Determine long-term care facility (LTCF) risk factors for a COVID-19 outbreak and recommend strategies for closing gaps in facility preparedness through a multidisciplinary team assessment carried out on site.
Data was obtained during visits to 14 LTCFs, completion of a standard assessment tool through interviews with site staff and leadership, and tours of the facility campus.
In all five dimensions of preparedness (staffing, professional medical support, infection control, engineering controls and testing), the degree of readiness was inversely proportional to the number of residents infected. Those facilities with high scores experienced no outbreaks while those that scored low suffered infection; in many cases, extremely high infection rates. The greatest difference in category preparedness between LTCFs with and without infection was the presence of professional medical support on site.
Long-term care facility infection prevention is multidimensional and adherence to goals is likely benefited by the presence of a physician (medical director) and an advanced practice provider (APP) on site.
COVID-19 prevention, Outbreak, Long-term care facilities, Skilled nursing homes, Professional medical support
Long-term care facilities in Washington State continue to struggle with COVID-19 and associated mortality eight months following the first reported case in a skilled nursing home (SNH) in King County [1]. Currently, of the roughly 237,000 deaths in the United States [2], more than 63,000 were in nursing home residents [3], representing 27% of all deaths from this infection nationwide. The case fatality rate for seniors in nursing homes is 22.6%, far higher than the country at large (2.4%). LTCF residents are 9.4 times more likely to succumb to COVID-19 than the general population [2,3]. There also remains wide variation between states. Massachusetts, for example, has the highest rate (55.3%) and Vermont, the lowest (0.36%) [3]. As of November, Spokane County has seen 141 COVID-19 deaths among 906 LTCF cases [4]. County deaths for the same period are 216 [5]. LTCF deaths, therefore, represented 65% of all deaths in the County.
There are many reasons why LTCF residents are at the highest risk of infection and mortality from COVID-19. For example, serious challenges exist in maintaining robust and reliable facility staff. Long-term care and services for frail and disabled Americans suffer serious and chronic workforce shortages. A survey report by the Agency for Health Care Administration revealed a vacancy rate among registered nurses and licensed practical nurses of 16% and 11% respectively. More concerning is the high turnover rate found among staff nurses (41%), licensed practical nurses (49.9%) and certified nurse assistants (65.6%) [6]. There is evidence that high rates of professional staff turnover in nursing homes are significantly associated with quality of care challenges [7]. Another factor impacting resident risk for infection derives from serious comorbidities [8]. In our experience in Spokane County, and those related in other published studies describing LTCF outbreaks, primarily in Washington State [1,9], there is growing evidence that nursing home resident comorbidities, such as dementia, correlate strongly with coronavirus mortality [10]. Additionally, the prolonged and close contact required of caregivers in these settings during activities of daily living (ADL) [11] would negatively impact transmission rates between staff and residents. Furthermore, elderly patients suffer from immunosenescence, an age-related deterioration in the ability to fight infection and develop immunity after vaccination [12]. The importance of pursuing robust infection prevention measures in LTCFs should not be diminished by the delivery of a COVID-19 vaccine. Older adults have often been excluded from a substantial number of COVD-19 clinical and vaccine trials therefore precluding optimal evaluation of efficacy and adverse effects in this population [13].
Additionally, this population has always been at significant risk for infection. This has been amply demonstrated by their high susceptibility to outbreaks of infectious disease, most commonly influenza, Noroviruses, Salmonella and group A Streptococcus. For example, the median infection rate for influenza in elderly care facilities is 33% with a median fatality rate of 6.5% [14]. It is not surprising, therefore, that nursing home residents are at dramatic risk for COVID-19 and death.
Herein we report observations by the Mann-Grand staff Veterans Affairs Medical Center (MGVAMC) COVID-19 Assessment Consultation Team (ACT) following evaluation of 14 LTCFs in eastern Washington and Northern Idaho. We evaluate the degree of facility preparedness and performance during the current COVID-19 pandemic in terms of staffing, professional medical support, infection control, engineering controls, and testing. Factors most likely to improve LTCF infection prevention and mortality are identified and inform recommendations for improvement. Nine of the facilities were Skilled Nursing Homes (SNHs). The remaining five included one Adult Family Home (AFH) and four Assisted Living Facilities (ALFs), herein referred to collectively as Adult Quarters Facilities (AQFs).
Following a significant outbreak in one of the first skilled nursing homes in Spokane County to experience COVID-19 transmission, and leveraging the experience gained by MGVAMC staff caring for these residents during hospitalization, a multidisciplinary team was convened. The ACT was made up of a senior geriatrician, infection preventionist, registered nurse, engineer, emergency manager and administrative officer. The goals of the team were to evaluate the preparedness of LTCFs to prevent COVID-19 infection and limit transmission. A further goal was to make recommendations for improvement. In this observational study, the degree of preparedness for an effective COVID-19 response was determined by formal assessment of five broad categories: staffing adequacy, professional medical support, infection control, engineering controls and testing adequacy. Standard data was collected for each LTCF visited and scored (Table 1).
Table 1: COVID-19 preparedness assessment & scoring tool. View Table 1
Staffing was determined by ACT interviews with facility leadership to determine their degree of confidence that current staffing levels were sufficient to prevent or limit COVID-19. Medical support was based on the presence or absence of an APP and/or medical director (physician) in the facility at least once a week. Infection control preparedness scoring was determined by an assessment of staff understanding of, and adherence to CDC guidelines, and compliance with isolation procedures (if positive cases) or existence of an effective isolation plan in place (no cases). The extent of staff training in infection control procedures including doffing and donning of personal protective equipment (PPE), availability of necessary PPE and days-on-hand supplies also contributed to scoring in this category. Engineering controls were scored based on a facility's ability to create at least one negative pressure room and one negative pressure wing. Air filtration and physical barriers to COVID-19 units were assessed. Adequate access to viral testing was also evaluated and scored.
Consultation was provided to LTCFs upon request by facility leaders. The ACT was publicized by the Spokane Regional Health District (SRHD) in Eastern Washington and the Panhandle Health District in North Idaho to facilities in their regions. Subsequent to our site visit, recommendations were made by written report to LTCF directors. Findings and recommendations remained strictly confidential. Reports were shared with LTCF leadership only. The ACT Emergency Manager was responsible for ensuring timely communication with local and state departments of health and the Federal Emergency Management Agency (FEMA). All consultation services were rendered free of charge with regular phone follow-up after the initial visit. At least three team members, including the senior geriatrician, were present at the LTCF during all consultation visits; other members participated virtually when unable to visit the facility. A wide range of LTCFs were visited including corporate, private and state facilities in fulfillment of the fourth mission of Veterans Affairs, which is to improve the nation's preparedness for response to national emergencies.
Among the nine SNH facilities, four had no residents with COVID-19 and the remaining five had an infection rate between 7.4% and 79.0% at the time of the first ACT visit (Table 2). The average number of days between the first peak in COVID-19 cases in Eastern Washington and Northern Idaho (April 1) and the first ACT visit was 175 days in facilities with no cases and 106 days in those with outbreaks. Total preparedness scores and percent of maximum score achieved by category in SNH facilities with and without infections are shown. There was an average number of 59 residents in nursing homes with no infections and 74 with outbreaks. The average percentages of maximum score achieved in SNHs with no infections were staffing (75.0%), medical support (Figure 1 and Figure 2) (87.5%), infection control (97.9%), engineering controls (62.5%) and testing (100%). For facilities with COVID-19 outbreaks, the findings were staffing (30.0%), medical support (30%), infection control (76.7%), engineering controls (30%) and testing (80%) (Figure 1). The three SNHs with the highest infection rate had no allied healthcare professional (AHP) or physician presence in the facility at least one day a week. Three of four SNHs with no infection had both a healthcare professional and physician in the facility at least one day a week. The remaining infection-free facility had a physician only on-site on a regular basis (Figure 2).
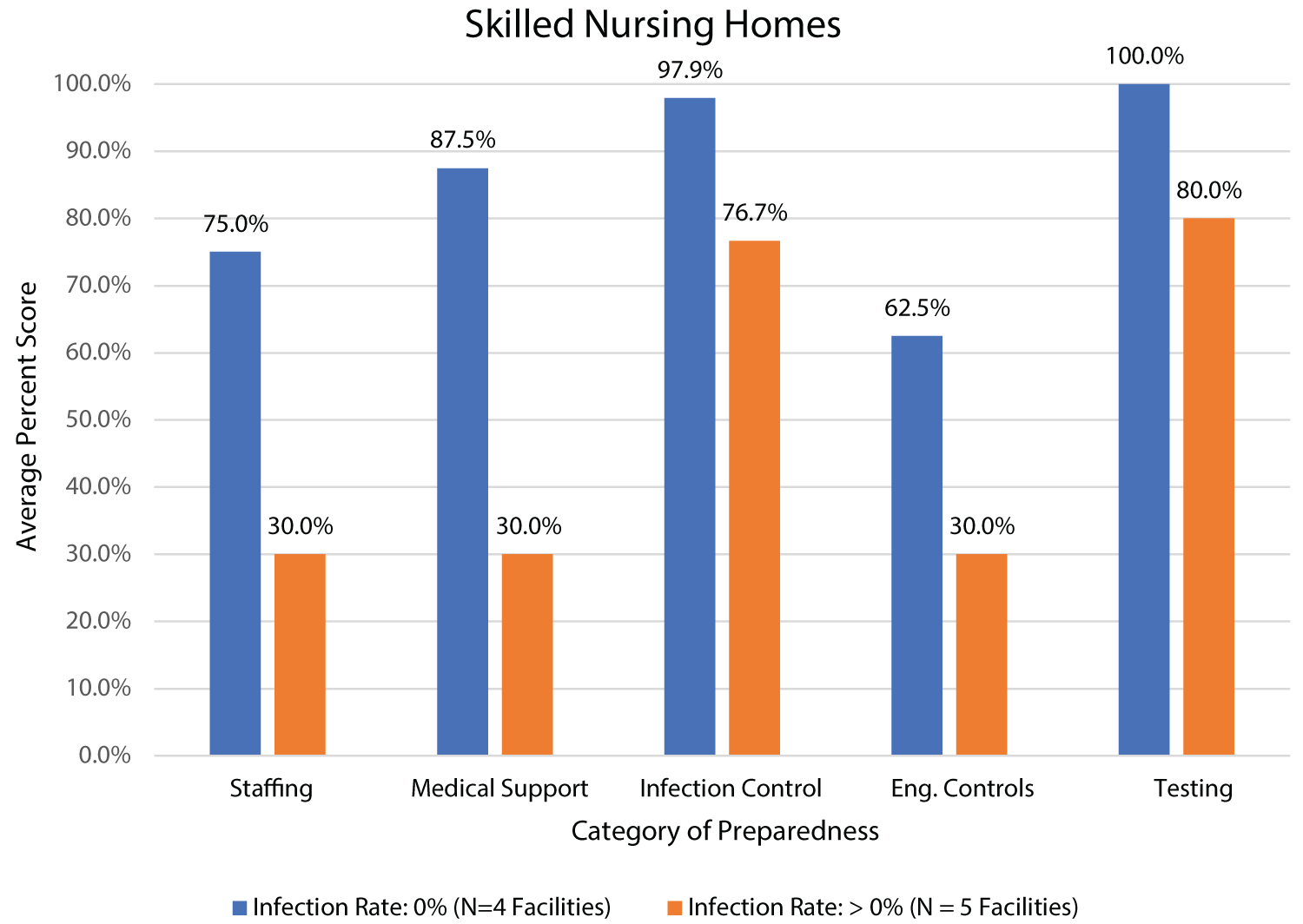 Figure 1: Comparison of average scores by preparedness category between facilities without and with COVID-19 cases.
Figure 1: Comparison of average scores by preparedness category between facilities without and with COVID-19 cases.
View Figure 1
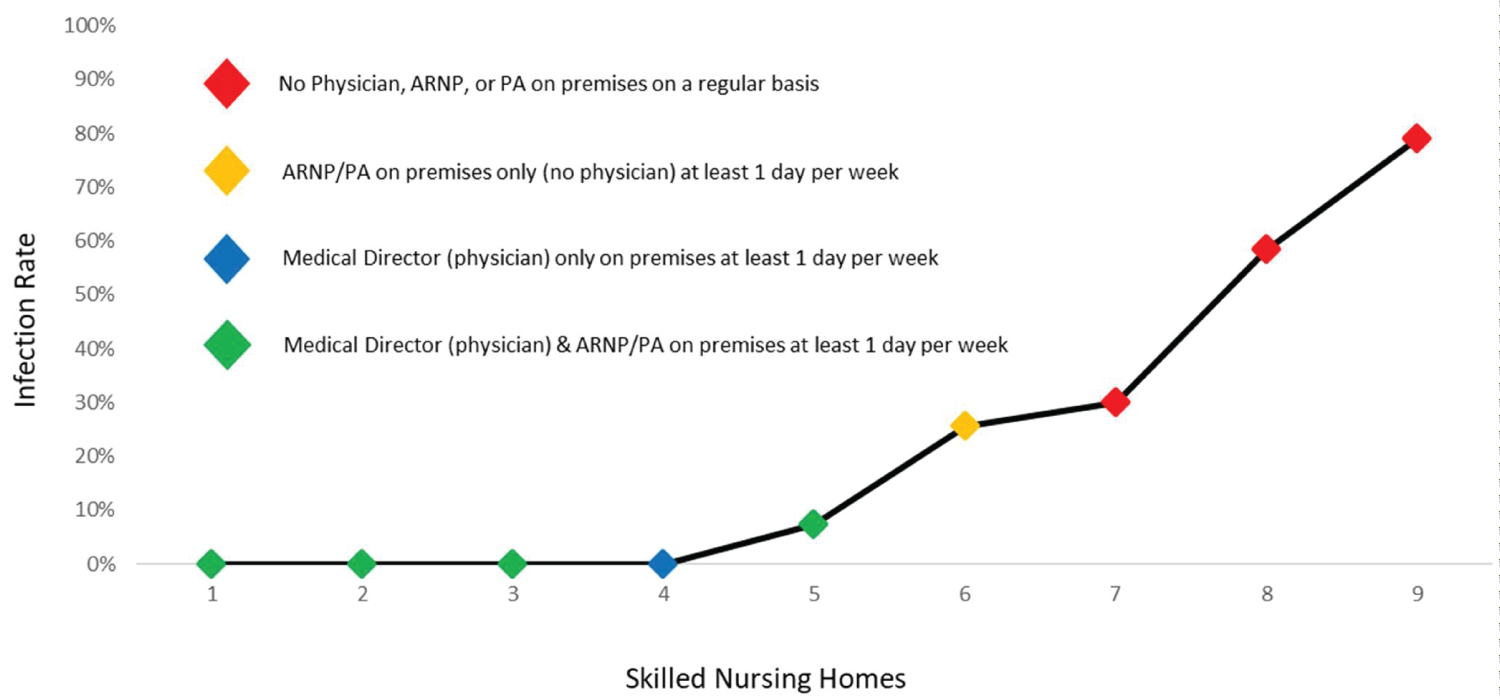 Figure 2: Skilled nursing homes infection rates and professional medical support.
View Figure 2
Figure 2: Skilled nursing homes infection rates and professional medical support.
View Figure 2
Table2: Skilled nursing home background & preparedness assessment. View Table 2
Similar results were scored by the five Adult Quarters Facilities (Table 3). Among these five (one Adult Family Home and four Adult Living Facilities), two had no residents with COVID-19 and three had infection rates between 7.7% and 100%. The average number of days between the regional peak in COVID-19 cases and the first ACT visit to AQFs with no cases was 148 days and 157 days in those with outbreaks. The average number of residents was 32 in facilities with no cases and 39 in those with outbreaks (Table 3). The average percentages of maximum score achieved in the facilities with no infections were staffing (75.0%), medical support (Figure 1 and Figure 2) (50.0%), infection control (85.4%), engineering controls (25.0%) and testing (100%). In facilities with COVID-19 outbreaks, the results were staffing (66.7%), medical support (0%), infection control (62.5%), engineering controls (8.3%) and testing (66.7%) (Figure 3). Three of the five facilities experienced a COVID-19 outbreak and in all three, there was no APP or physician on the premises at least one day per week. Of the two facilities with no infections, one had an APP and physician present at least one day per week, one an APP only (Figure 4).
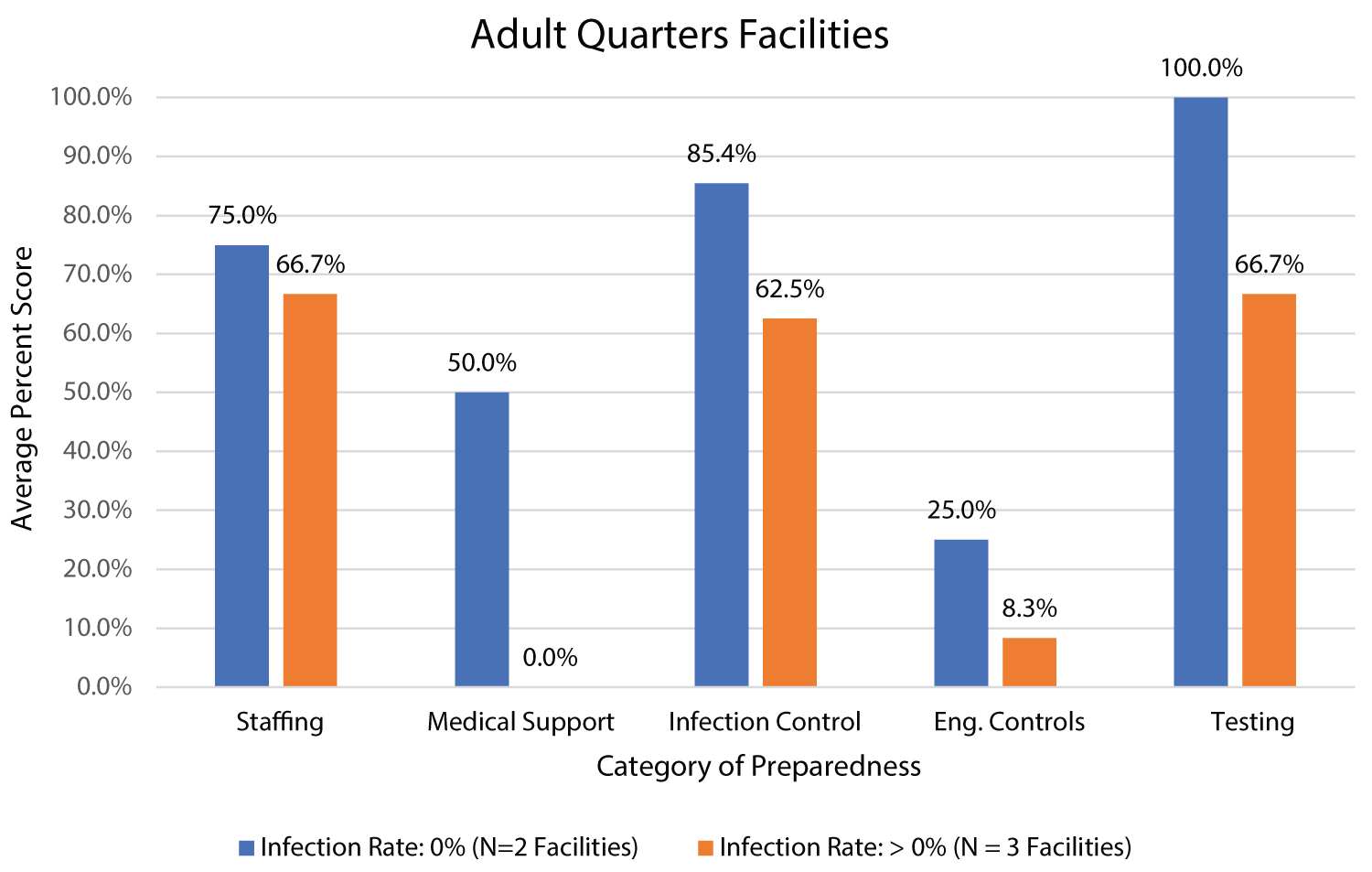 Figure 3: Adult quarters facility by infections rates and assessment categories.
Figure 3: Adult quarters facility by infections rates and assessment categories.
*: Adult quarters facilities include adult family homes and adult living facilities.
View Figure 3
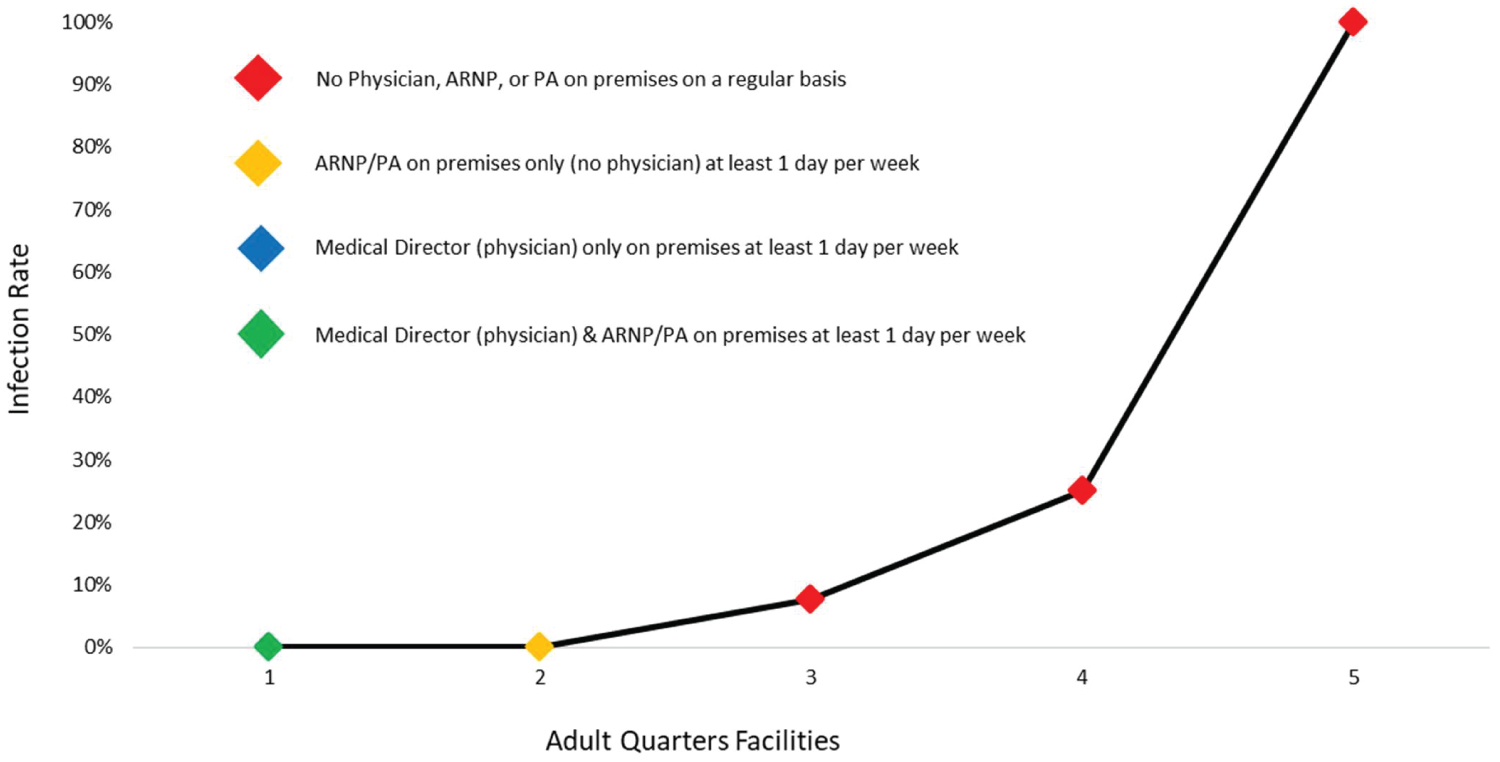 Figure 4: Adult quarters facilities infection rates and professional medical support.
View Figure 4
Figure 4: Adult quarters facilities infection rates and professional medical support.
View Figure 4
Table 3: Adult quarters facility background & preparedness assessment. View Table 3
Although the highest COVID-19 case fatality rate is, by far, among residents of long-term care facilities, there is surprisingly little in the literature about improving professional medical support as a strategy for risk mitigation. Compared to hospitals and large integrated healthcare systems, nursing homes accumulate woefully little aggregated clinical data from which to draw conclusions and clinical recommendations. In the current study, we have had the privilege of visiting a series of LTCFs in Eastern Washington and North Idaho. As a result of these consultations, a better understanding has been gained of the challenges pandemic's pose for these facilities, and in many cases, the outstanding degree of preparedness achieved. Interestingly, the temporal pattern of COVID-19 spiking in community cases has been largely the same for Eastern Washington and North Idaho with a first relatively small spike occurring around April 1 [15,16].
The temporal relationship between the first peak in COVID-19 cases in our region (April) and the dates of consultative visits to LTCFs reveal that facilities with outbreaks were visited closer to the initial community spike. Another regional peak was experienced in July and there is a current prolonged and serious increase in confirmed positive cases at the time of this writing, four months later [15,16]. Although it may appear that the longer time goes by after initiation of community infection, the greater the likelihood of LTCF outbreaks, in fact, the facilities that were, collectively, exposed the least amount of time, had higher rates of transmission and outbreaks. Because ACT visits were voluntary on the part of LTCFs, facilities with outbreaks were more likely to request consultation sooner. There was also a tendency for larger facilities to experience COVID-19 outbreaks, likely a reflection of greater numbers of staff and greater opportunities for infection transmission to residents.
For this analysis, we divided nursing home data into two main groups for comparative purposes. One group consists of nine traditional skilled nursing homes and the other consists of one adult family home and four adult living facilities, collectively referred to as Adult Quarters Facilities. We further compared data within each group by examining facilities with and without resident infections at the time of the consultative visit.
In each of the five categories, there was a consistent tendency for lower scores of COVID-19 preparedness among facilities with infection in both SNHs and AQFs (Figure 1 and Figure 3). Of the four SNH facilities with no infections, all but one had both an APP and physician on the premises at least one day a week; one facility had a physician only. The three with the highest infection rate had neither on site.
The average preparedness assessment for SNH facilities having resident infections was 121 of 200 points (60.5%) as compared to 177.5 of 200 points (88.8%) for those facilities without infection. Notably, in the four facilities with no infection and one with a low infection rate (7.4%), the level of professional support in-house was high. The three highest infection rates are associated with the absence of regular in-house professional medical support (Figure 2). The average preparedness assessment for AQFs having resident infections was 91.7 of 200 points (45.8%) as compared to 140 of 200 points (70%) for those facilities without infection. Three of five Adult Quarter Facilities experienced outbreaks; there was no professional medical support on board (Figure 4).
Study limitations include the small number of LTCFs evaluated and the observational nature of the study. Facilities were not chosen randomly for consultative visits but rather by request. The data collected was not subject to statistical analysis and significance testing. Nonetheless, interesting trends were discovered, and these may inform best practices for outbreak avoidance in our area.
Not surprisingly, the data reported here is consistent with a positive relationship between robust preparation and the successful prevention of COVID-19 transmission in long-term care facilities visited by the Assessment Consultation Team. What is less expected is the suggestion medical support plays such an important role in keeping LTCFs free from infection, in particular, the presence of a physician medical director and/or advanced practice provider. Their presence, on site, appeared to have a salutary impact on COVID-19 outbreaks in our sample of facilities. In elderly and frail residents (23% infection fatality rate nationally), it is imperative that focus remains on effective strategies for infection prevention. The tolerance and efficacy of COVID-19 vaccination among residents of LTCFs, often with numerous and serious underlying health conditions, are unknown at this time and should not represent a substitute for robust and proven preventative measures.
Pursuing public and private healthcare organization partnerships with our region's long-term care facilities may well provide an additional element of professional medical support that could benefit LTCF residents by reducing serious morbidity and death from COVID-19.
• Long-term care facilities (LTCFs) that optimize Coronavirus disease 2019 (COVID-19) preparedness lessen the risk of infection transmission and outbreaks.
• Successful infection prevention is dependent on adequate facility staffing, professional medical support, adherence to infection and engineering controls and availability of testing.
• In-house presence of a physician (medical director) and an advanced practice provider (APP), namely a Nurse Practitioner or Physician Assistant, at least one day a week, may be essential in preventing COVID-19 outbreaks in long-term care facilities thereby minimizing disease exposure and death among the elderly and infirm.
On behalf of all authors, the corresponding author states that there is no conflict of interest.
This material is the result of work supported with resources and the use of facilities at the Mann-Grandstaff Veterans Affairs Medical Center, Spokane, Washington, USA. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. We would like to acknowledge the staff and leadership of the long-term care facilities that reached out to our consultation team. The pandemic has been extremely challenging for administrators and caregivers of the nation's elderly and infirm and we have been constantly impressed by their level of dedication and commitment to elder care. We also would like to specifically recognize Stephen D. Fischer for his invaluable assistance in proofreading this submission.