The SARS-CoV-2 pandemic has placed a considerable strain on public health services worldwide. According to the Johns Hopkins COVID-19 Dashboard (https://coronavirus.jhu.edu/map.html), as of April 2021 over 150 million cases had been recorded worldwide with a global death toll of over 3 million. Most efforts in delineating the effects of SARS-CoV-2 infection have focused largely on the pulmonary, digestive and nephrological organ involvement as well as thromboembolic complications.
There is however growing evidence that there may be significant nervous system involvement in the context of SARS-CoV-2 infection [1].
Generally, the geriatric population has been disproportionately affected by the SARS-CoV-2 infection and the protean manifestations of COVID-19-related disease. The full extent of the potential sequelae of COVID-19 disease is yet to be known.
In this case presentation, we report of an elderly patient with SARS-CoV-2 infection with neuropsychiatric disorders. We present clinical, laboratory, imaging, neuropsychiatric test findings and electrophysiological evidence to underscore the potential of the neuropsychiatric burden of COVID-19 in the geriatric population.
In May 2020, a 76-year-old patient was brought to the Emergency Department of our hospital after her husband had alerted the Emergency Medical Services (EMS) of her deteriorating health. On arrival at the patient's home, the Emergency Physician noted altered consciousness (GCS 3/15) as well as dyspnea and stretch synergisms. The patient's husband reported that she had suffered at least one episode of syncope. On-site cardiomonitoring showed bradycardia that subsequently degenerated into Pulsless Electric Activity (PEA). A Cardiopulmonary Resuscitation (CPR) was successfully administered (Return of Spontaneous Circulation, ROSC 2 minutes). She was subsequently sedated, intubated and mechanically ventilated and required vasopressor support due to cardiorespiratory collapse.
On arrival at the Emergency department a diagnostic procedure was performed.
Laboratory findings showed marked leukocytosis (30.50 n/l; normal range: 3.9-10.5) as well as lymphopenia (13.1%; 20-44%), C-reactive protein level of 12.6 mg/dl (< 5), creatinine 1.11 mg/dl (0.50-0.90) (eGFR 48 ml/min/1.72 m2; > 90) and high D-Dimere levels (> 20 mg/l; < 0.5); there were also elevated levels for LDH (1370 U/L; 135-250), troponin-T (413 ng/l; < 14), Ferritin (8201 μg/l; 130-150), IL-6 (486 ng/l; < 7) and NT-pro-BNP (15.321 ng/l; < 526). All other relevant laboratory parameters including procalcitonin, creatinine kinase and CK-MB remained within normal limits. However, blood gas analysis (BGA) was notable for severe acidosis (pH 7.133; 7.35-7.45), as well as a pCO2 of 50.3 mmHg, a base deficit of -11 mmol/l and an elevated lactate level (71 mg/l; 5-20 mg/dl). An empiric antibiotic therapy with tazobactam/piperacillin for suspected incipient sepsis was initiated. A 12-lead ECG showed sinus tachycardia with no evidence of an acute myocardial infarction. An echocardiographic study showed a normal left ventricular ejection fraction and no evidence of wall motion abnormalities or relevant valvular abnormalities.
A Computed Tomographic (CT) scan of the brain showed no acute pathologies. A CT scan of the chest and abdomen with contrast material (Figure 1) showed pulmonary infiltrates in the dorsobasal aspects as well as bilateral ground-glass opacities and consolidations, features that were suggestive of COVID-19 pneumonia [2].
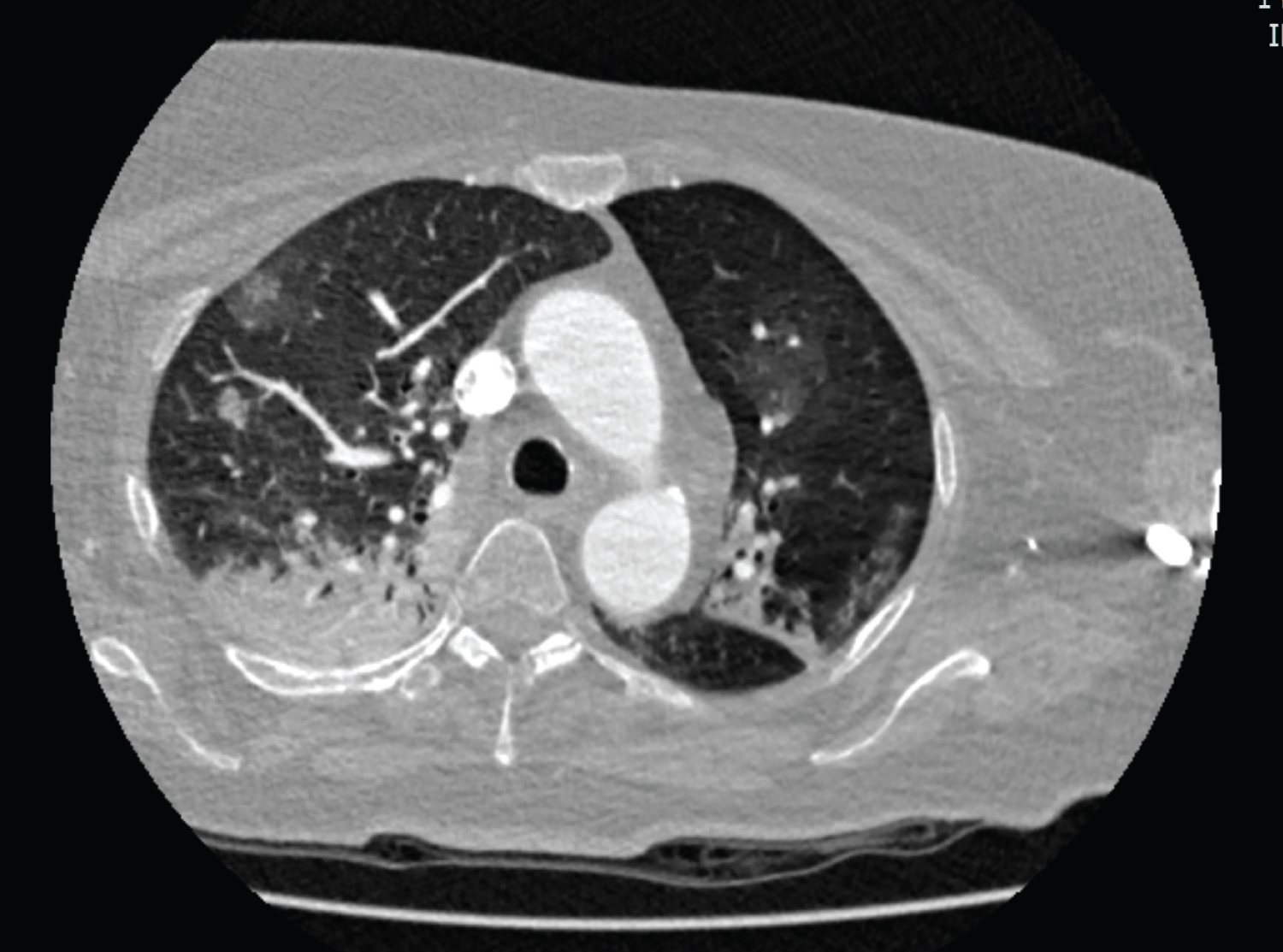 Figure 1: CT scan of the patient's chest showing pulmonary infiltrates in the dorsobasal aspects 72 as well as bilateral ground-glass opacities and consolidations, features that were suggestive of 73 COVID-19 pneumonia.
View Figure 1
Figure 1: CT scan of the patient's chest showing pulmonary infiltrates in the dorsobasal aspects 72 as well as bilateral ground-glass opacities and consolidations, features that were suggestive of 73 COVID-19 pneumonia.
View Figure 1
There was no evidence of pulmonary embolism, trauma or abdominal infection. While undergoing the imaging diagnostic procedure, she again experienced cardiorespiratory arrest and was successfully resuscitated (ROSC 2 minutes) and required continuous vasopressor support. A reverse transcriptase PCR (RT-PCR) test for the SARS-CoV-2 virus from nasopharyngeal samples returned positive.
She was subsequently transferred to the intensive care unit (ICU) for further treatment. On arrival on the ICU she was sedated (Richmond Agitation Scale -2, indicating light sedation), intubated and mechanically ventilated with the blood gas analyses showing an impaired gas exchange with global respiratory insufficiency. On examination her pupils were isocor and reactive to light. On the third hospital day, she was extubated and weaned off mechanical ventilation.
She was placed on continuous positive airway pressure (CPAP) received oxygen therapy via High Flow Nasal Cannula (HFNC) intermittently. In the clinical examination she was awake and responsive but displayed signs of deilirium that required medication with risperidone. Laboraotory studies here then revealed high levels for C-reactive protein (105.5 mg/l; < 5), procalcitonin 99.49 μg/l (< 0.5), interleukin-6 (486.4 ng/l; < 7), NT-pro BNP (12.845 ng/l; < 526), Ferritin (4086.2 μg/l; 130-150) and creatinine (4.35 mg/dl; 0.5-0.9), eGFR < 15; > 90).
Diuretic therapy with furosemide and haemodialysis were initiated after consultation with a nephrologist.
Meanwhile blood and urine cultures remained sterile. The antibiotic therapy was discontinued on the 8th hospital day following improvement in the patient's clinical condition, laboratory and vital parameters. Subsequent RT-PCR tests for SARS-CoV-2 from nasopharyngeal samples returned negative.
After further stabilization, she was transferred to the geriatric department of our hospital for further treatment and rehabilitation. She still required 4 litres of oxygen administered through nasal cannula. On examination, she displayed psychomotor sluggishness and was unable to sit or stand, let alone walk alone. The remainder of the physical examination was otherwise unremarkable.
Neuropsychological studies then disclosed findings that were suggestive of cognitive impairment (Mini Mental State 23/30, with 30 depicting the highest score attainable on the cognitive scale). Further tests using the The Consortium to Establish a Registry for Alzheimer's Disease (CERAD) test battery showed deficiencies in mental flexibility, processing speed and memory. A neurological examination performed by a trained neurologist was notable for her reduced reflexes and strength in the lower extremities as well as pallhypaesthesia of the malleolar joints. She showed hyporeflexia of the Achilles tendon, especially on the right side. She also displayed truncal instability and was unable to stand or walk on her own.
Dialysis was still ongoing. Pulmonary function tests were inconclusive because the patient was physically weak and mentally impaired to follow instructions. However, the patient had no shortness of breath and the oxygen saturation levels were satisfactory while she was breathing ambient air.
In our dedicated virology laboratory, neither SARS-CoV-2 viral loads nor antibodies were detected in the Cerebrospinal Fluid (CSF). In addition, analysis of the Cerebrospinal Fluid (CSF) showed no evidence of a co-infection with Borrelia burgdorferi, varizella zoster or herpes simplex virus. Furthermore, antibodies against SARS-CoV-2 were not detected in the CSF. However, in indirect immunofluorescence studies, high levels of IgG binding to intracellular structures (among others ANA) were detected.
Despite intensive physiotherapy, no significant improvement was initially observed in the ambulation or functional independence in our patient (Barthel index 15/100). Hence further diagnostic work-up was performed to rule out possible nervous system involvement. An MRI scan of the brain showed hippocampal atrophy, reduced brain volume, findings that are otherwise consistent with Alzheimer's disease. There was no clear evidence of spinal cord injury on MRI studies.
Electrophysiological studies then showed changes consistent with polyneuropathy analogous to critical illness polyneuropathy (CIP) (see Figure 2).
 Figure 2: Findings of the nerve conduction studies showed no stimulus response of the right pe132 roneal nerve (motoric nerve; on the left) and right sural nerve (sensory nerve); on the right) des133 pite maximal stimulation. Fibrillating potentials and positive sharp waves in the tibial anterior 134 muscle were also noted, findings that are consistent with Critical Illness Polyneuropathy (CIP).
View Figure 2
Figure 2: Findings of the nerve conduction studies showed no stimulus response of the right pe132 roneal nerve (motoric nerve; on the left) and right sural nerve (sensory nerve); on the right) des133 pite maximal stimulation. Fibrillating potentials and positive sharp waves in the tibial anterior 134 muscle were also noted, findings that are consistent with Critical Illness Polyneuropathy (CIP).
View Figure 2
In the meantime, the initially abnormal laboratory findings returned largely to within normal values. The electrolyte levels, HbA1C, folic acid and vitamin B12 were within normal limits. She was successfully weaned off dialysis. Following intensive physical therapy and respiratory training, her functional independence improved somewhat (Barthel index 35/100). There were no longer any signs of delirium and risperidone was discontinued; she however still showed signs of cognitive impairment in repeat neuropsychological testings, with deficits in verbal and figurative memory. She was transitioned to a phase B rehabilitation centre for further treatment and care.
Severe SARS-CoV-2 infections typically tend to manifest in the respiratory system, causing acute respiratory distress syndrome (ARDS) requiring intensive care potentially leading to multiorgan failure. The present case, however, seeks to corroborate growing evidence suggesting severe neuropsychiatric involvement in the setting of the COVID-19 disease. In summary, our patient was diagnosed with acute SARS-CoV-2 infection which initially involved the cardiopulmonary system, although - against the backdrop of the syncope she experienced - neurologic involvement might well have been present from the onset especially given the stretch synergism that was present. The course was further complicated by multi organ failure, the need for intubation and mechanical intubation due to respiratory failure and dialysis for acute renal failure accompanied metabolic derangement. Before hospitalization, the patient had been otherwise healthy and functionally independent with a medical history of well-controlled asthma and hypertension.
Strikingly, although she was intubated and mechanically ventilated for only 3 days, she showed clinical signs of polyneuropathy which were subsequently confirmed by electrophysiogical studies which demonstrated features consistent with critical illness polyneuropathy, even though the timeframe of severe illness in this patient was rather too short to make this diagnosis [3]. In this context, the absence of clinical evidence and imaging correlates of severe or permanent damage in the central and peripheral nervous system appears to argue against the presence of substantial brain or nerve damage consequent upon CPR.
Neurophysiological assessments showed mild cognitive impairment and subclinical delirium with MRI brain scans revealing features consistent with (chronic) neurodegenerative changes. Considering the age of the patient, it would be safe to assume that these changes pre-existed the onset of acute illness brought on by SARS-CoV-2 infection. Analyses of the cerebrospinal fluid failed to detect SARS-CoV-2 pathogens and antibodies, which is in line with recently published literature [4]. However, in indirect immunofluorescence studies of CSF high levels of IgG binding towards intracellular structures (among others ANA) were documented, suggestive of autoreactivity, a feature which has been recently described in COVID-19 patients with neurological manifestations even in the absence of SARS-CoV-2 in the CSF [5]. Crucially, there was no evidence of a co-infection by other neurotropic viruses.
Although there is growing evidence of an association of SARS-CoV-2 infection with neurologic pathologies, it remains unclear if the SARS-CoV-2 infection was the culprit or an innocent bystander in relation to the neuropsychiatric changes seen in this patient, although such a hypothesis would appear cogent in the light of our findings. Indeed, recent data from autopsy and other reports suggest that SARS-CoV-2 infections are associated with neuropathy as well as changes in mentation in affected individuals [6].
Following 3 weeks of intensive physical and cognitive therapy in the geriatric department, we noted improvements in her functional abilities at the time of transfer. She regained truncal stability and was able to sit on her own; she could also walk using a walking frame under the guidance of a physiotherapist and it was possible to converse with her adequately. As of February, 2021 following discharge back home from rehabilitation, she was doing well and could ambulate independently using a walking frame and her cognition had improved. She however complained of tremors of the hands.
The findings presented here strongly suggest a neurological involvement in the setting of SARS-CoV-2 infection in this otherwise previously healthy patient. This hypothesis was largely substantiated by the clinical observations, electrophysiolgical and laboratory and CSF studies. A deranged cellular immune response that mimics the Guillain-Barre syndrome has been proposed as a likely mechanism for the neurologic pathologies seen in COVID-19 infection [7].
The transient nature of her recovery and the absence of substantial neuropsychiatric sequelae argue against significant hypoxic brain damage, tipping the scales towards direct potential CNS damage by an autoimmune response. Interestingly, detection of the SARS-CoV-2 viral antigen or antibodies directed against it - as seen in this case - do not appear to be preconditions for neurologic involvement.
The disturbed mentation was ascribed to pre-existing (latent) underlying mild cognitive impairment (MCI) which was accentuated by the SARS-CoV-2 infection.
With this investigation, we wish to draw attention to the genuine probability of neuropsychiatric involvement in the context of SARS-CoV-2 infection. In the light of this and other clinical observations published elsewhere, it is easy to envisage a situation where elderly frail patients also present with neuropsychiatric symptoms. Physicians and caregivers should accordingly raise their suspicion index for neurological and mental health issues in geriatric patients with ongoing or antecedent SARS-CoV-2 infection. This would help in early diagnosis and the institution of adequate therapy (in this case intensive physical and cognitive therapies).
This case also highlights the importance of a multidisciplinary approach (in this case medical, laboratory, neurocognitive and physical therapy expertise) in the management of the fall-out from SARS-CoV-2 infection with a view to ameliorating the public health burden associated with this novel human virus. This report also throws a searchlight on the potential manifold manifestations of SARS-CoV-2 infection as we await further clinical, laboratory and epidemiological findings in the efforts to fully understand this novel disease entity.
We thank Dr. Victor Max Corman for the virological studies and Prof. Rajan Somasundaram for reviewing the initial draft.
Michael Nnaji coordinated the post-Covid care of the patient, was involved in the conception of the report and wrote the manuscript; Adrian Rosada conceived the report and provided crucial consultation in the patient's care and in the writing of the report; Skadi Wilke performed the neuropsychological assessment and provided cognitive training to the patient in the vignette; Isabelle Wirsching was involved in the neurological care of the patient and contributed to the manuscript; Johannes Schurig was involved in the neurological care of the patient and wrote the neurological part of the report; Harald Prüss performed the immunological studies; Christiana Franke provided crucial neurological expertise in clinical and data interpretation as well as making inputs to the manuscript; Wolfgang Bauerled the initial treatment of the patient in the Emergency Department and contributed to the manuscript; Ursula Müller-Werdan was involved in the conception of the report and provided crucial material and other support.