Recent technological advancements and accumulating surgical experience have led to a higher interest in orthopedic minimally invasive surgery. This study aims to present the feasibility of posterior mini-incision for partial hip prosthesis compared with total hip prosthesis.
We enrolled 15 patients (nine females, six males) who presented with a geriatric hip fracture between 2013 and 2014. While 11 of the fractures were in the collum femoris, 4 were intertrochanteric fractures. Hemiarthroplasty with a mini-incision was applied to all patients.
In all patients, a mini-incision of 8.5-cm mean length was used. The mean surgical duration was 67.4 min, and the mean blood loss was 526 mL. We observed no neurovascular damage in any patient resulting from the limited exposure. Moreover, no postoperative complication was reported, and there was no mortality during the follow-up.
This study suggests that the advantages and disadvantages of classic and mini-incision methods should be comprehensively assessed, and the most appropriate method should be selected for each patient.
Hip fracture, Mini-incision, Partial hip prosthesis, Total hip prosthesis
Treatment of geriatric fractures aims to mobilize patients as soon as possible and regain pre-fracture function, while preventing medical and surgical complications as far as possible. In the treatment of geriatric fractures, especially in elderly patients with low-level activity, the application of partial endoprosthesis is a relatively acceptable treatment option [1]. However, total hip arthroplasty is recommended for patients with a history of hip arthritis [2]. Geriatric hip fractures, a significant health problem in the elderly, have high mortality and morbidity [3].
Surgical approach to the hip has different choices, each of which has specific advantages and disadvantages [4]. As in all fields of surgery, orthopedics is witnessing a growing interest in minimally invasive surgery and mini-incisions [5]. Although several studies have reported the use of mini-incision in total hip arthroplasty, limited studies have reported the use of mini-incision in hemiarthroplasty for hip fractures [6,7]. This study aims to present the feasibility of posterior mini-incision for partial hip prosthesis compared with total hip prosthesis and discuss our experience demonstrating that mini-incisions can be used without a special retractor in the application of hemiarthroplasty in geriatric hip fractures, while also attempting to minimize complications in elderly patients with several comorbidities besides the fracture.
In this study, we enrolled 15 geriatric patients [nine females (60%) and six males (40%); mean age: 77.3 (64-89) years] who presented with a hip fracture and were treated with hemiarthroplasty with posterior mini-incision between 2013 and 2014. This study protocol was approved by the Institutional Review Board, and we obtained informed consent from all patients.
While 11 of the fractures were in the collum femoris, 4 were intertrochanteric fractures. On the mean postoperative day 5, patients were discharged from the hospital and were followed up on day 45, 6 months, 1 year, and 4 years. The fracture types were Garden Type III (5 patients) and Garden Type IV (6 patients). In addition, the intertrochanteric fractures were unstable per the Evans classification. In 4 of 11 patients with collum femoris fractures, a straight stem bipolar endoprosthesis was applied, whereas a unipolar endoprosthesis was applied to the remaining 7 patients.
In 3 of 4 patients with intertrochanteric fractures, a unipolar endoprosthesis with lift support was applied, whereas a straight stem unipolar endoprosthesis was applied to the remaining 1 patient. Anesthesia was applied as general to four patients, spinal to three patients, and epidural to eight patients. In addition, a visual pain scale (Visual Analog Scale, VAS) was assessed preoperatively and at 24 h postoperatively. All patients were made to lie on the healthy hip and operated in the lateral decubitus position. After appropriate preparation and draping, the borders of the trochanter major were identified. Based on the patient’s size, an incision of 7-10 cm was made in the posterior third of the trochanter major. Notably, the proximal third of the incision was over the acetabulum, and the distal two-thirds was over the trochanter major. After incision, under the skin and the tensor fascia lata, the trochanteric bursa was excised, and the external rotators were exposed by a marginal internal rotation of the hip. While no attempt was made to locate the sciatic nerve in any of the patients, knowing that the localization was close to this nerve, caution was taken to evade damage. At this stage, tagging sutures were applied to the external rotators after placing a tapered retractor under the gluteus medius and minimus tendons. After that, the external rotators and capsule were cut, and bleeding vessels were cauterized. The gluteus maximus tendon was not cut in any patient. The femoral head was removed with a corkscrew. Finally, the removed femoral head was measured, and the correct size was determined with trial heads after checking fracture fragments and degeneration in the acetabulum.
Next, a length of gauze was placed in the acetabulum, and the femoral canal was prepared by bringing the hip into flexion, adduction, and internal rotation, and where feasible by pushing toward the proximal femur incision. In some cases, the femoral neck had to be shortened with an electric saw. Then, the canal was reamed after placing two Hohmann retractors under the proximal femur. The trial reduction was made, generally by scraping, in some cases by placing the prosthesis and in doubtful cases by checking under fluoroscopy. After the canal was systematically washed and dried, the cement was applied then the prosthesis was put into place (Figure 1).
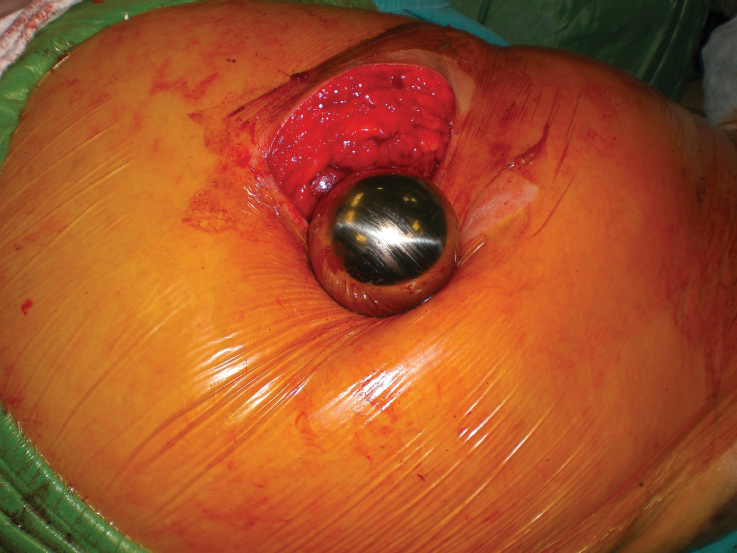 Figure 1: The intraoperative placement of the prosthesis in the mini-incision. View Figure 1
Figure 1: The intraoperative placement of the prosthesis in the mini-incision. View Figure 1
In all cases, a cemented prosthesis was applied. Then, bleeding was checked following reduction and tests. In all cases, the external rotators were repaired with sutures passing through the holes opened in the trochanter major. In addition, the capsule was repaired. After that, a hemovac drain was placed, and the layers were closed (Figure 2). Of note, a special retractor developed for mini-incisions was not used in any case. Figure 3 presents postoperative radiography of the case.
 Figure 2: The postoperative view of the incision length. View Figure 2
Figure 2: The postoperative view of the incision length. View Figure 2
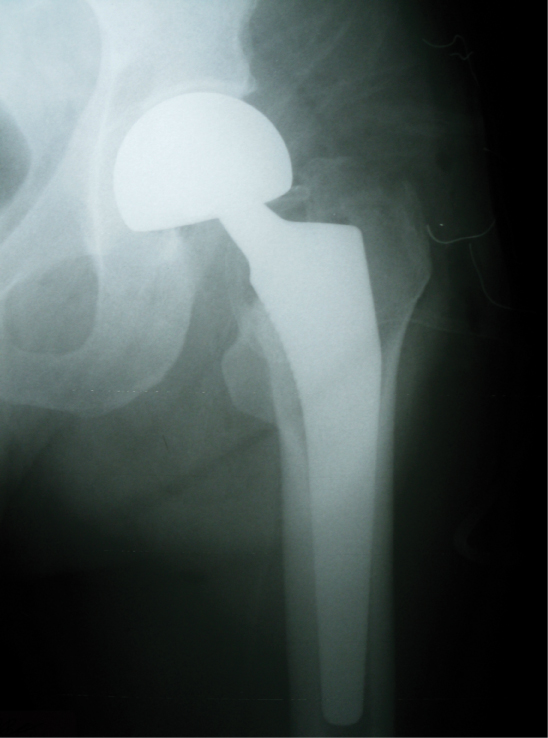 Figure 3: Postoperative view of radiography. View Figure 3
Figure 3: Postoperative view of radiography. View Figure 3
In this study, mini-incisions were used in all patients, with the posterior approach allowing for a length of 8.5 (range: 7-10) cm (Table 1). Extending the incision was imperative in any case. In the postoperative period, we observed no neurovascular damage resulting from limited exposure. The mean surgical duration was 67.4 (range: 52-80) min, which was slightly longer than operations made with classic incisions. The mean blood loss was 526 (range: 481-611) mL. The mean preoperative VAS score was 6.5, and the mean postoperative 24-h score was 2.8. The mean time to hospital discharge was 5 (range: 3-8) days. All patients, except 1, were mobilized on postoperative day 2 and were weight-bearing on the operated side. There was no postoperative complication, and we observed no mortality during the follow-up.
Table 1: Data of patients included in this study. View Table 1
Hip fractures accepted for major operations involve major incisions. However, over time, surgeons have realized that every incision incurs trauma, which permanently damages the tissue of patients. Perhaps, a smaller incision could cause less damage to the skin tissue. Thus, attempts should be made to cause the least damage to muscles, tendons, and ligaments.
Surgeons should always remember the crucial roles of the gluteus maximus and minimus in the abductor mechanism of the hip. However, a small incision does not always imply little damage to tissues and patients overall. Notably, in the period marking the beginning of the learning curve for surgeons, increased bleeding from the medulla is likely because of the extended operating time, improper positioning of the implant because of an inadequate view, and higher damage to the surrounding tissues from the retractor.
Despite the availability of multiple approaches for mini-incisions, it would be better for surgeons to select a mini-incision to be used in some cases where a classic incision has been more often used previously. We felt more comfortable using a posterior mini-incision in cases where we had previously used a modified Gibson incision. The leading disadvantage of the posterior incision is the high rate of dislocation. Nevertheless, discounting the past, since we started seriously repairing the posterior capsule and external rotators, we have not noted any posterior dislocation [8,9].
Mardones, et al. reported that the muscle damage in arthroplasty caused by two incisions was higher than that of arthroplasty with a mini-incision [10]. However, Meneghini, et al. upon comparing Smith-Petersen and posterior mini-incisions reported that the muscle damage was higher in posterior incisions [11]. Pagnano, et al. operated on patients with a double incision on one side and a single posterior mini-incision on the other side and recommended the mini-posterior approach [12].
The mini-incision application of partial endoprosthesis for hip fractures is more advantageous than the total hip replacement, as there is no need for reaming of the acetabulum in the partial application; thus, the incision is more than adequate for partial endoprosthesis. In addition, thin patients are more suitable for this approach. In the total hip replacement, as it is critical to ream the acetabulum at an angle of 45°, the distal part of the cut needs to be extended if a patient is overweight and no specifically designed reamer is available. Experienced surgeons use classical posterior incision do not encounter difficulties with posterior mini-incision. Although the reduction of operating time has been mentioned in the literature, surgery might take longer, especially in the period marking the beginning of the learning curve for surgeons, which might create problems for patients with other medical comorbidities [13].
Another reported advantage of mini-incisions is minimal blood loss [14]. In this study, we observed no marked decline in the amount of blood loss compared with classic incisions because bleeding occurs more during the cutting of the external rotators and while preparing the medulla for the prosthesis. As no difference exists at these stages between classic and mini-incisions and we accepted bleeding between under the skin and the muscles in a long incision as inconsequential, we did not observe any evident elevation in bleeding from a small incision. Perhaps, the not-so-small blood loss could be attributed to the prolonged operation time. With the application of hypotensive anesthesia, the amount of bleeding might be much lower.
In this study, a significant reduction was determined in the VAS scores of patients in the postoperative period and, meanwhile, a decreased need for analgesia; this enables earlier mobilization of patients, raising of the feet and legs, and, thus, a lower risk of the development of deep vein thrombosis. One of the disadvantages of mini-incision is the incorrect placement of the component because of insufficient exposure [15]. To avoid this in this study, suspected cases were checked under fluoroscopy after the reduction of the hip with the trial component. If the fluoroscopy is prepared beforehand, it only takes a short time to apply, which does not adversely affect the surgical duration and the position of the prosthesis, and the reduction can be checked and revised simultaneously. However, based on a study published in Sweden, total hip arthroplasty made with mini-incision is more advantageous in terms of short-term costs [16].
In conclusion, making a small incision might not always offer maximum benefit to all patients. This study suggests that it is more appropriate to select the most beneficial method for each patient on a case-by-case basis.