted interventions to inform EHO enforcement approaches in the LHD.
The study found that after 6 July 2015 more COD operators were aware of some of the key changes required by the smoke-free COD regulations, including awareness of the 4-metre rule, potential fines for non-compliance, requirements for signage and requirements for smoke-free COD areas. Two thirds of all the operators, including 6 operators that only provided drinks and an additional 6 (50%) of operators that also provided smoke-free COD areas, provided a designated smoking area.
One interesting finding is that owners and operators, who were reportedly unsure of what to do prior to the bans, became aware of the option of providing a designated smoking area where only drinks could be consumed, after the regulations were explained by health staff and after the bans came into effect on 6 July. This may be as a result of operators hearing about the bans through various news media, but it wasn't clear that they had other options.
The losses were reportedly associated with loss from food sales; and with customers choosing to utilise dedicated smoking areas to drink and smoke. The reduction in concerns may have been attributed to the improved awareness that operators could choose to change their business to provide designated smoking areas or do partial smoke free COD and smoking. There is a high smoking rate among the populations that reside in this area.
On one hand, a complete ban of smoking in COD would have been ideal, to protect the large numbers of shoppers and community members using food, shopping and recreational facilities in the vicinity, against the toxic effects of second-hand smoke [2,4]. NSW research shows strong community support from both non-smokers and smokers for smoking bans in commercial outdoor dining areas and other public areas. The study carried out by the Cancer Council found 80% of people support smoking bans in commercial outdoor dining areas of restaurants, hotels, clubs and cafés and within 4 metres of a pedestrian access point to a restaurant, hotel, club or café; with seven out of ten people support fines being issued to those who fail to comply with the outdoor smoking laws [13].
The decision by some operators to change their business to 'designated smoking areas (whether full-time or part-time), would likely be influenced by the fact that a significant proportion of their clientele were from ethnic groups with high smoking rates [13]. News reports before [14] and after [15] the bans confirm the concerns of operators in the study area. Several days after the ban, one news report stated that "cafes in places like Liverpool have already stopped customers from eating in their outdoor spaces so patrons can still light up" [16]. Additional reports implied that operators were also concerned about their personal safety and the repercussions of having to enforce the smoking bans in their COD areas [16].
Observations of activities and the layout of COD revealed a significant reduction in the number of patrons from 158 to 38 and number of smokers from 28 to 0 post implementation. The reduction in customers may be associated with the changes in business operations, such as in cases where businesses were serving food only at lunch time, while allowing smoking before and after lunch time and in cases where only tea and coffee were being sold, leading to a reduction in customers [16]. The low numbers of patrons could also be associated with the increased awareness created by the media coverage on the smoking bans and patrons' uncertainty around business operations following the bans. The reduction in smoking may also be a reflection of the public's awareness and support for the bans in COD areas [15,17].
Since the conduct of this study, more café operators have converted to allow smoking legally. This may have been influenced by an increase in patronage from new migrant residents and construction workers from nearby development sites who smoke. The increased smoking in this locality, designed for families, has resulted in more residents complaining to the local council. The matter has been raised at Liverpool City Council's March 2018 meeting; with a proposal for a smoking ban at Macquarie Mall raised at their meeting in June 2018. The news report indicated that the trial to make Macquarie Mall a smoke-free zone would be supported by the development of a comprehensive education and communications program for communities and amendment of the Macquarie Mall Outdoor Dining Permit, and lobbying NSW Health to enforce smoke-free zones. According to the report, there was strong community support for a complete smoking ban in the Macquarie Mall. The community were in support, indicating that banning smoking would be an opportunity for a totally new demographic to use the mall, resulting in increased patronage for local businesses [18]. However, the matter has been deferred by the Liverpool Council to allow further consultation with stakeholders. Some local councillors have called for an urgent resolution to the situation, in response to the community's concerns [18].
In conclusion, this study identified a relatively high level of awareness and preparedness for the implementation of smoke-free COD regulations among COD proprietors' in Liverpool's Macquarie Street Mall. However, this case study revealed that once proprietors understood that they had options, a majority of COD operators chose to change their business operations in order to allow customers to lawfully continue to smoke. This has inadvertently resulted in more clients smoking in close proximity to where food is being consumed, with an increased risk for consumers to be exposed to second hand smoke. It reinforces the challenges associated with the limitations in the regulations to prohibit smoking completely in COD areas and for physical barriers to be erected between those areas permitted to smoke and those with smoke-free dining. There is a lack of political will to move ahead to make this Mall a smoke free zone. A multi-sectoral collaborative approach that engages culturally and linguistically diverse consumers as key partners is needed to develop and implement effective strategies to reduce smoking in commercial outdoor dining areas, particularly in areas with high smoking rates.