Background: The global trend towards an increasing aging population demands for adequate geriatric medical care services to cater for health needs of the aging population seeking clinical care in hospitals. In Uganda, geriatric care as a specialty in medicine is still at infancy stage, and this is further worsened by the fact that the current curricula followed in training health workers lacks a component dedicated to elderly care. There is therefore need to assess knowledge, attitudes and treatment practices of medical doctors towards clinical care for elderly persons.
Objective: We aimed to assess knowledge, attitudes and treatment practices of medical doctors towards care for elderly persons accessing clinical care services at hospitals in Kampala.
Methods: We conducted a cross sectional descriptive study between April and June 2019 at outpatient's clinics, inpatients wards and non-communicable disease clinics at selected hospitals in Kampala Capital City Authority Uganda. All medical doctors providing direct clinical care to elderly persons at the selected hospitals and meeting the inclusion criteria were selected using a multi stage clusters ampling method. Those who consented were interviewed using a pre-tested semi structured questionnaire. The Knowledge about Older Persons-Q (KOP-Q) scale and the Older People in Acute Care Survey-United States (OPACS-US) scale were utilized, and responses measured on a Likert scale coded and entered into Microsoft Excel 2010, cleaned and then exported to STATA 13 for analysis. A generalized linear model was used with the family of Poisson and log link with robust standard error to provide prevalence ratio as a measure of association with corresponding 95% confidence intervals and p-values. Ethical clearance was obtained from the respective hospital Institutional Review Boards, Higher Degrees Research and Ethics Committee at Makerere University School of Public Health, and Uganda National Council of Science and Technology.
Results: Among the 110 respondents, 73 (66.4%) medical doctors had suboptimal knowledge on clinical care of elderly patients, majority of medical doctors demonstrated a positive attitude towards care of elderly persons and over three-quarters 82 (74.5%) of medical doctors did not routinely observe recommended treatment practices when caring for elderly patients. Factors found to be significantly associated with knowledge on clinical care of elderly persons were level of education of medical doctors and frequency of refresher trainings on geriatric care. Similarly, level of education of medical doctors and hospital affiliation were significantly associated with treatment practices when caring for elderly patients.
Conclusions: Majority of medical doctors had suboptimal knowledge on geriatric care, with a majority failing to follow routine recommended treatment practices when caring for elderly patients.
Recommendations: Therefore, the higher education division of Ministry of Education should enforce integration of geriatric care in training curricula for medical schools. Also, guidelines on geriatric clinical care and treatment practices should be drafted and made more accessible to medical doctors at the hospitals.
Knowledge, Attitudes, Treatment practices, Medical doctors, Elderly care
Globally the number of elderly persons is growing faster than the number of persons in the younger age group, and it is expected that between 2017 and 2050, virtually every country in the world will experience a substantial increase in the population size of persons aged over 60 years. This number of elderly persons is projected to reach nearly 2.1 billion by 2050 [1].
In Africa, the population of elderly person's is most likely to account for 4.5% of the continent's population by 2030, and almost 10% by 2050. Sub-Saharan Africa currently accommodates about 46 million elderly persons (5% of the population) and this is expected to increase four-fold by 2050 [2].
Uganda faces the same trend of an ever-increasing elderly person's population. According to the 2002 Uganda population census, the population of elderly persons increased from 686,260 (4.1%) of the total population of 16.6 million in 1991 to 1.1 million (4.6%) of the total population of 23.9 million in 2002 [3]. Current UBOS statistics estimate a total number of persons aged over 60 years to be 1.43 million persons (4.8% of the population) and it's expected to rise further to a projected 10.5 million elderly persons come 2030 [4]. This population increase directly impacts on health delivery systems especially in terms of human resources to cater for increased healthcare needs for elderly persons seeking healthcare [5].
Increased health care needs amongst elderly persons is as a result of retrograde biological growth process accompanied by a decline in physical functions, increased susceptibility to diseases and an altered response to medications compared to younger persons. Elderly persons therefore tend to frequent health facilities more than younger adults, with an estimated 11.4 average hospital visits a year for elderly persons aged over 60 years compared to younger persons [6].
Frequent hospital visits by elderly persons therefore requires medical doctors to be equipped with appropriate competences and skills to fulfill significant roles in responding to the current and future health needs of the elderly population. Although the above situation (health workers with adequate knowledge, attitudes and skills to care for older persons) is desirable, it is far from the reality on ground as a majority of health workers are not fully equipped with appropriate competencies and skills to cater for elderly persons in clinical care, but more worryingly health workers trained in health institutions with no defined curriculum on geriatric medicine and hence limited knowledge and treatment practices when caring for elderly persons.
Previous studies done in the past by Topaz and Doran; Dacey, et al. [7,8] have all revealed insufficient knowledge on elderly person's clinical care amongst health workers. Also, studies carried out since the 1950s have identified negative attitudes of health care workers toward the hospitalized elderly persons or those seeking health care services at the health facilities. Those attitudes have prevailed into the 1990s and highlight the low status associated with working with elderly patients [9]. Research also showed that the quality of health care services provided by health workers to elderly persons is strongly influenced by their knowledge and attitudes towards elderly people [10]. Furthermore, knowledge of ageing and attitude towards the elderly are important in promoting good clinical care practices in the healthcare delivery systems [11].
Even though the above studies have provided some information on clinical care of elderly persons by health professionals, a majority of these studies have either not solely focused on medical doctors, or have been done in countries with a different health care system compared to the Ugandan health care system. There is therefore need to assess knowledge, attitudes and treatment practices of medical doctors towards clinical care for elderly persons. Results from this study will help provide basic information for designing structures and programs for the care of elderly persons in the health facilities as well as drafting of training curriculum designs on geriatric care to be used in the training of health professionals both in training institutions and during in- services training programs.
A descriptive cross-sectional study was conducted between April and June 2019 among medical doctors who provide clinical health care to elderly persons in the outpatient's clinics, inpatients wards and special disease clinics at selected hospitals in Kampala Capital City Authority Uganda.
A multi-stage cluster sampling method was employed to select hospitals, facility departments (OPD, medicine wards, surgery wards, special clinic departments) and medical doctors (respondents) for the study. The hospital departments were purposively selected and medical doctors in each of the selected departments were randomly selected for the interview. Sampling was done at 3 stages. In Stage one, we did listing and description of hospitals located in Kampala. The number of hospitals in both public (governmental) and private (nongovernmental or for profit) hospitals within Kampala were identified. In stage two, we did stratification of listed hospitals into government hospital, specialized hospital, private not for profit and private hospital. From each stratum, simple random sampling was done to choose a minimum of two hospitals. The chosen hospitals within each stratum were then utilized as study units. In stage three we did purposive sampling to select hospital departments and, in each department, sampled, lists of all medical officers (respondents) were used as sampling frames. Using the sampling frame from the selected departments, probability proportionate to size was employed to obtain number of medical doctors sampled from each hospital sampled. At the chosen hospitals, simple random sampling was applied to select the respondents for the study.
All coded data from questionnaires were double entered into Epi Data 2010, it was then cleaned for errors and exported to Stata Version 15 for statistical analysis.
Univariate analysis was used to summarize categorical variables into proportions and frequencies. Cross tabulations were done for knowledge and treatment practice as dependent variables, for each of the individual and hospital factors. Cells that had less than five counts were not included in bivariate and multivariate analysis using regression. A generalized linear model (glm) was used with the family of Poisson and a log link with robust standard error for bivariate and multivariate analysis of knowledge and practice since the prevalence of knowledge (37%) and practice (28%) were greater than 10% [12]. Un-adjusted prevalence ratios (UPR) for knowledge and practice with their 95% confidence intervals and p-values with a statistical significance of 0.05 were presented to measure the association between each individual and health facility factor (independent variables). Independent factors from bivariate analysis that had a p-value less than 0.05 qualified for multivariate analysis. Stepwise elimination method was used to add and drop independent factors. Independent factors were tested for collinearity to ensure they were not strongly related to each other. Adjusted prevalence ratio (a PR) with their 95% confidence intervals and p-values with a statistical significance of 0.05 were presented to measure the association between individual and hospital factors with knowledge and practice as dependent variables. Responses for positive and negative attitudes were presented as a Likert scale in table form.
Ethical approval to carry out the study was sought from from the respective hospital Institutional Review Boards, Higher Degrees Research and Ethics Committee at Makerere University School of Public Health and Uganda National Council of Science and Technology. Written informed consent was obtained from all participants before participating in the study.
Of the 125 medical doctors working in selected hospitals within Kampala, total of 110 medical doctors participated in the study giving a response rate of 88%. A majority of the participants were male (n = 61, 55.5%), with a majority (n = 51, 46.4%) in the age range of 20-29 years. Eighty (72.7%) participants had received undergraduate training only based on education achievement attained so far and a minority (n = 10, 9.1%) had received an additional medical fellowship specialty training. Majority of medical Doctors 39 (35.45%) trained at Makerere university medical school, and 5 (4.6%) in foreign medical schools. Only respondents trained in foreign medical schools 5 (4.6%) reported to have had a curriculum on geriatric medicine while the rest of the respondents who had their medical training in Ugandan medical schools reported that they did not have a curriculum on geriatric medicine at undergraduate level and postgraduate schools. Regarding medical working experience, a majority (n = 66, 60%) had a 1-3 year working experience, about half of the respondents (n = 55, 50%) were working in government hospitals and a minority (n = 14, 12.7%) in specialized hospitals (Cancer and Heart institute). All hospitals sampled had an active refresher training program being held on varied schedules depending on the hospital, majority hospitals visited (n = 108, 98%) did not have special geriatric wards, no geriatric guidelines at the hospitals, no geriatric specialists and no geriatric nurses available at hospital. By professional cadre, 44 (40%) were medical officers, 37 (33.6%) were junior house officers, 18 (16.4%) were Special grade medical officers and 11 (10%) were senior house officers. A majority of the respondents (n = 88, 80%) did not have any training on geriatric care. Table 1 and Table 2 summarize the sociodemographic characteristics of the participants.
Table 1: Baseline characteristics of study patients. View Table 1
Table 2: Hospital factors. View Table 2
For analysis purpose, knowledge was measured using average number of correct responses and categorized into two; good knowledge (> 20) and average knowledge (< 20) [13]. Thirty-three percent (n = 37) of the participants scored 20 or more in the knowledge questionnaire and were considered to have good knowledge, the remaining majority (n = 73, 66.4%) scored less than 20 and were considered to have average knowledge (Figure 1). Factors found to be significantly associated with knowledge on geriatric care were advanced educational level (post-graduate and fellowship) a PR: 1.51; 95% CI: 1.31-1.75; p = 0.001, a PR: 1.42; 95% CI: 1.17-1.71; p = 0.001 and refresher training on geriatrics a PR: 1.24; 95% CI: 1.07-1.45; p= 0.005 (Table 3).
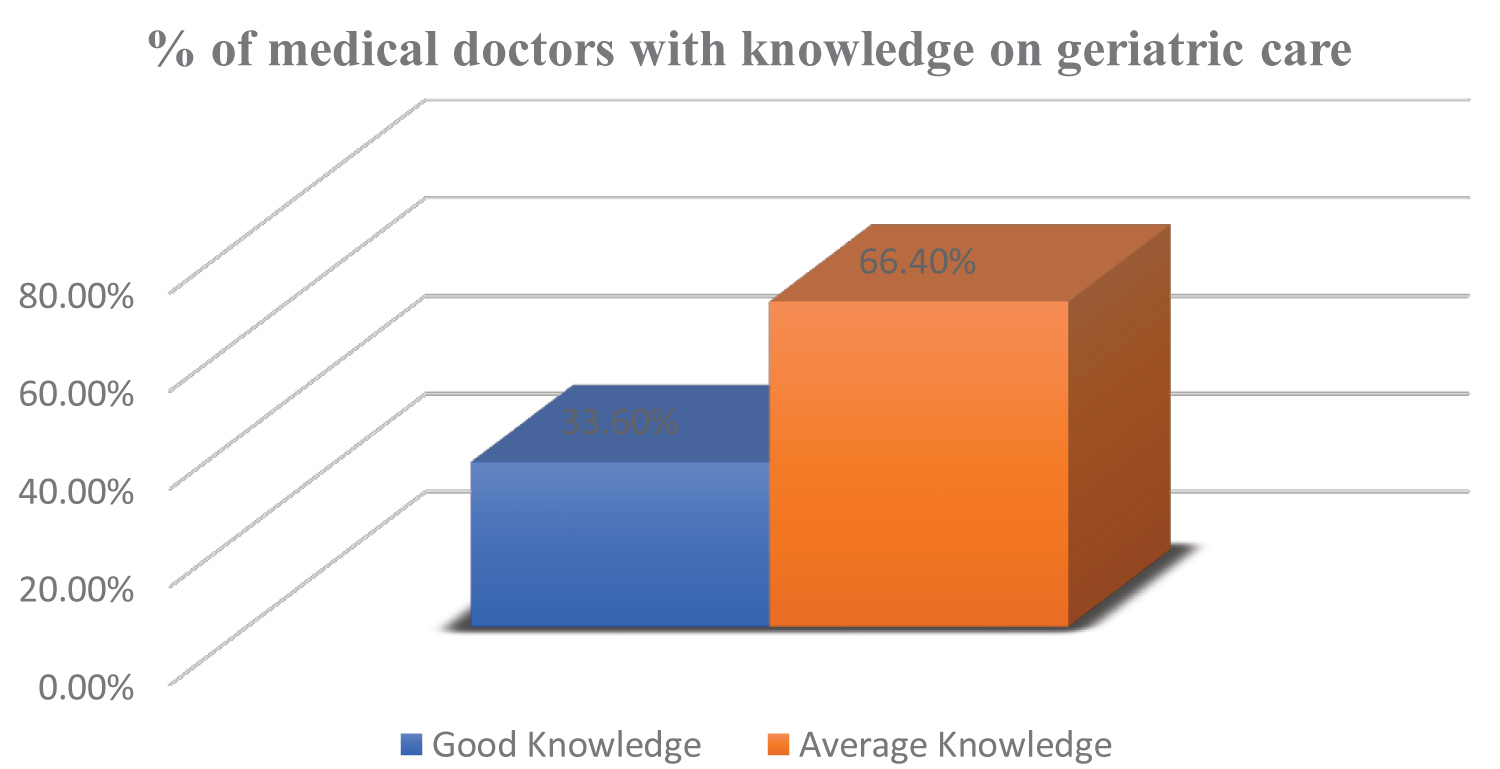 Figure 1: Knowledge of participants on geriatric care.
View Figure 1
Figure 1: Knowledge of participants on geriatric care.
View Figure 1
Table 3: Factors associated with knowledge on geriatric care. View Table 3
Majority of the study participants (n = 76, 69%) had a positive attitude regarding care of elderly patients, most of the responses using the Likert scale were on "agree" as per the positive opinion being explored. About 40 (36.4%) had a negative attitude regarding care of elderly patients. Their responses using the Likert scale on negative attitudes were on "agree" as per the negative opinion being ±score was 106.0 ± 4.68 with the range of 34-170 (Table 4 and Figure 2).
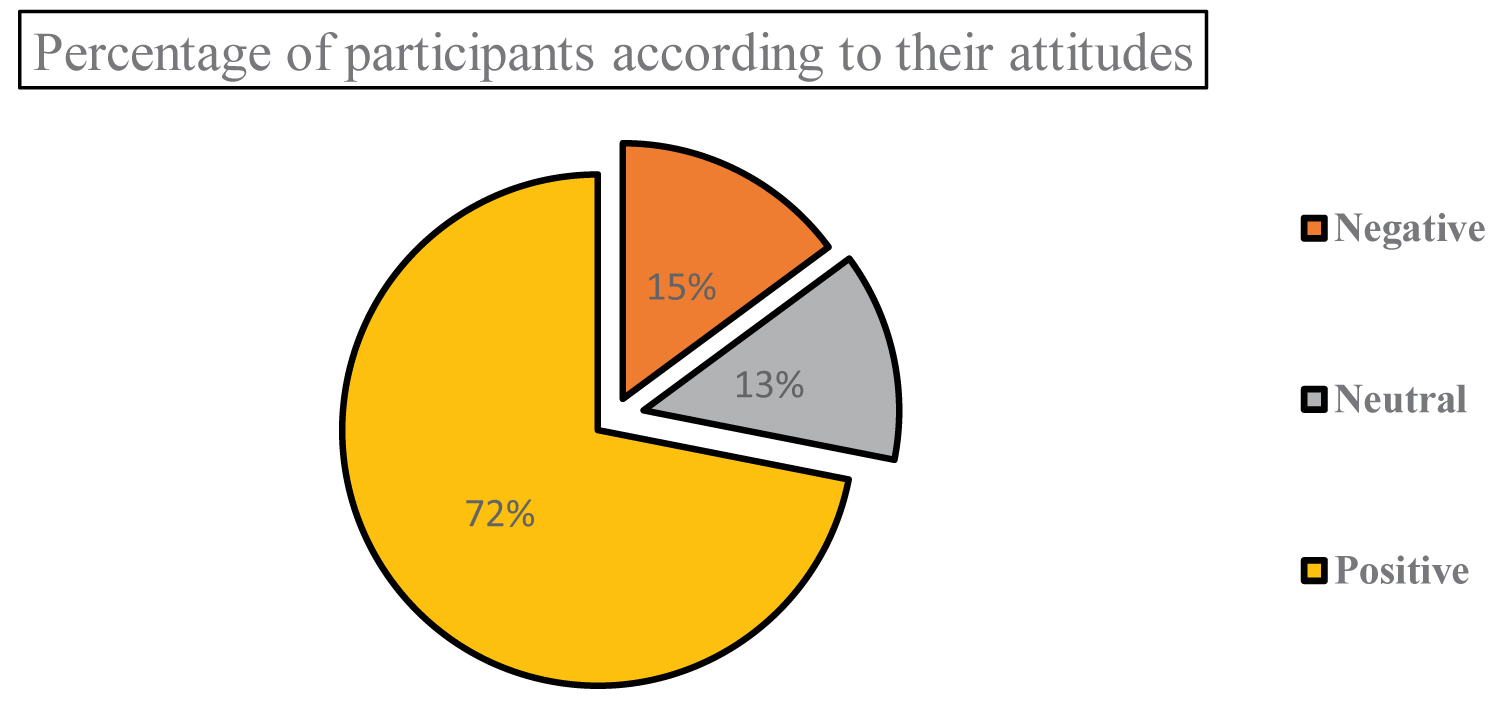 Figure 2: Percentage of participants according to their attitudes level.
View Figure 2
Figure 2: Percentage of participants according to their attitudes level.
View Figure 2
Table 4: Mean score and categorization of attitude score regarding elderly care (Max attainable score: 170). View Table 4
Study participants were asked a set of questions on treatment practices when caring for elderly patients. All participants who responded "Always" were considered to be routinely observing recommended treatment practices when interfacing with geriatric patients while those who responded "Sometimes" were considered not to be routinely observing treatment practices when interfacing with the geriatric patients. Majority of the study participants (n = 82, 74.5%) did not routinely observe treatment practices when caring for elderly patients. 71 (64.6%) did not routinely obtain a comprehensive health history from older patients and a majority 104 (94.6%) were not using a health assessment tool specifically designed for assessing older patients. Only a third (n = 33, 30%) routinely offered more time when interacting with elderly patients. Overall, three quarters (n = 82, 74.5%) of the study participants did not routinely observe treatment practices while one quarter (n = 28, 25.5%) routinely observed treatment practices when caring for elderly persons (Figure 3). Factors found to be significantly associated with treatment practices of medical doctors when caring for elderly persons were advanced educational level (aPR: 1.31; 95% CI: (1.17-1.44; p = 0.001, aPR: 1.32; 95%CI: (1.07-1.61; p = 0.001 and hospital affiliation in a specialized hospital (aPR: 1.19; 95% CI: (1.05-1.35; p = 0.05 Table 5).
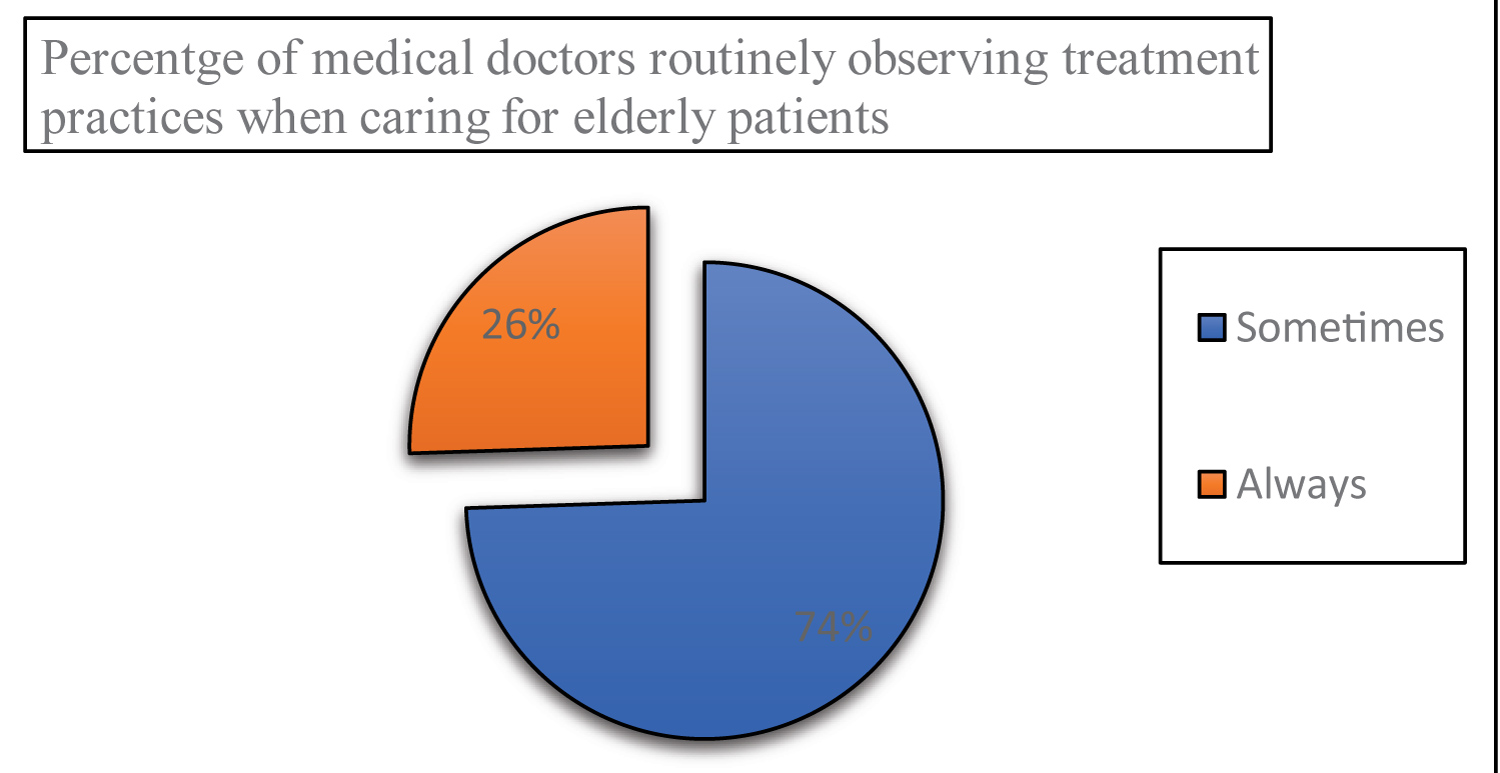 Figure 3: Percentage of medical doctors routinely observing treatment practices.
View Figure 3
Figure 3: Percentage of medical doctors routinely observing treatment practices.
View Figure 3
Table 5: Factors associated with treatment practices when caring for elderly patients. View Table 5
Geriatric medicine as a specialty is still in an infancy stage in Uganda, and yet medical doctors are at the forefront in offering clinical care to the rapidly increasing elderly population. It is therefore of paramount importance that medical doctors have appropriate knowledge, attitude and treatment practices when caring for elderly persons accessing clinical care services at the hospitals.
To the best of our knowledge, this is the first study in Uganda to assess the KAPs of medical doctors towards clinical care of elderly patients. There are also very limited studies that document KAPs among medical doctors globally. In the present study we were able to demonstrate that medical doctors in general had sub-optimal knowledge on clinical care of elderly persons, which findings are similar with findings by Dacey, et al. [8], where about two thirds of physician assistants had low knowledge on geriatric care. These findings are possibly due to absence of teaching modules on geriatric care in the undergraduate and postgraduate training curricular of medical doctors as documented by Donatelle [14], and Alsenany [15] that poor knowledge on ageing amongst healthcare providers is attributed to absence of modules on geriatric care during their training. Also, few refresher trainings on geriatric care, with no specific extensive courses undertaken in geriatrics education by medical doctors contributed to deficiency in knowledge on geriatric care. The findings were similar to those in a study by Kaempfer, et al. [16] that showed low knowledge amongst health care workers because no refresher training courses related to geriatrics had been undertaken.
Medical doctors demonstrated a positive attitude when caring for elderly persons. This was attributed to their level of education, as documented by evidence from Nelson [17] which showed that graduate health workers were more likely to develop positive attitudes towards elderly persons under their care than nongraduate health workers.
An earlier study by Kaempfer, et al. [16] reported that the higher the level of education of health workers, the more positive their attitude towards care of elderly people under their care. Also, a study by Doherty, et al. [18] measuring health worker's attitudes towards elderly people reported a significant association between having a university graduate education and positive attitudes towards care of elderly people.
Similarly, positive attitudes are strongly influenced by cultural, social and life experiences of living with elderly persons outside the school context, which act as strong foundations to developing positive perceptions towards elderly people. Medical doctors could have been driven by socialization components related to culture, personal values and family upbringing, and therefore regarded care of elderly persons as an obligation inculcated into them through cultural and social upbringing. Findings are in line with Callaghan, et al. [19] who reported that attitudes are influenced by many factors primarily related to socialization components such as culture, personal values and religious belief. In the same vein, Andrews, et al. [20] points out that a person's attitudes are greatly influenced by cultural values, norms and social structure of community.
In contrast to the study findings, it should be pointed out that a positive attitude towards elderly persons may not necessarily translate into superior care since positive and negative feelings can coexist [21]. This contradiction is evident in study findings that revealed gaps in treatment practices of medical doctors when caring for older persons in spite of positive attitudes displayed by medical doctors.
Majority medical doctors did not routinely follow recommended treatment practices when caring for elderly peoples in clinical care. Suboptimal treatment practices demonstrated could partly be attributed to the inadequate knowledge exhibited by medical doctors on geriatric care.
Findings are similar to studies by Adibelli and Kilic [22] and Deguzman, et al. [23], where insufficient general geriatric knowledge was a barrier to optimal treatment practices when caring for elderly people. Similar findings of insufficient knowledge on geriatric care having an impact on clinical treatment practices when caring for elderly people have been reported in high income countries by Bleinjenberg [24] and Lambrinou, et al. [25].
Absence of guidelines on geriatric care in the hospitals could partly explain the suboptimal treatment practices demonstrated when caring for elderly people, as documented by Grimshaw, et al. [26], Lomas, et al. [27]. The findings are similar to a study conducted in the USA and Netherlands by Grol and Grimshaw [28] that reported about 30-40% of patients did not receiving care according to recommended evidence because either treatment guidelines were not being used or were absent in the health care institutions.
Level of education (postgraduate), refresher training on geriatric care and working in specialized hospitals were significantly associated with knowledge and treatment practices of medical doctors on geriatric care. This finding could be due to improvement in knowledge and treatment practice that comes with advancement in training or more years of education, work experience and as such, more exposure to geriatric education and interaction with elderly peoples in clinical care as documented by Alsenany [15]. The findings are similar to studies done by Bleijenberg, et al. [24] and Lambrinou, et al. [25] that reported that senior colleagues in medical practice had better knowledge and skills than junior colleagues in medical practice. Also, findings in the study are in line with Donahue, et al. [29], where geriatric education enhanced knowledge and attitudes of health workers towards care for elderly people.
On the contrary, Eltantawy [30] reported no significant association between exposure to geriatric training modules and knowledge of care for elderly people.
Our study has limitations. Firstly, only medical doctors working in selected Kampala hospitals were surveyed and the results of this study may not reflect the KAPs of medical doctors in the entire country. However, this is the first study to assess KAPs, it can be used to formulate targeted Continuing Medical Education (CME) on geriatrics for medical doctors and enrolled in a countrywide survey and training on geriatric care. Secondly, a small sample size of consultant doctors in the study prevented the analysis of knowledge and treatment practices of this cadre of doctors and as a result, they had to be collapsed with the cadre of medical officer special grade doctors. Also, the number of respondents who had their medical training in foreign universities was minimal and as such it was not possible to determine whether they had better knowledge and treatment practices on geriatric care. In view of the above two limitations, the concepts from this study may not be generalizable to consultants' doctors and doctors trained in foreign universities, who work in other hospitals within the country, and this limits the survey's generalization.
In conclusion, we found that more than two-third of medical doctors working at hospitals in Kampala had suboptimal knowledge about geriatric clinical care. Knowledge about geriatric clinical care was significantly higher among medical doctors with postgraduate training and had received refresher training on geriatric clinical care. Majority of the medical doctors had a positive attitude towards care for elderly people, their opinions on geriatric care indicated that they were willing to offer clinical care to elderly people as well as work within the context of elderly people. Over two thirds of medical doctors did not routinely follow recommended treatment practices when caring for elderly persons in clinical care.
In light of these study findings, we recommended that the higher education division of Ministry of Education should consider drafting and integrating geriatric care modules in the general curricula of medical schools both at undergraduate and postgraduate levels. This will empower medical trainees with the required competences, and help improve the knowledge and treatment practices of medical doctors churned out of medical training schools in Uganda. Also, hospitals should adopt the WHO guidelines on geriatric care and place them at accessible points for medical doctors to always refer to when caring for elderly people as well as consider creating special services for elderly people in the hospitals. This can be in form of special wards, clinics and triage systems for geriatric.
We acknowledge the supervisor's Dr Sebastian Olikira, Dr. Stephen Kabwama for their commitment and unreserved efforts made when reviewing this work; Dr. Patricia Ntege, Dr. Dorah Nakayiwa and Dr. Jemimah Nambooze for reviewing and analyzing this work.