Treatment of patients with fractures of the bones of the leg in an outpatient setting occurs under conditions of a forced increase in the axial load on the injured lower limb. The aim of the study was to determine the conditions for the formation of periosteal callus of the shoulder and lower leg and to assess the effect on its formation of the time frame for fixation of bone fragments in people of different ages under the conditions of treatment in the outpatient setting.
Two groups of patients with closed diaphyseal bone fractures were examined using the Ilizarov method. The first group consisted of 29 patients with fractured shoulders aged from 24 to 94 years (43 ± 3). The second is 36 patients aged from 17 to 84 years (44 ± 4) with fractures of the bones of the leg in the conditions of Ilizarov treatment. All patients were treated for the first 2 weeks in inpatient, and later on in the outpatient setting.
It was found that increased motor mode and axial load on the limb in the conditions of outpatient treatment lead to an increase in the period of fixation of bone fragments as compared with the previously recommended G.A. Ilizarov standards by 60% and the appearance of periosteal callus. At the same time, the size of callus on the tibia is relatively more than on the shoulder by 43% (p ≥ 0.05), while the timing of fixation of bone fragments was not statistically significantly different. Increasing the size of callus is favorable for reducing the time of fixation of fragments in patients with shoulder injury. In patients with a leg injury of working age with an increase in the number of past years, the size of the periosteal callus also became larger, however, this increase only influenced the reduction of fixation time when the shadow size of the callus reached 360 mm2. At the same time, on the lower legs, the time of fixation of fragments, unlike patients with shoulder herbs, after the formation of callus, ceases to depend on the initial micromobility of bone fragments that took place after the application of the Ilizarov apparatus. As a result, no selective adverse effect of an increase in the load on the lower leg was revealed on the terms of treatment of patients with lower leg injuries on an outpatient basis.
Fractures of the Bones of the Leg and Shoulder, Ilizarov method, Outpatient treatment, Periosteal callus
With an increase in the life expectancy of the population in the structure of morbidity, the proportion of the pathology of people in the older age groups increases. They often experience osteoporosis, a decrease in tissue vascularization, the expression of chondrogenic and osteogenic genes, which, in the treatment of limb bone fractures, leads to loss of their mass and strength, as well as delayed the formation of bone regenerate (callus) [1-4]. Therefore, the total length of stay in the hospital positively correlates with the patients' age [5].
Fracture treatment in the elderly is complicated by a decrease in the ability to form bone tissue. The loss of osteoblasts in the aging skeleton is explained by a decrease in the number of mesenchymal stem cells and their ability to differentiate into precursors in the direction of the osteoblast line [6].
However, not all authors recognize the effect of age as such on the timing of adhesion of bone fragments [7]. In particular, the declining quality of life of older patients is important [8].
We set ourselves the task of conducting a comparative analysis of the effect of the age factor on the Ilizarov treatment of injuries of the shoulder and lower leg on an outpatient basis, when locomotor activity and axial load on the injured lower limb increase significantly. Education with periosteal callus in people with injuries to the bones of the limbs does not always occur. It is assumed that it is aimed at creating additional fixation of bone fragments. For us, the most important is the question: what is the relationship of the size of the periosteal callus of the shoulder and tibia with the age of the patients [9].
The aim of the study was to determine the conditions for the formation of periosteal callus of the shoulder and lower leg and to assess the impact on its education of the timing of fixation of bone fragments in people of different ages under conditions of treating patients on an outpatient basis.
Two groups of patients with closed diaphyseal bone fractures were examined during the Ilizarov treatment period. The first group consisted of 29 patients with fractures of the humerus. The age of patients is from 24 to 94 years (43 ± 3), the period of fixation of the bone by the Ilizarov apparatus at the time of examination is from 3 to 94 days (22 ± 6). The second group consisted of 36 patients aged from 17 to 84 years (44 ± 4) with fractures of the bones of the leg. All patients were treated for the first 2 weeks in inpatient, and later - on an outpatient basis with follow-up visits from a traumatologist 1 every 2 weeks.
The size of the periosteal callus was determined planimetrically from the area of its X-ray image on the day of the end of the period of fixation of bone fragments.
When using a strain gauge station and a B7-73/1 voltmeter, a sensor signal was recorded, allowing to determine the change in the distance between the spokes coming out of the bone above and below the fracture zone, in increments of 5 kgf increasing axial load on the limb, which allowed determining the micromodularity of fragments of the humeral or tibial bones [8].
All surveyed signed an informed agreement to participate in the survey and publish its materials without identifying their identity.
Statistical processing of research results was carried out using the Microsoft-Office Excell-2010 data analysis package. The normal distribution of empirical samples was confirmed using the modified Kolmogorov criterion. The tables show the average values of the indices and the mean square error.
When analyzing the dynamics of changes in indicators, methods of correlation and linear regression analysis were used. In order to take into account the effect of multiple comparisons, analysis of variance was applied using the Scheffe criterion for independent samples. To assess the statistical significance of differences in the results when analyzing two samples, we used the Student's t-test for independent samples.
The diameter of the humeral diaphysis was found to be 21.8 ± 0.7 cm. The transverse size of the tibia was 12% larger (24.4 ± 0.5 cm, p ≤ 0.05). The average area of the X-ray image of the periosteal callus of the shoulder was 153 ± 16 mm2, and the tibia 219 ± 27 mm2 (p ≤ 0.05). In this case, the duration of the period of fixation of fractures of the shoulder and tibia was, respectively, 87 ± 4 and 94 ± 7 days.
It was noticed that in the treatment of patients with shoulder injuries in the hospital, the periosteal bone reaction was practically absent. When treating on an outpatient basis with increasing age up to 40 years, the area of callus shadow tended to decrease. In subsequent years, the size of periosteal callus with increasing age became larger (Figure 1).
 Figure 1: Age dynamics of the size of the periosteal callus of the humerus.
View Figure 1
Figure 1: Age dynamics of the size of the periosteal callus of the humerus.
View Figure 1
In patients with this group, with an increase in the size of periosteal callus, the periods of fixation of bone fragments became less (Figure 2).
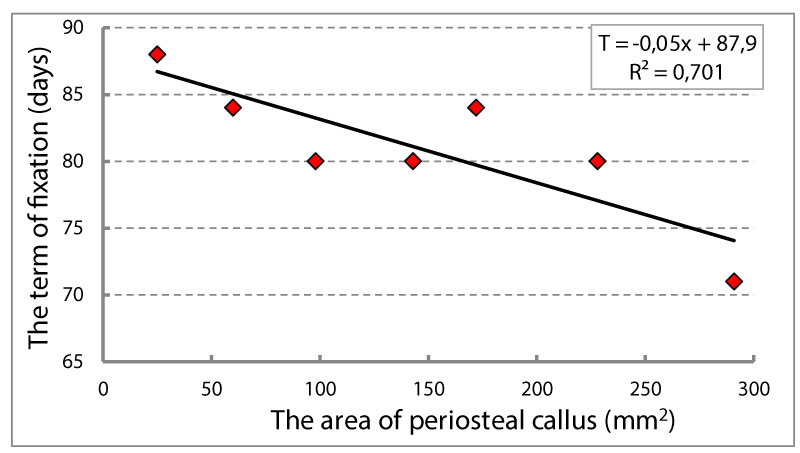 Figure 2: The relationship of the size of the periosteal callus of the shoulder and the duration of the period of fixation of bone fragments.
View Figure 2
Figure 2: The relationship of the size of the periosteal callus of the shoulder and the duration of the period of fixation of bone fragments.
View Figure 2
In patients with group 2 with a leg injury, the size of the periosteal bone regenerate is greater, the older the patients are up to 55-60 years old (Figure 3). However, at an older age, periosteal callus sizes were relatively smaller.
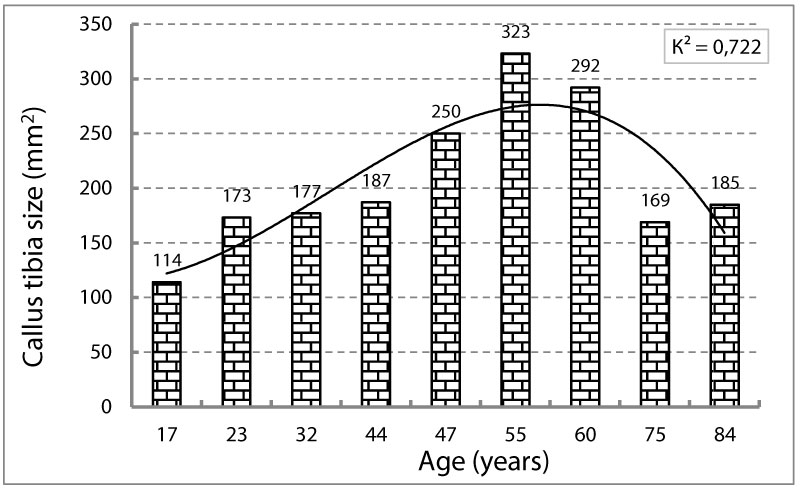 Figure 3: Age dynamics of periosteal tibial callus size.
View Figure 3
Figure 3: Age dynamics of periosteal tibial callus size.
View Figure 3
In patients of the 2nd group, an increase in the size of callus began to lead to a decrease in the duration of the fixation period only when reaching sizes greater than 360 mm2 (Figure 4).
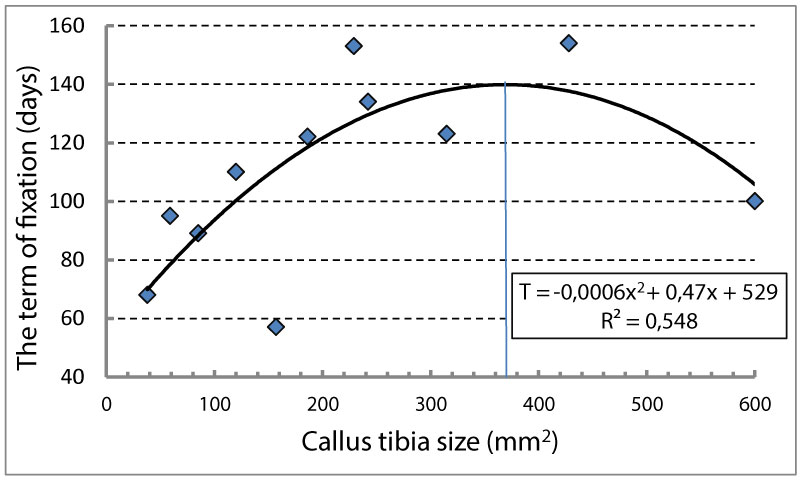 Figure 4: The dynamics of the size of the tibial callus at the end of the fixation period during treatment in a hospital and clinic.
View Figure 4
Figure 4: The dynamics of the size of the tibial callus at the end of the fixation period during treatment in a hospital and clinic.
View Figure 4
In patients with shoulder injuries after osteosynthesis, the smaller the initial micromotion of the bone fragments, the shorter the period of fixation (Figure 5). In patients of the 2nd group, the initial micromotion of the bone fragments did not have such a pronounced effect on the duration of the fixation period.
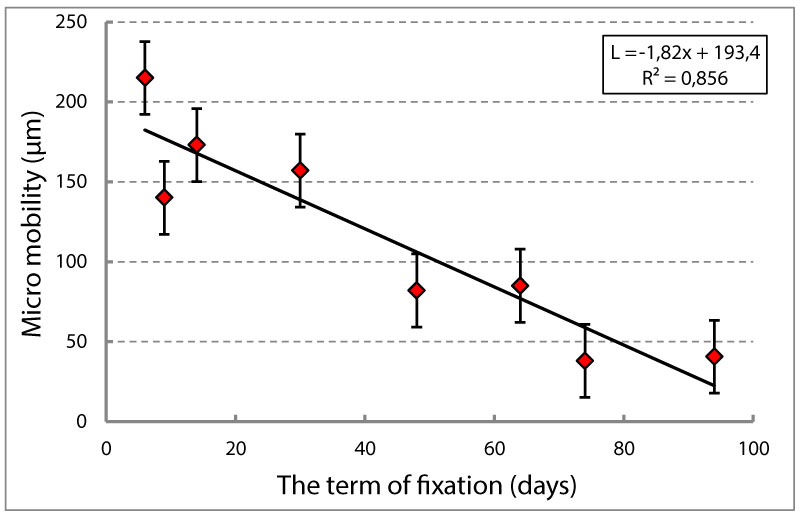 Figure 5: The relationship of the initial stiffness of fixation of fragments of the humerus and the timing of their fixation.
View Figure 5
Figure 5: The relationship of the initial stiffness of fixation of fragments of the humerus and the timing of their fixation.
View Figure 5
Thus, the increased motor mode and the axial load on the limb in the conditions of outpatient treatment lead to an increase in the period of fixation of bone fragments as compared to the standards recommended earlier by G.A.Ilizarov. At the same time, the size of callus on the lower legs is relatively more than on the shoulder, by 43% (p ≥ 0.05), and the timing of fixation of bone fragments is not significantly different (by 11%).
Increasing the size of callus is favorable for reducing the time of fixation of fragments in patients with shoulder injury. In patients with a leg injury of working age with an increase in the number of past years, the size of the periosteal callus becomes larger, but this increase begins to affect the reduction of fixation periods only when the size of periosteal callus is more than 360 mm2. At the same time, the terms of fixation of fragments on the legs, unlike the treatment of injuries of the shoulder, after the formation of callus, cease to depend on the initial micromutation of the bone fragments after applying the Ilizarov apparatus.