Our world is changing. Globally the population of older people will account for 1.4 billion by 2030. In 2050 we are seeing the prevalence of disability in developing countries to increase by 400% due to aging population. At the same time, natural disasters have increased by 60% in the last decade and climate change is impacting natural disasters by increasing the frequency of flooding, landslides, drought. The population of older adults is amongst the groups of the most vulnerable to the negative impacts of natural disasters. The importance of assessing the geriatric patient through an ethnogeriatric lens has become increasingly apparent. In the US we treat older adults from various ethnic backgrounds and who have potentially lived through natural disasters and geographic isolation. The research addressing how disasters and geographic isolation is affecting older adults is still limited and more research needs to be supported in the future. Evidently, contrary to some commonly held beliefs that aging is associated with increased dependency, loss of self-control, ailment, incapacity, disengagement from life, and social isolation that may make older adults more vulnerable to life crises, some studies show that elderly earthquake survivors have a higher positive mental health compared to younger counterparts, in the wake of natural disasters. Further research is needed to study hubs of chronically affected areas by natural disasters as well as geographic isolation and hardship, which could serve clarify the trajectory of aging in place, mental health, resiliency, and frailty under the reign of repetitively impeding natural disasters and isolation.
Natural disasters, Resilience, Social support, Trauma, Preparedness plans
As our population is aging rapidly and with climate change taking over the planet, we are seeing more natural catastrophes annually. It is of utmost importance to be reminded of the vast vulnerability associated with the older adult population around the globe living through and surviving natural disasters. The daunting mortality of these patients during natural disasters together with the robust immigration patterns we observe in our world, call for a change in the role of the healthcare providers, who need to train to address the needs of such populations, including support to survive post natural disaster syndromes, and should ultimately participate in the design of preparedness plans.
The island of Kefalonia is a majestic island on the Ionian Greek Sea. Kefalonia sustained one of the most catastrophic earthquakes in 1953, also known as the Great Kefalonia earthquake, described as one of the greatest disasters to ever befall Greece. An earthquake like this was bound to happen eventually, as this island is just east of a major tectonic fault, where the European and the Aegean plates meet. In the history of the island there were four major earthquakes, which literally destroyed almost every house on the island. The strongest earthquake measured 7.3 on the Richter scale in August of 1953. The center was on the southern tip of the island and raised the area by 60 cm [1]. The watermarks on rocks around the coast bear testimony to this. The only areas that escaped destruction were on the northern side.
Most of the population fled the island: Some people temporarily moved to the capital of Greece, however the majority emigrated out of Greece entirely to countries such as Canada, USA, Australia, or the UK, leaving the island and its economy in ruins. This left only a few residents on the island. Survivors who were unable to leave are the people who stayed behind and sustained the consequences of this natural disaster. This part of the population was affected the most by the tectonic rath that led to dramatic geography hence isolation and lack of access to resources thereafter. These communities aged in place and through the years, as their health needs increase, they remain isolated from proper and organized health care, mainly supported by family and community values. This is a population that not only lives to tell the story of the 1953 disasters but also constitutes a population ideal to study the effect of trauma from natural disasters on physical and mental health.
Earthquakes still regularly affect the island, including several in recent years, including 2003, 2005, 2014 and 2018. There is no information on the percentage of older adults lost to these earthquakes. Sadly, upon researching the mortality of older adults during natural disasters, the unfair loss of mainly older adults ranges from anecdotal to most recently clear and dominant.
Our world is changing. Natural disasters have increased by 60% in the last decade entailing earthquakes, heat waves, tsunamis, cyclones, typhoons, mudslides, hurricanes, and floods (Table 1). Climate change is impacting natural disasters by increasing the frequency of flooding, landslides, drought, and wildfires around the world. Figure 1 is depicting the decadal average number of deaths from natural disasters. Globally the population of older people will account for 1.4 billion by 2030, will exceed the number of children by 2045, with a percentage of older adults rising to 22% by 2050 ( Help Age International 2024 ). The population of older adults is amongst the groups of the most vulnerable to the negative impacts of natural disasters. Currently, it is estimated that 26 million older adults are affected by natural disasters every year [2].
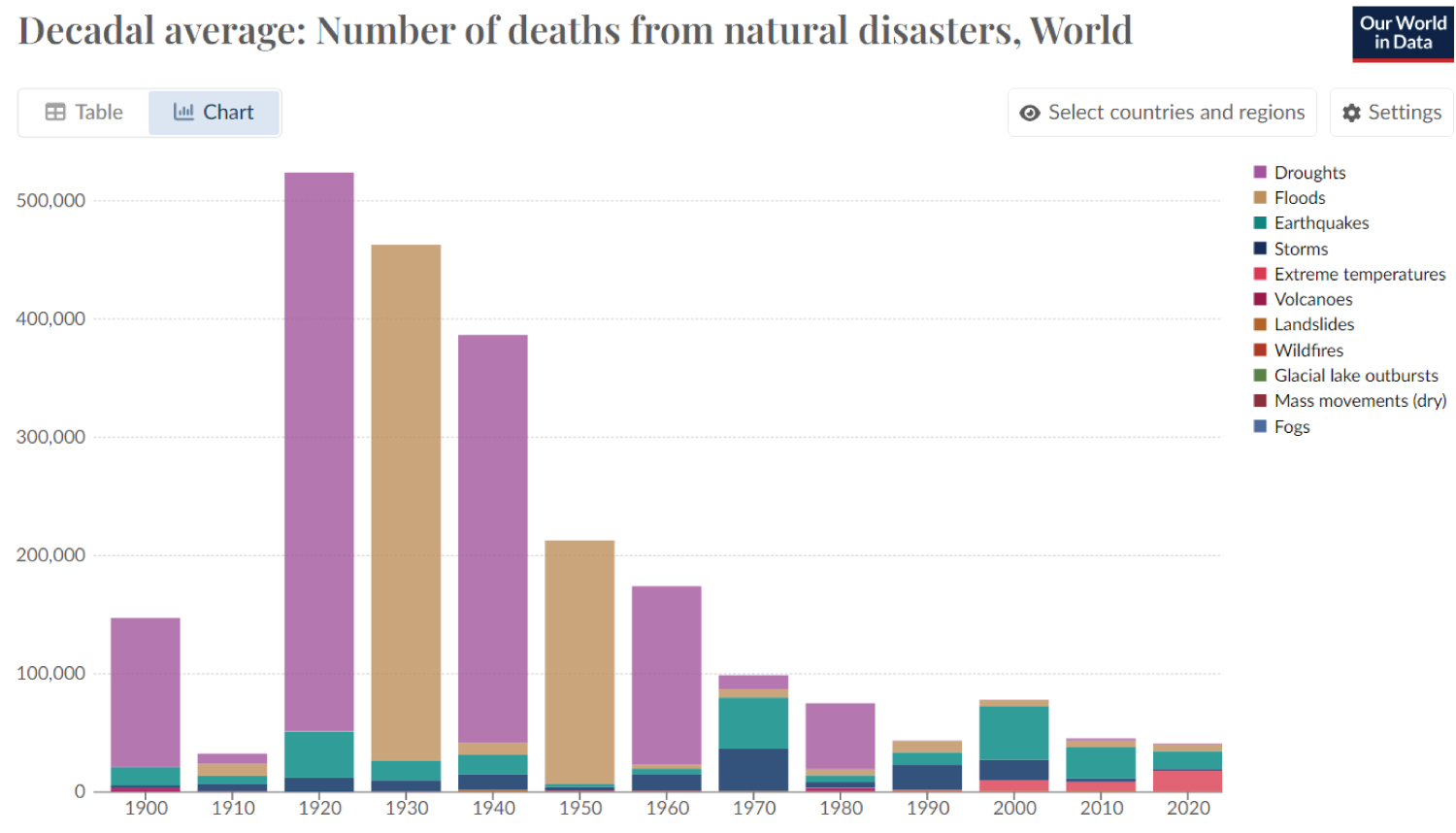 Figure 1: Deaths from natural disasters since 1900 to current decade, Ourworldindata.org.
View Figure 1
Figure 1: Deaths from natural disasters since 1900 to current decade, Ourworldindata.org.
View Figure 1
Table 1: 2001 to date natural disaster summary, Ourworldindata.org. View Table 1
In the US, 71% of the victims of hurricane Katrina that took place in 2005 in Louisiana, were older than 60 years of age and 47% were over the age of 75. According to grant makers in aging, many of the 200 people who died because of the hurricane in Mississippi were also older adults, while 70 nursing home residents died in their facilities [3]. The ones surviving and suffering with chronic illnesses remained cut off medication or treatment for a prolonged period; however, the death toll of these chronically ill patients who were unable to receive timely treatment and care has yet to be reported [4].
A very harsh reality of the death toll of older adults following natural disasters is apparent in Puerto Rico; an island struggling to recover from a series of brutal natural disasters constantly, as it is aging more rapidly than most places on Earth [5]. In 2017, hurricane Maria left 3,000 dead, the majority of which were over 60-years-old [6]. More than one fifth of the population is over 65, making the country’s share of older adults the 10 th in the world, together with Italy, Japan, and Germany, countries with much stronger economic bedrocks. The Puerto Rico territory is aging by compression, just like Kefalonia did immediately after the 1953 catastrophic earthquake, as the younger adults are leaving their country.
Natural disaster inducing mainly older adult deaths around the world include the 2011 Japan earthquake and tsunami, with 77% of deaths were people over 65-years-old [7]. In the great Hanshin earthquake in Japan in 1995, more than half the fatalities were over 60-years-old [8]. The same pattern of mortality was observed in the Guatemalan and Armenian earthquakes, in 2017 and 1988 respectively [9], as well as the Indonesian tsunami in 2004 [10]. It remains difficult to find accurate statistics of mortality of older persons affected in recent crises including 2018 earthquake in Indonesia and 2018 drought in East Africa [11]. Reports of the 2019 cyclone in East Mozambique, Malawi, and Zimbabwe report that older people and their families are among those most affected by the flooding. Another unfortunate mortality example is that of the North Korea earthquake in 2018 [12] and the 633 older adult deaths reported the same year after the British heat wave, only to exceed 2,800 deaths in adults over 65-years-old in 2022 [13].
None of these reports are surprising. During natural disasters, it is widely accepted that vulnerable adults are at higher risk than younger adults to die, to suffer injuries, not to receive enough assistance and support from public authorities or non-governmental organizations and to develop post disaster health problems [14,15]. Older adults with physical or cognitive disabilities are among the population subgroups that are vulnerable or disadvantaged during periods of crisis and social disorganization caused by disasters. For this population, minor barriers in normal circumstances can be significant handicaps in times of crisis. A particularly vulnerable part of the older adult population mostly affected by these challenges is the home bound older adult; socially isolated, mobility impaired, fighting against the vastness of the difficulty to survive and recover [16]. Vulnerability decreases the ability to prepare, respond and recover from catastrophic incidents. In the event of a disaster, when thousands of people need support, the difficulties of attending to the older population only grow.
The aftermath of a disaster in a frail older adult can potentially lead to additional re-victimization, increased dependency, declining health, poverty, and deprivation [17]. The trajectory thereafter depends on the support available. Various scenarios come to mind when studying the older adult population surviving earthquakes in Kefalonia; can older adults restart jobs or learn new skills? Can they survive being ignored and neglected by wrong allocation of relief? What is the morbidity and mortality cost of delayed care in chronically ill older adults? What is the cost on mental health as decency decreases after a natural disaster? Low mood, sadness, fear, anxiety, insecurity, frustration, sleep problems have all been documented in older adults in the aftermath of natural catastrophes [18].
Contrary to some commonly held beliefs that aging is associated with increased dependency, loss of self-control, ailment, incapacity, disengagement from life [19,20], and social isolations that makes older adults more vulnerable to life crises, some studies show that older earthquake survivors, for example, have a better and more positive mental health compared to younger counterparts in the wake of natural disasters [21,22].
The mental health of vulnerable populations can be undermined by natural disasters, Begum, et al. found a significant increase in mental health problems among older adults immediately after hurricane Sandy in 2012 [23]. However, the data in the literature is conflicting. In the aftermath of disasters, older people appeared to suffer greater psychological distress and were more likely to develop further symptoms compared to younger populations [15,24-26]. However, older people who survived the first year after a disaster coped with the long-term mental effects better than younger people. Studies show that older adults are less vulnerable to the psychological impacts of disasters compared to younger adults [27-29].
There seem to betway theories underlying the mental health trajectory of older adults after a natural disaster: The inoculation/maturation theory and the resource/exposure theory.
The inoculation theory suggests that previous experience with disaster provides inoculation against strong emotional reaction to similar disasters [30]. The maturation theory proposes that older adults are less emotionally reactive to post disaster distress, by developing mature coping styles.
Empirical data show that certain factors allow older adults to become resilient more effectively than other individuals; previous exposure to a natural disaster could buffer older adults negative experience of the event, thus leading to resiliency. Research suggests that survivors are relatively resilient and tend to report fewer emotional effects and prior experiences of disasters reduce adverse psychological effects. Age, life experience and prior experience of coping may lead to increased resilience [31-34].
The WHO in 2008 declared that older adults are resources for their families and communities during time of crisis. Their years of experience can make them models of personal resilience and sources of inspiration and practical knowledge. They voluntarily aid, care for grandchildren, neighbors, and support recovery. Including them in preparedness plans has been speculated to only benefit the whole community. This report compiled studies of older people around the world from natural disasters such as the tsunami after the Indian ocean earthquake in 2004, the heatwave in Europe in 2003, to Chernobyl in 1986 and Lebanon conflict in 2006. The studies concluded that the survival know how in emergencies that older adults have acquired helps them cope and provides inspiration and guidance to others (REF page 4/6).
Older adults are more vulnerate to natural disasters, and this includes the resource theory and exposure theory [30]. The resource theory says that elderly are not easily able to recover due to lower socioeconomic status and weak functional capacity. The exposure theory argues that older adults are not easily aware of the disaster magnitude, therefore they are more likely to experience greater sense of deprivation resulting from their own losses [18,35-37]. An aspect contributing to the increased mental decline in these circumstances is the so-called survivor’s guilt [38].
Preparedness plans and good recovery plans play a central role in defining either trajectory [39,40]. However, the trajectory is highly influenced by the society and community surrounding older adults. The role of society and community in survival and resiliency has gained attention most recently. A lot of importance is given to the structure of society and the ability to respond in caring ways supporting and changing frailty trajectories for the older adult population, at times, evidently more influential and substantial than government interventions [41].
The population is rapidly aging and a projection of people over 60 will be almost 2 billion by 2050 [42]. In parallel, climate change is increasing the frequency and death toll of natural disasters [43]. In 2050 we are seeing the prevalence of disability in developing countries to increase by 400% due to aging population [44]. With these realizations, first and foremost it is important to continue pressing for solid disaster plans and preparedness plans focusing on the geriatric population. The frailest part of the population needs to be accounted for and registries need to be created to identify those at highest risk who will require emergency evacuation and support during natural disasters. It is clearer now more than ever that these plans need to develop around geriatric focused care as the victims of natural disasters unfortunately are mainly this vulnerable population.
The older adults are largely invisible in disaster preparedness, rescue efforts and reconstruction programs. Most disaster management research concerning older adults focuses on the response and recovery phase. However, most recently a shift in the focus has been noted towards preparedness plans for older adults. Specifically, i n September 2023, the 20 th annual national preparedness month was marked; a time for everyone to recognize the importance of preparedness and to take steps to protect their loved ones was reached, with FEMA releasing the Disaster Preparedness Guide for older adults [40]. It is intended to support older adults and their caregivers by assessing needs, creating a plan, and engaging their network. It is a people centered product to help close the disaster preparedness gap and meet people where they are, specifically older adults from low income and rural communities and those living with disabilities and others with access and functional needs [35].
Older adults spend more time in their homes, and home is their most important place where they feel the most independent and safe. Programs are developing around the country offering primary care at home. An aspect of the preparedness plans needs to consider and utilize the help conferred by home based care providers. Home based care has filled the critical need for continuation of health care. This care can continue from the home in to shelters and hotels in the event of natural disasters. Maintaining health and healthcare in a disrupted environment after a disaster can help support chronically ill older adults and result in better outcomes [41]. Thus, as preparedness plans are created, it is important not to lose site of the important channel for health care delivered as home-based care. In fact, studies from the US Veterans health administration have provided strong evidence for the success of disaster preparedness activities with a federally supported organizational structure [45-47].
The impact and support offered by the community should also not be underestimated. Social support can have protective effects for all mental health outcomes, including anxiety, depression, and PTSD. Different studies show that older adults trusted their communities rather than the governmental agencies for primary source of support, such as local organizations able to tailor their effort to the needs and values of the community. Work from Dr. Kawachi and others shows how social connectedness is a protective factor during different types of natural disasters [48].
In conclusion, as older adults are the main victims of natural disasters, preparedness plans are starting to emerge. Questions remain: Have the views of older adults been specifically canvassed, while developing disaster preparedness plans? Is the field being mapped based on disciplines of psychology, sociology, health care, climate change and demography? The research addressing how disasters affect the older adults is still limited and more research needs to be supported in the future. Evidently, contrary to some commonly held beliefs that aging is associated with increased dependency, loss of self-control, ailment, incapacity, disengagement from life, and social isolation that may make older adults more vulnerable to life crises, some studies show that elderly earthquake survivors have a higher positive mental health compared to younger counterparts, in the wake of natural disasters. Further research is needed to study hubs of chronically affected areas by natural disasters, like the island of Kefalonia, which could serve clarify the trajectory of aging in place, mental health, resiliency, and frailty under the reign of repetitively impeding natural disasters. Results of this research can help design preparedness plans in the level of government, but most importantly, community, medical support personnel and home health workers.
Beyond supporting preparedness plans for natural disasters, research in this field can tremendously enrich the geriatric approach of the health care professional. In the practice of geriatric medicine, a new role emerges for the health care providers to inquire about survivorship from natural disasters, add this experience in one’s history and monitor accordingly to identify and support needs. The daunting mortality of our patients during natural disasters together with the robust immigration patterns we observe in our world, call for a change in the role of the healthcare providers who need to train to address the needs of such populations, including supporting post natural disaster syndromes. Our clinical approach should incorporate querying about exposure to natural disasters as we deliver care, and anticipate vulnerability, resiliency and tactics of survival that may affect our patients’ health trajectories. In taking care of older adults, it is of prime importance to be aware of surviving natural disasters to place the patient physically and mentally in a demographic with specific needs and the factors that could be influencing their frailty, mental illness, resilience, and post traumatic growth.
The authors would like to thank Prof A Germenis for the review and edits of this article.
No conflict of interest to declare.
Equal contributions.
No sponsors.