Background: Dementia presents a significant public health concern, with a high prevalence rate and considerable challenges in managing behavioural and psychological symptoms of dementia (BPSD) for patients with dementia (PwD).
Aim: The aim of this integrative literature review was to evaluate the effectiveness of BLT in managing BPSD for PwD.
Methods: A literature search was conducted using PubMed, CINAHL, and Web of Science. Studies were included if they involved people with dementia of any type receiving BLT of any methods, forms, duration, intensity and frequency, and had outcomes measures including BPSDs such as sleep disturbance, cognition, depression, and/or agitation. The Joanna Briggs Institute critical appraisal checklists were used to evaluate the methodological quality of the studies. Seven studies were included in the final review.
Results: Three themes were identified: The impact of BLT on sleep, the impact of BLT on mood and behaviour, and the impact of BLT on cognition. Studies found varied results, with subjective sleep showing consistent improvements but objective measures having mixed findings. BLT showed potential in enhancing mood and behaviour, especially in advanced dementia stages, though outcomes depended on dementia type and severity. Notably, BLT consistently improved cognitive function across studies, suggesting promise as a non-pharmacological intervention for cognitive enhancement in PwD.
Conclusion: The use of BLT in managing BPSD in PwD appears promising. Nevertheless, further research may be necessary to optimise the effectiveness of BLT across varied disease stages and types and strengthen the evidence for BLT as an effective intervention.
Light therapy, BLT, BPSD, PwD, Dementia, Nursing, Behavioural, Psychological, Cognition
The World Health Organization (WHO) [1] has reported a global increase in the proportion of older adults within populations across countries worldwide, where one in six people globally will be above the age of 60 years by 2030. As the aging population continues to increase, individuals are at a higher risk of experiencing complex health conditions often referred to as geriatric syndromes, such as dementia, depression, diabetes, hearing loss, cataracts, and osteoarthritis [1].
Dementia, a neurocognitive brain disorder, presents with cognitive and non-cognitive symptoms impacting daily functioning [2]. According to WHO [3], dementia is a major health problem among the elderly population globally, leading to disability, dependence, and mortality. With the aging population worldwide, there is an expected rise in the incidence of dementia, projected to increase from an estimated 57 million to 153 million cases by 2050 [3]. While age remains the primary risk factor of dementia, disparities in prevalence linked to gender are predominantly attributed to the longer life expectancy of females [4]. Furthermore, during their illness trajectory, approximately 80% of PwD will develop BPSD, with 97% developing at least one symptom within five years [5]. BPSD includes disruptive behaviour, mood, cognition, or perception symptoms such as agitation, irritability, anxiety, depression, apathy, and sleep disturbances [6].
In the 1940s, symptoms now defined as BPSD were observed to worsen during the late afternoon or early evening [7]. Thus, it was theorised that the primary reason for this phenomenon was the difficulty in retaining a spatial image under reduced light conditions [7]. This relation was subsequently termed “sundowning”, attributing the behaviour changes to the decreased light levels when the sun sets [8]. While the concept of sundowning syndrome is commonly used today, its definition remains unclear, and the underlying mechanism is not fully understood [8]. Evidence suggested that the underlying reason could be due to the dysregulation of circadian biology and alternations in circadian rhythms associated with the decreased light levels [9]. Furthermore, according to current clinical and preclinical research, the circadian rhythm, which is influenced by light levels may have an impact on mood, sleep, cognition, and aggressive behaviour [10]. Consequently, inappropriate light levels and wrestling dysregulated circadian rhythms could potentially be a plausible explanation for the sundowning syndrome [10].
BPSD can interfere with clinical management, causing distress to patients and caregivers, and is associated with diminished quality of life [11]. PwD has a higher risk of institutionalisation and the presence of BPSD can further complicate the treatment due to the special treatment requirements and additional behavioural and medical complications, leading to extended hospitalisation stays and increased costs [12]. In clinical settings, BPSD inflicts greater stress on caregivers and is commonly described as more challenging to manage than the cognitive deficits typically associated with dementia with agitation and sleep disturbances as prominent symptoms [12]. BPSD symptoms pose complications during routine nursing tasks including issues such as catheter removal and food throwing, and can lead to physical and verbal incidents for nursing staff during the delivery of nursing care, contributing to job dissatisfaction, burnout, and increased attrition rates among nursing staff [12-15].
Current BPSD treatment options are limited, raising concerns about side effects and insufficient research support [15]. In clinical settings, antipsychotic medication are commonly used for the management of BPSD but have limited effectiveness and significant adverse side effects such as the increased risk of hospitalisation, falls, and mortality [16]. Therefore, guidelines from experts favour non-pharmacological interventions for BPSD due to their significant influence on overall BPSD outcomes and the absence of adverse events [17]. However, restraints, one of the most commonly used non-pharmacological interventions to manage BPSD, have been proven to further exacerbate BPSD and lead to numerous physical injuries [18]. Furthermore, healthcare providers often face emotional conflict regarding the use of restraints and their potential dehumanising impact on the patient’s dignity and autonomy [19]. Therefore, non-pharmacological treatment involving environmental and behavioural interventions such as bright light therapy could potentially serve as first-line alternatives.
BLT offers a feasible non-pharmacological treatment for BPSD in PwD, yielding positive outcomes in sleep, agitation, and cognitive functioning [20]. Older adults with dementia experience reduced general sensory input, demonstrating decreased sensitivity to the impact of light on the suprachiasmatic nucleus (SCN), and limited exposure to bright environmental light [21]. BLT can potentially reverse degenerative alterations in the SCN, which form the biological foundation for circadian rhythm disturbances such as sleep-wake rhythm and rest-activity in PwD [21]. Most clinical settings maintain consistently low light levels which might not provide an adequate stimulus for the circadian clock to synchronise with the 24-hour day [21]. The appropriate light dose can effectively influence circadian rhythms, thereby improving factors such as sleep quality, depression, functional status, or behavioural issues in PwD [20]. BLT involves controlled light delivered through various means such as natural outdoor sunlight, or artificial indoor light sources such as light boxes, ceiling lights, or stimulation dawn-dusk illumination [22]. Furthermore, it can be administered at different times of the day such as in the morning, afternoon, or intermittently throughout the day, to prevent the patients from sleeping during those periods [23]. Moreover, BLT is non-invasive and has minimal side effects, where users can engage in various activities within their field of vision while undergoing BLT, making it an ideal non-pharmacological intervention easily implementable across institutional settings [24].
Since the 1900s, BLT has been a subject of research in managing BPSD in PwD, particularly in sleep and circadian rhythms [25]. While some reviews have investigated its effects on cognition, mood, and behaviour, the reported findings are inconsistent. The identification of an effective and feasible non-pharmacological treatment, such as BLT, for managing BPSD in PwD is imperative for tailored nursing care. Utilising such behaviour management intervention can enhance the individual's quality of life, and ensure patient safety during the nursing care delivery. Additionally, introducing BLT can potentially reduce the stress and burden associated with caregivers for informal caregivers such as family members and formal caregivers such as nurses. Nursing management can consider instituting BLT as part of policy changes in improving holistic care of PwD and nurses’ job satisfaction. Therefore, this review seeks to offer current insights and robust evidence regarding the effectiveness of BLT in managing BPSD in PwD, facilitating the development of new knowledge for informed clinical practice, enhancing the quality of life in PwD, and improving dementia care.
The literature search was done following the PRISMA 2020 guidelines [26]. Three databases (PubMed, CINAHL, and Web of Science) were searched using keywords such as: “dementia”, “light therapy”, “behavioural”, “psychological”, and” cognition” with the use of Boolean operators to identify relevant studies. Search filters were applied across the databases to obtain studies that were published between 2019-2023, and in English.
A total of 81 articles were identified from the databases. Mendeley Reference Manager was used for the removal of 12 duplicates gathered from the search results [27].
The remaining articles were subjected to title and abstract screening. Studies were included if they involved people with dementia of any type receiving BLT of any methods, forms, duration, intensity and frequency, and had outcomes measures including BPSDs such as sleep disturbance, cognition, depression, and/or agitation. Research articles that did not match the aims of the present literature review, articles focusing on participants with other neurological conditions, and studies that included other non-pharmacological interventions were excluded, together with non-full text and non-English articles published before 2019 (Table 1). After screening, 11 articles remained for full-text review. Two articles were excluded as one did not qualify as a primary studies while the other was conducted in a home setting. Ultimately, nine articles were considered eligible for this review [20,25,28-34]. Figure 1 shows a PRISMA flowchart illustrating the literature search flow.
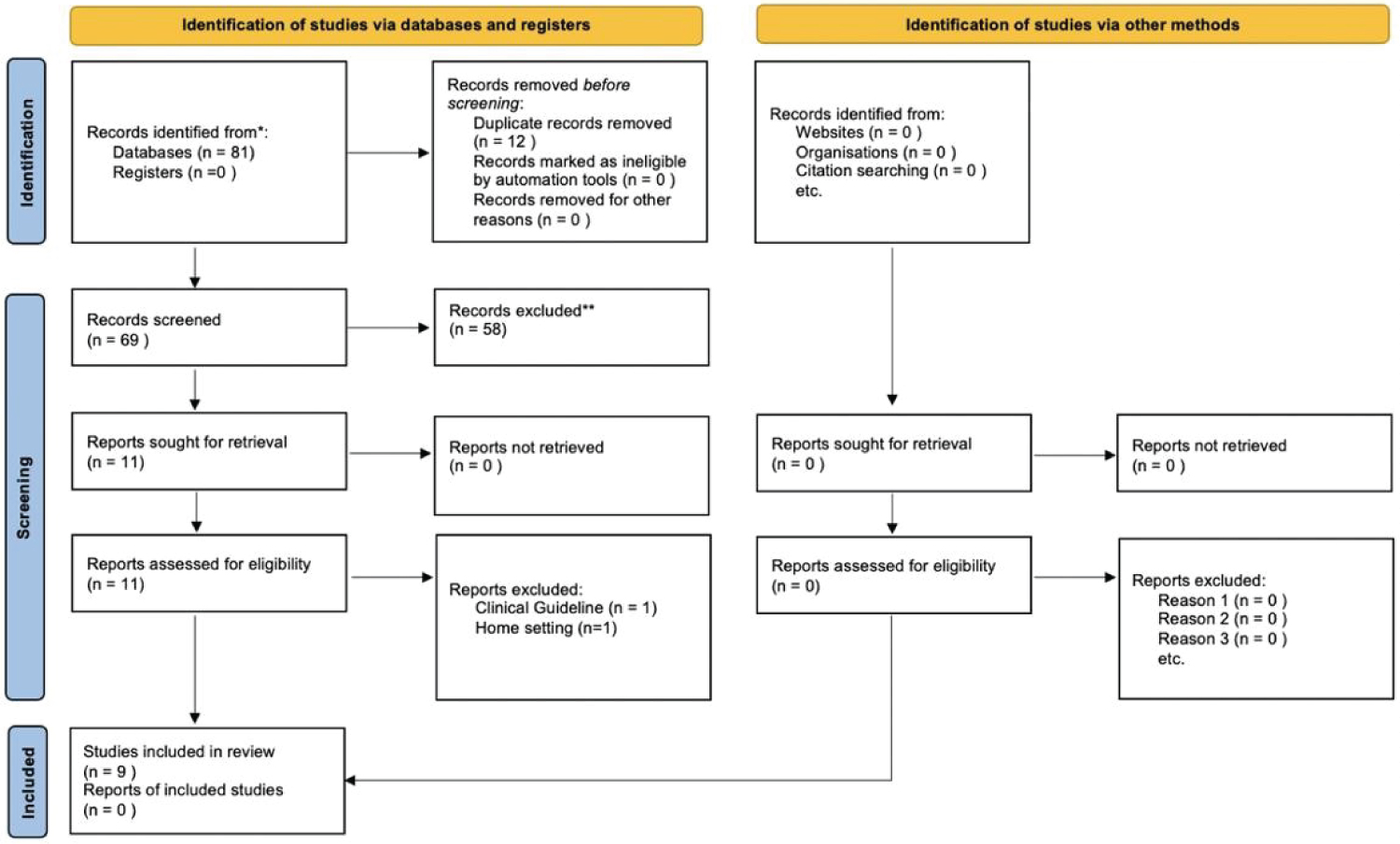 Figure 1: PRISMA 2022.
View Figure 1
Figure 1: PRISMA 2022.
View Figure 1
Table 1: Inclusion and exclusion criteria. View Table 1
The nine studies were evaluated for their methodological quality using the Joanna Briggs Institute (JBI) critical appraisal tools. According to the JBI [35] level of evidence for effectiveness, all nine RCTs in this review were classified as Level 1.c, denoting the highest quality of evidence. While JBI levels of evidence offer valuable ranking, it is not a definitive measure of study quality and should not preclude the need for critical appraisal and clinical reasoning when applying evidence [36]. Therefore, the methodological quality of the nine studies will be further evaluated using the JBI checklist for randomised clinical trials [37], critically appraising the sample size, population characteristics, validity and reliability of measurement tools, data collection method, study design, and risk of bias. Each study was given a quality percentage by first scoring it out of 13 before converting the score into a percentage. Scores were obtained by summing the number of items on the checklist with a “Yes” response. The quality appraisal are summarised in Table 2.
Table 2: Joanna Briggs Institute critical appraisal checklist for randomised clinical trials. View Table 2
Notably, all nine studies had a relatively small sample size of less than 50 participants and power analysis was implemented in only four studies [20,25,30,32], with all recruiting fewer participants than calculated. Consequently, these small sample sizes could potentially compromise the robustness and generalisability of the results, resulting in insufficient statistical power to accurately detect the true effects of BLT. Additionally, a gender bias was evident, with a higher proportion of females, which could confound the result due to gender-specific responses to the light interventions [38]. Furthermore, while concerns were raised regarding the validity of watch actigraphy for objective sleep measurement, the homogeneity and reliability of the remaining measurement tools, assessing subjective sleep, mood and behaviour, and cognition, were deemed valid and reliable. Lastly, despite the potential risk of biases in majority of the studies, the lack of allocation concealment and participant blinding is unlikely to undermine the validity of the results or introduce significant bias due to the nature of the light intervention. However, two studies failed to demonstrate true RCT due to the absence of proper randomisation, lacking an appropriate washout period in their crossover RCT [28], and conducting a single-arm intervention study without a control group [29]. These deviations from the standard RCTs were not accounted for in the conduct and analysis which, therefore, introduced high risks of biases. This, in turn, suggests that the reliability and validity of the findings of both studies could be compromised and the evidence may not accurately reflect the true effects of the study, overall indicating a low quality of evidence. Consequently, these two studies were eventually excluded due to poor methodological quality [28,29].
Overall, based on the assessment of methodological rigor, four of the seven studies achieved a score of 70% and above, indicating high-quality evidence [20,25,30,32]. Among the remaining five studies, three attained at least 50% of the predefined appraisal criteria [31,33,34], indicating moderate-quality evidence. The two studies that were excluded, scored below 25%, indicating low-quality evidence [28,29].
The main characteristics of the studies are summarised in Table 3. All seven studies in this review were RCTs, including the standard RCTs [30,33,34], cluster RCTs [20,25,32] and crossover RCTs [31]. Six studies were conducted in Western countries including Italy [30], Norway [20,25,32], the United States of America [31], and Iran [33], while one was conducted in Asia, specifically South Korea [34]. A total of 315 participants were included, with the largest group consisting of 69 participants [25,32]. The majority of participants were females, and the mean age of the participants was 81 years. Four studies only included patients with AD [30,31,33,34], while the remaining included participants with several types of dementia such as VD, Lewy Body Dementia and Frontotemporal Dementia [20,25,32]. Most studies included individuals with moderate to severe dementia [20,25,31-33].
Table 3: Characteristics of studies. View Table 3
The intervention characteristics varied in the type of light, intensity, duration, and frequency. Among the seven studies, BLT interventions can be grouped into three main categories: standard visible light, light-emitting diodes (LED) light, and laser light. Most of the studies employed standard visible light interventions, such as normal bright light [31,32] and blue-enriched light [30,34]. In contrast, three studies incorporated LED light sources, including LED helmet devices and ceiling-mounted LED panels [20,25], while the remaining study used low-level laser therapy [33]. BLT exposure duration ranged from ten minutes to 24 hours, spanning from three to seven days a week, and lasting two to 24 weeks. The intensity of BLT ranged from 550 lux to 10,000 lux. In three studies, the delivery of light intervention and illuminance was tailored according to each participant’s circadian phase [30,31], while in another three studies, the light intervention provided varying illuminance throughout the day [20,25,32]. The remaining study involved participants receiving the light intervention at the same intensity for only one hour each morning [34]. Control conditions generally implemented low light intensities, ranging from 30 lux to 300 lux, with a some studies requiring participants to wear blue- attenuating sunglasses [34] or turning the light intervention off [33]. In assessing the impact of BLT on sleep, both objective sleep measures, like Watch Actigraphy, and subjective sleep measures, including Sleep Disturbance Index (SDI), and Pittsburgh Sleep Quality Index (PSQI) were employed. Agitation levels were assessed using Cohen-Mansfield Agitation Inventory (CMAI) scores, while depression was measured using Cornell Scale for Depression in Dementia (CSSD) scores, Cornell Scale for Depression in Dementia Korea Version (CSSD-K) scores, and Beck Depression Inventory. The overall mood and BPSD were evaluated through the Neuropsychiatric Inventory-Nursing Home Version (NPI-NH), the Korean Version of the Neuropsychiatric Inventory Questionnaire (KNPI-Qs), and the Interact short scale. Cognition was assessed using the Mini-Mental State Examination (MMSE). Standardised questionnaires and scales were mainly administered by nursing staff [20,31,32], except in studies where assessors were not specified [33,34] or tools like KNPI- Qs involved patient’s informal caregivers [34]. Notably, in the study by Cremascoli, et al. [30], patients completed sleep questionnaires, specifically PSQI, under medical supervision.
Three themes were identified: 1) The impact of BLT on sleep; 2) The impact of BLT on mood and behaviour, and 3) The impact of BLT on cognition. Table 4 presents a summary of the studies of each theme.
Table 4: Thematic analysis. View Table 4
Five studies investigated the effect of BLT on sleep outcomes such as sleep quality, rest-activity cycles, and circadian rhythm [25,30-32,34]. Objective sleep outcomes using actigraphy yielded no significant effect on sleep duration or rhythm [25,30-32,34]. However, all four studies that measured subjective sleep outcomes using proxy-rated questionaries such as PSQI and SDI, reported significant improvements in terms of subjective sleep and total sleep time quality [30-32,34]. Variations in outcomes could be dependent on the means of assessing sleep, with significant treatment effects as measured by proxy-rated PSQI and SDI, as opposed to assessing sleep through actigraphy. Actigraphy and proxy-rated sleep measurements represented a distinct approach to measuring sleep. It is possible that actigraphy may not exhibit the same degree of sensitivity to change as proxy-rated measurements. Furthermore, low participant activity levels could contribute to the lack of effect, as actigraphy could potentially misinterpret periods of wakefulness as sleep due to minimal movement, potentially missing subtle variations in sleep and wakefulness [32]. Nonetheless, the most used characteristics of BLT among these five studies that resulted in positive effects on sleep measures were LED lights programmed to provide varying illuminance and correlated colour temperature throughout the day, with a peak of 1000 lux, 6000 K between 10 a.m. and 3 p.m., for 24-weeks [25,32]. Overall, while BLT had a positive impact on subjective sleep outcomes, it did not show a significant effect on objective sleep measures.
Four studies investigated the impact of BLT on mood and behaviour focusing on overall BPSD and behavioural symptoms such as depression and agitation [20,30,31,34]. Firstly, Figueiro, et al. [31] reported significant improvement in agitation as measured by CMAI scores. In the four studies that measured the effect of BLT on depression, two studies reported a significant difference in CSSD scores [20,31] while the other two studies conducted by Kim, et al. [34] and Cremascoli, et al. [30] did not find any significant improvements in CSSD-K score and Beck Depression Inventory respectively. Lastly, overall BPSD was assessed using the NPI-NH and KNPI-Qs in three studies [20,30,34]. While Kolberg, et al. [20] reported significant improvements in overall BPSD, as measured by NPI-NH scores, the remaining two studies, conducted by Cremascoli, et al. [30] and Kim, et al. [34], did not report significant differences in overall BPSD. The conflicting findings may be attributed to variations in dementia severity among the participants in the four studies. The studies conducted by Figueiro, et al. [31] and Kolberg, et al. [20] focused on moderate to late-stage dementia, while the other two studies focused on early-stage dementia [30,34]. As highlighted by García-Martín, et al. [39], neuropsychiatric symptoms such as agitation and depression may be more prevalent in the later stages of dementia, which further reinforces the probability that BLT might have a more prominent impact on mood and behaviour in PwD with advanced stages of dementia. Notably, among the four studies, positive outcomes in mood and behaviour were associated with tailored BLT characteristics including LED light peaking at 1000 lux between 10 a.m. and 3 p.m. daily for 24 weeks [20], and white light 550-700 lux daily for 14-weeks [31]. Overall, BLT had a positive impact on mood and behaviour through varied outcomes. The positive effects were evident in individuals with more advanced stages of dementia but not in the early stages of dementia.
Three studies investigated the impact of BLT on cognition and consistently reported significant improvement in cognition, measured by MMSE scores [30,33,34]. Cremascoli, et al. [30] suggested that the observed improvement in cognition in PwD could have been attributed to the participants’ early stage of dementia. Yamadera, et al. [40] reported that the observed reduction in damage to the suprachiasmatic nucleus and retinogeniculate pathway during early dementia stages compared to later dementia stages may account for the cognitive improvement due to the early stage of dementia amongst the participants. However, incongruities in dementia severity, with two studies focusing on mild to moderate dementia stages [30,34] and one focusing on late-stage dementia [33], raised concerns about the generalisability and the validity of the finding, particularly in the study by Kheradmand, et al. [33]. Utilising MMSE as the primary outcome measure for cognitive assessment in the study conducted by Kheradmand, et al. [33] may potentially pose a limitation due to its sensitivity and specificity for detecting mild dementia stages, instead of advanced dementia stages [41]. Notably, the most used characteristics of BLT among these three studies involved blue-enriched light ranging from 30 to 10,000 lux for 20 to 60 minutes, daily over 2 to 4 weeks [30,34]. Overall, BLT has demonstrated positive effects on the cognitive functioning of PwD.
Firstly, regarding the impact of BLT on sleep outcomes, studies consistently reported positive results in subjective sleep outcomes such as sleep quality and sleep disturbance, while objective sleep outcomes such as sleep-wake rhythm showed no significant positive effects across all studies [25,30-32,34]. These findings align with previous literature reporting beneficial effects on subjective sleep quality such as sleep duration as documented by improvement of PSQI scores but no difference in objective sleep measures like rest-activity rhythms [42].
In mood and behaviour assessment, particularly for overall BPSD, agitation, and depression, the results varied. Studies with advanced dementia stages showed favourable outcomes [20,31], contrasting with studies with early- stage dementia that found no significant differences [30,34]. This aligns with a previous study reporting that BLT has greater benefits in mood and behaviour for individuals in advanced stages of dementia compared to those in the early stages [43].
Cognition improved significantly in participants in all three studies that examined the impact of BLT on cognition [30,33,34]. These results were consistent with previous studies [44,45], which similarly indicated positive effects on cognitive function.
A variety of BLT characteristics was observed across all studies. However, the most used characteristic of BLT among the studies that resulted in overall positive effects on the outcome measures, particularly sleep, mood, and behaviour measures was the use of LED light for 24 weeks.
There were several gaps found in the review of the literature. Firstly, heterogeneity among the intervention characteristics and dementia types and severity led to generally heterogeneous findings. Consequently, the overall evidence on the effectiveness of BLT for BPSD remains inconclusive. Therefore, as suggested by Nizamutdinov, et al. [46], focusing future research on moderate to late-stage dementia may yield more meaningful results, as participants with advanced stages of dementia might exhibit more noticeable improvements compared to the participants in the early stages of dementia. Additionally, employing measurement tools sensitive to changes in the later stages of dementia would enhance the accuracy of assessing BLT's impact. While MMSE is widely acknowledged as a reliable and valid measurement tool for assessing cognitive function, its greater sensitivity and specificity toward detecting mild dementia may limit its effectiveness in assessing cognitive changes in the advanced stages of dementia [47]. Future research could consider incorporating a diverse set of cognitive assessments for a more comprehensive evaluation, particularly in cases of moderate to severe dementia. Moreover, the possibility of measurement errors in light exposure duration makes it challenging to ascertain whether participants were exposed to the intended duration of light exposure. In most studies, the specific measurement of light exposure for each participant was not conducted. Instead, many of these studies relied on estimations of exposure, which were derived from standardised light meter measurements and subjective data, such as nurses’ reported duration spent in the room. Therefore, to enhance the accuracy of measurement of the duration of light exposure, the development of objective light measurement tools such as wearable devices could be introduced to objectively measure the duration and amount of light to which participants are exposed.
This review found heterogeneity among the intervention characteristics and dementia types and severity has led to generally varied outcomes. While BLT exhibits promise as a therapeutic intervention for improving sleep, mood, behaviour, and cognition in PwD, it is strongly recommended that further research be conducted to determine the optimal implementation and efficacy of BLT across diverse populations and disease stages. By addressing these research gaps, future studies can contribute to advancing our understanding of BLT's potential as a non-pharmacological intervention for enhancing the well-being and quality of life of PwD.