The population of elderly in the world is continuously increasing. According to the National Institute of Health dated March 2016, approximately 8.5 percent of people worldwide (617 million) (ages 65-years-old and older) and this percentage would advance to nearly 17 percent of the world's population by 2050 (1.6 billion) [1,2].
According to the United Nations, World Population Prospects: The 1998 revision: Volume I, [3] majority of the aging population are found in the developing countries roughly 248 million of the 418 million (59 percent) people (65-years-old and older). Asia, with the greatest number of elderly people at around 217 million [3].
Philippines, being a developing country situated at the Southeastern part of Asia, number 2 in the most populous country among south eastern countries with 109,581,078 (as of October 2020 based on the latest United Nation estimates), has at least 4.6 million senior citizens (60 years and older) representing about 6 percent of the total population. By the end of 2025, an expected elderly population will be 10.25 percent [4,5].
Having this in mind, the inferences of this growing population could be greatly influenced by the lifestyle, socioeconomic and nutritional aspects that could predict the increasing trend our beloved elderlies. It is important to note that the implications of these growing population are a result of cultivating appropriate strategies based on the quality of life, social stability, and health apprehensions [6,7].
What are the factors that affects the longevity and quality of life among community- dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
The study will serve as scientific evidence that will be useful for health professionals, organizations, and policy maker - providing services to the older persons and those working in geriatrics. It may also help in design management and treatment strategies that will contribute in life expectancy of the geriatric population.
Tondo Medical Center is an institution that aims to have its own Geriatric Medicine unit as part of its mission to serve and provide quality health care among the growing population of elderly in Northern Metro Manila.
General objectives: 1. To determine the factors associated with longevity among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
Specific objectives: 1. To determine the clinicodemographic profile among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
a. Age
b. Gender
c. Body Mass Index
d. Presence of comorbidities
2. To determine the lifestyle factors that affect the longevity among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
a) Leisure activities
i. Physical
ii. Intellectual
iii. Social
iv. Recreational
b) Smoking
c) Alcohol Consumption
3. To determine the socioeconomic factors that affect the longevity among community- dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
a. Living status
b. Occupation
c. Educational attainment
4. To determine the nutritional status using the mini nutritional assessment-short and cognitive screening among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
a. Mini Nutritional Assessment
b. Cognitive function
linic demographic profile: Refers to the general information of patients that include their age and gender.
Longevity: Also referred to as life expectancy; is one of the commonly used terms in aging research that may be defined as an individual's ability to reach longer life span.
Community-dwelling elderly: People are defined by their age (≥ 60 years of age) and by living independently. This group can suffer from a large variety of health care problems; from just getting older (not diseases specific) to suffering from multiple pathologies.
Rural: A geographic area that is located outside towns and cities.
Seniors: Any individual at the age of 60 and above.
Nutritional status: Defined as an individual's health condition as it is influenced by the intake and utilization of nutrients.
Functional status: Is an individual's ability to perform normal daily activities required to meet basic needs, fulfill usual roles, and maintain health and well-being.
Activities of daily living: Everyday routines generally involving functional mobility and personal care, such as bathing, dressing, toileting, and meal preparation. An inability to perform these renders one dependent on others, resulting in a self-care deficit.
Mental Status: A comprehensive or statement of patient's intellectual capacity emotional state and general mental health based on examiners observations and directed interview.
New normal: Refers to the emerging behaviors, situations, and minimum public health standards that will be institutionalized in common or routine practices and remain even after the pandemic while the disease is not totally eradicated through means such as widespread immunization. These include actions that will become second nature to the general public as well as policies such as bans on large gatherings that will continue to remain in force.
COVID-19 inter-agency task force on Emerging Infectious Disease (IATF): Is a task force organized by the executive of the Philippine government to respond to affairs concerning emerging infectious diseases in the Philippines.
Social distancing: The practice of maintaining a safe or appropriate physical distance from other people, or the measures taken to reduce close physical.
Aging is an inevitable process that every individual will go through. As the saying goes "aging is not lost youth but a new stage of opportunity and strength", therefore the maintenance of functional aptitude which empowers wellbeing in older adults is an active and heathy aging [8].
Philippines being a developed country has its own growing statistics of elderly population. According to the 2015 Census population, [4] approximately 7.5% of our total populations were senior citizens ages 60-years-old and over. Amongst the regions in the Philippines, rural area contributes largest to its component. The top five regions with the highest number of senior citizens were Region IV-A (13.3%), followed by Region III (11.6%), NCR (11.3%), Region IV (9.4%), and Region VII (8.2%). Out of the 5 regions, only one belongs to the urban area [5]. The rural areas still managed to dominate, even noted to have a less accessible community, with a probable low cost of living, provided with a fewer highly specialized institution catering their utmost needs.
Among the living population of our country, female senior citizens dominated the study which encompasses 58.8% (3.33M) compared to males with 44.2% (4.22 M) [5]. The life expectancy of our country, may be credited with the combining efforts of the local government to eliminate communicable diseases where our senior citizens were vulnerable. The family support, resilience and optimistic attitude of every Filipinos backs up on reaching their retirement stage.
Life expectancy among Filipinos in 2018 is 69.3 years, according to the latest data published in 2018 by the World Health Association [6]. It is referred to as the average number of years that members of a population live. An assessment of different factors that contributes to the longevity of Filipinos living in a rural area may be compared to those residing in urbanized zones (Figure 1).
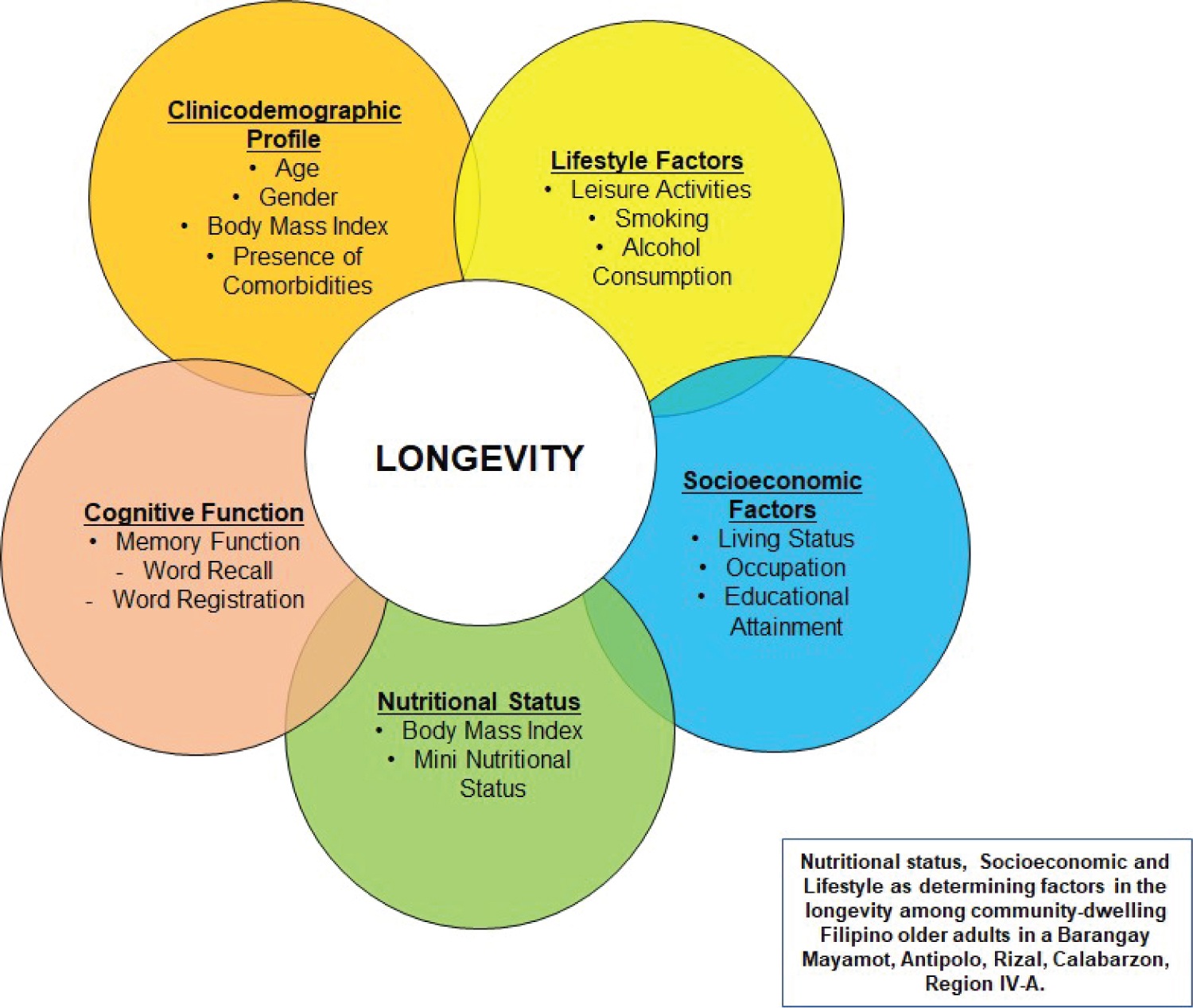 Figure 1: Conceptual framework based on Swedish study.
View Figure 1
Figure 1: Conceptual framework based on Swedish study.
View Figure 1
The framework of the study is primarily based on the study by Rizzuto, Orsini, Qiu and Wang in 2012, a population-based cohort study conducted in Kungholsmen, Stockholm, Sweden [9].
As define by the study of Ferreira, et al., in 2018, entitled Evaluation of Lifestyle and quality of life in the elderly: A literature review, "lifestyle is characterized as a set of habits, choices and customs experienced by individuals throughout life". Habits include smoking, alcohol beverage drinking and physical exercise [10].
Elderly is more vulnerable to malnutrition, since their nutritional requirements are not well established, especially those with multiple comorbidities. A decline in the lean body mass and basal metabolic rate accompanies aging process. Nutritional status greatly affects the elderly as it may contribute to the different diseases they developed [11]. In the program of World Health Organization, named Ageing and Health, some recommendations were cited regarding factors that affects aging and nutrition, and one of these are dietary intake and nutrition absorption in older person. In one of the studies done in Europe, entitled "Survey in Europe on Nutrition and the Elderly: A Concerted Action (SENECA), 2006, dietary intake of elderly people was sufficient but tended to decline overtime, this is caused by the decrease capacity of the body to synthesize and absorb nutrients" [12].
A questionnaire was developed for geriatric patients in Switzerland, named The Mini Nutritional Assessment (MNA) form, it was designed and validated that provides rapid assessment of nutritional assessment in elderly [13]. This was used in a local study done by the Department of Nutrition, College of Public Health, University of Philippines Manila entitled "Use of Mini Nutritional Assessment as Nutritional Screening Tool, among Urban Older Adults in Pasay City, Philippines". in which they identify who are nutritionally at risk among urban elderlies [14].
Cognitive impairment is an important determinant of clinical outcomes. It is vital in the assessment of geriatric population to provide better management. A 3-minute Mini-Cog instrument will assess cognitive impairment in older adults [13]. The strategic instrument can be used effectively by a health care provider and in community settings, however it does not substitute for a complete diagnostic workup. Other than this, a mini-cog instrument form is provided with different languages that are easily understood by the participants.
The research examined the factors that affect the longevity among community-dwelling Filipino older adults based on their structured self-assessment questionnaire. This is to determine the nutritional, the socioeconomic, and the lifestyle factors that could serve as indicators that affects longevity and active aging among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A. Every Tuesday and Thursday of the month, approximately four to six senior citizens ages 60 to 64-years-old were catered in the rural health unit. Considering the Inter-Agency Task Force protocol, any persons below 15-years-old, over 65-years-old, and pregnant women shall be required to remain to their residences except when indispensable under the circumstances for obtaining essential goods and services, or for work in industries and offices or such other activities permitted in this section, Resolution No. 79 (October 15, 2020) [15].
In observance of the COVID-19 Inter-Agency Task Force on Emerging Infectious Diseases (IATF) Resolution No. 88 (December 14, 2020) [15], health protocols were observed and followed strictly for the duration of the research study. Including social distancing, proper wearing of face masks and face shields, proper disinfection, and proper disposal of used materials.
An approximately 28 meters by 15 meters open area (half basketball court), outside the rural health unit is provided. It is an open and well-ventilated area covered by tent. Half of this is allotted for the survey area, and the other half will act as a waiting area for the respondents. The number of people that can be accommodated in the survey area following the social distancing protocol is 10 (8 of which are respondents, 1 rural health unit nurse, and the principal investigator), while approximately 8 to 10 respondents will be at the waiting area (with proper social distancing).
A screening area outside the barangay health unit is provided. Before proceeding to the triage, respondents were screened. If the respondent has one of the exclusion criteria, they will not proceed to the next step. But they will have a separate check-up to address any health concerns, as referred by the Principal Investigator to the rural health medical officer. If the respondents meet the inclusion criteria, they can proceed to the next step. These respondents underwent triage by two (2) barangay health workers. First, foot bath. Second, sanitation process (hand hygiene necessities and checking of proper wearing of face mask and face shield). And last, checking of vital signs (blood pressure, heart rate, temperature, respiratory rate, body weight in kilograms, and height in centimeters). The following apparatus were provided and used - one (1) blood pressure monitor, one (1) infrared forehead thermal scanner, one (1) stethoscope, two (2) tape measures, one (1) weighing scale, one (1) pulse oximeter, and one (1) UV sterilizing box. After use, adequate sanitation was applied using sanitation materials such as alcohol and alcohol wipes. In case of incomplete protective gears, the Principal Investigator provided free necessary materials.
After completing the triage protocol, the respondents were seated at four (2) long tables measuring 2.5 meters, which can accommodate 2 participants each (with chair provided), observing social distancing of 1 to 1.5 meters. As well as a pair of pencil and pen for each respondent.
Consent form was provided for each respondent. The Principal Investigator explained the mechanics of the survey. Participants were guided and assisted by the principal investigator as they accomplish each form. There will be three questionnaires, namely – 3 min Mini-cog form, clinicodemographic profile form, and mini nutritional form.
The first questionnaire, 3 min Mini-cog form was performed by the Principal Investigator and the rural health unit nurse who was properly oriented regarding the procedure. It includes three domains which include cognitive, language, visuospatial and executive function. First is the three-word registration, the facilitators asked the respondent to listen carefully as they mention three words that they need to remember and recite back to the facilitators. Second is the clock drawing, where a pre-printed circle (on a paper) was given to the respondent, then the facilitator asked the respondent to draw a clock. They were asked to write the numbers and set the clock to specific time (within three 3 minutes). Lastly, is the three-word recall. Here, the facilitators asked the respondents to repeat back the three words they recited in the first domain (three-word registration). In case, the respondents were evaluated to have decreased cognitive function, they will be referred to a more detailed evaluation of their cognitive status to determine necessary management.
The second questionnaire is the clinicodemographic form. It is a checklist of the clinicodemographic profile of the respondent which includes educational attainment, previous occupation, recreational activities, living status, health status, and smoking/drinking history. For the health status, it is an evaluation of any underlying comorbidities and chronic medical conditions. The Principal Investigator extracts history of common medical conditions associated with aging. It also includes the review of their medications that they are taking currently. In case of finding out that the respondent has an underlying condition, they were referred to the rural health unit medical officer for proper evaluation and management in accordance with the severity of the disease at the end of the survey.
The third questionnaire is the Mini-nutritional Status Assessment Form. It is a screening tool in evaluating the nutritional status of the respondent. This is to determine if the respondent is at risk of malnutrition. The Principal Investigator guides the respondent in answering the questions. In case of finding out that the respondent has an underlying malnutrition status, they are referred to the rural health unit medical officer for proper evaluation and management.
Used face mask and sanitation kits are disposed properly in a yellow bag. Before exiting the premises, a sanitation area is provided. Each respondent receives a sanitation kit, and a snack, as a token of appreciation for participating in the study (Figure 2, Figure 3A and Figure 3B).
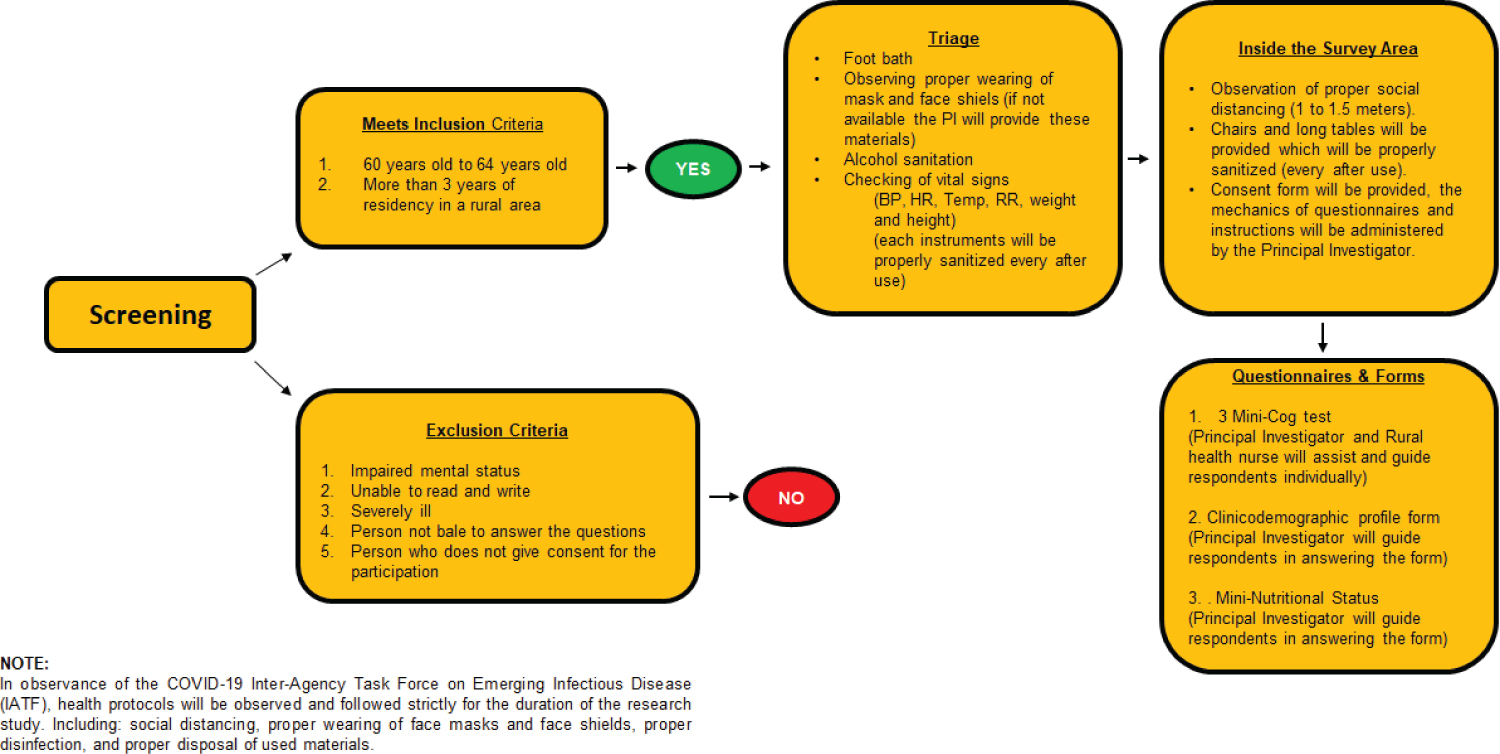 Figure 2: Flowchart of the screening and survey process.
View Figure 2
Figure 2: Flowchart of the screening and survey process.
View Figure 2
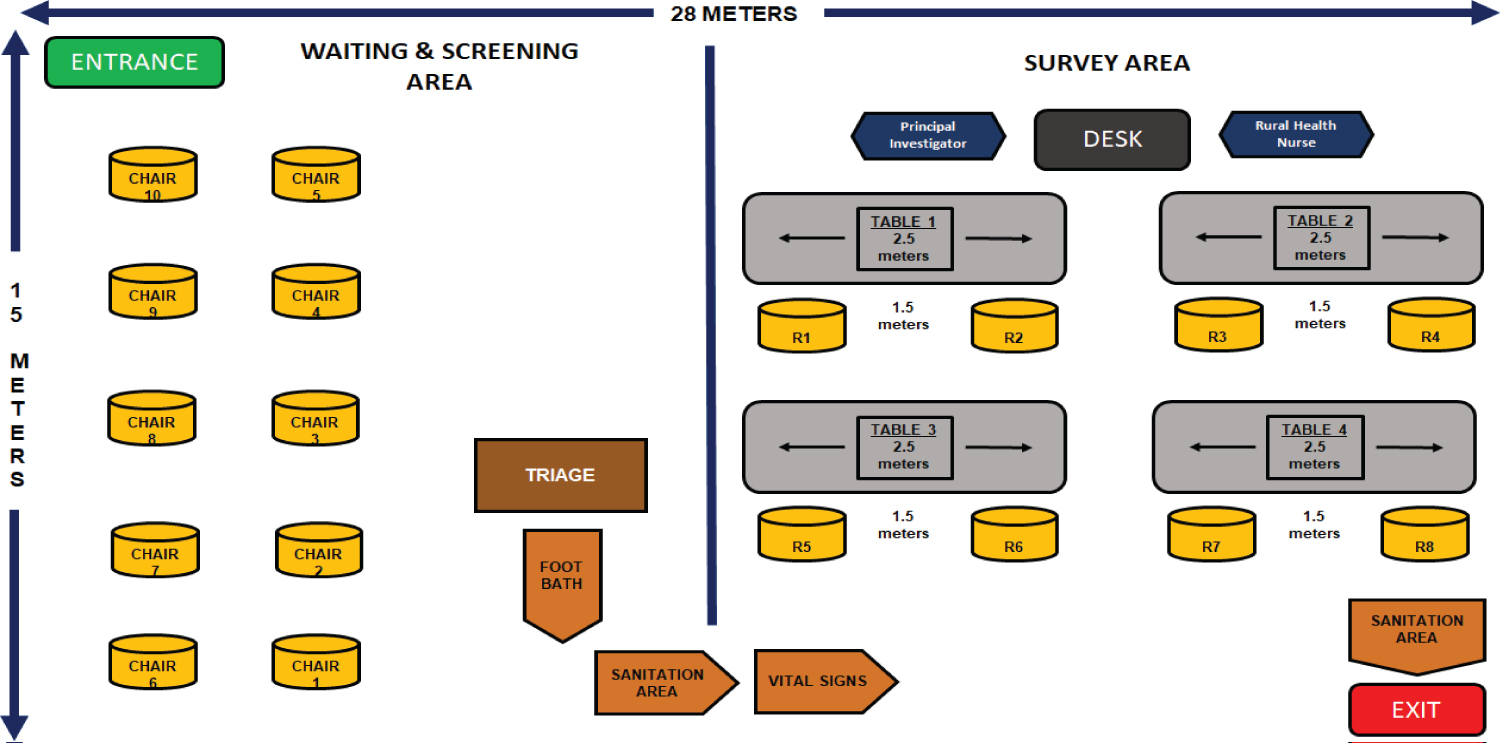 Figure 3A: Ideal Floor plan of the reserved area for the research study.
View Figure 3a
Figure 3A: Ideal Floor plan of the reserved area for the research study.
View Figure 3a
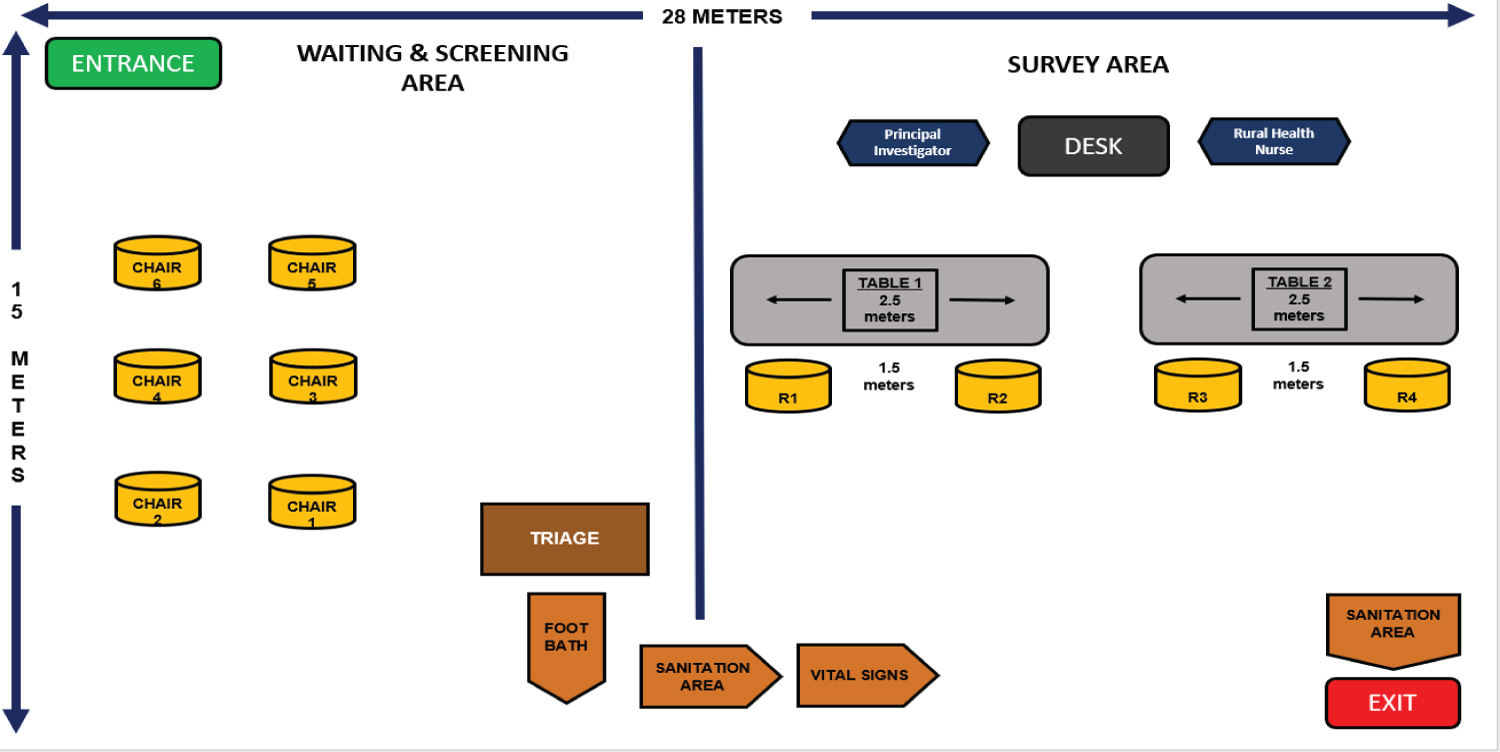 Figure 3B: Actual Floor plan of the reserved area for the research study.
View Figure 3b
Figure 3B: Actual Floor plan of the reserved area for the research study.
View Figure 3b
The research is a prospective study that examines the factors that affects the longevity among community-dwelling Filipino older adults based on their structured self-assessment questionnaire, to determine nutritional, socioeconomic, and lifestyle factors.
Demographic characteristics are reported as frequencies and proportions based on mean age stratification, sex (female and male), lifestyle, nutritional, and socioeconomic factors.
The study is conducted from January 2021 to April 2021, in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A. It is a rural health unit in Calabarzon Area, Region IV-A, serving the 3 barangays in Antipolo, namely Barangay Mayamot, Barangay Cupang and Barangay Mambugan, in which according to the Philippine Statistics office 2015 Census has the largest population size in Region IV-A area [16]. A consent form was handed over to rural health unit officer, explaining the purpose of the research study in their community.
As per the rural health unit officer a list of senior citizens is provided. In this list, demographic profile is included, where the qualified respondents were determined, as guided by the inclusion and exclusion criteria of the study.
1. 60-years-old to 64-years-old
2. More than 3 years of residency in a rural area
1. Severely ill
2. Impaired mental status/presence of cognitive impairment
3. Unable to read and write
4. Person not able to answer the question
5. Person who does not give consent for the participation
Different types of data were collected from the participants of the study, namely:
• Personal Characteristics
• Employment Information
• Mental Activities
• Physical Activities
• Social Activities
• Productive Activities
• Social Networks
• Smoking and Alcohol Consumption
• Chronic Medical Conditions and Comorbidity
A checklist of most common medical conditions and comorbidities were provided in the questionnaire.
Participants were guided in answering chronic medical conditions. Medical history, vital signs, and maintenance medications were asked by the principal investigator in order to evaluate if there are presence of comorbidities.
A checklist provided by the rural health unit, indicating the most common maintenance medications they prescribe to each participants are reviewed.
Health status:
Check if any is applicable (may mga sakit na sumusuod)
o Hypertension
o Diabetes Melitus
o Heart Disease
o Chronic Kidney Disease
o Arthritis
o Lung Disease
o Others:____________
Evaluation of the health status includes probing in the history and medications used by the participants. In order to be objective, the criteria for each comorbidity are evaluated. According to the Eighth Joint National Committee (JNC8) published the evidence-based guidelines in diagnosing hypertension in adults. A systolic blood pressure of 140-159 mmHg and a diastolic pressure of 90-99 mmHg is classified as Hypertension Stage I, while a Systolic blood pressure of > 160 mmHg and a diastolic BP of > 100 mmHg is a diagnosis of Stage II hypertension. First line medications with hypertension includes ACE inhibitor and blockers (e.g. Enalapril, lisinopril), ACE blockers (e.g. Losartan, telmisartan), Calcium channel blockers (e.g. Amlodipine, felodipine) and beta blockers (eg metoprolol, carvedilol). On the other hand, diabetes mellitus is one of the leading comorbidities among elderly, is define as having the following ADA (American Diabetes Association) criteria; FPG ≥ 126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 h or 2-h PG ≥ 200 mg/dL (11.1 mmol/L) during OGTT. The test should be performed as described by the WHO, using a glucose load containing the equivalent of 75g anhydrous glucose dissolved in water or A1C ≥ 6.5% (48 mmol/mol) or in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥ 200 mg/dL (11.1 mmol/L). First line medications for diabetes mellitus includes Biguanides (e.g., Metformin), sulfonylureas (e.g., Gliclazide, glimepiride), SGLT 2 inhibitor (e.g., Empagliflozin, dapagliflozin), DPP4 inhibitor (linagliptin, sitagliptin) and insulin. Other comorbidities such as coronary artery diseases, stroke, arthritis, cardiovascular pulmonary disease and renal diseases were evaluated accordingly.
Nutritional status: Mini nutritional assessment form is a clinical tool to help identify elderly persons who are malnourished or at risk of malnutrition [14].
Mini nutritional status examination has a standardize questionnaire form, each participant was assisted by the principal investigator as they go along with the questions. Body mass index is a big part of this form in which a weighing scale and tape measure measuring calf circumference was used, if BMI is not available as specified in the questionnaire form.
Screening measures were provided below: Decline in Food intake is measured with questions "Has the food intake declined over the past 3 months due to loss of appetite, digestive problems, chewing or swallowing difficulties?" response options were 0 = Severe decrease food intake, 1 = Moderate decrease in food intake, 2 = No decrease in food intake.
Weight loss during the last three months. Response options were 0 = weight loss greater than 3 kg (6.6 lbs), 1 = Does not know, 2 = Weight loss between 1 and 3 kg (2.2 and 6 lbs).
Mobility. Response 0 = Bed or chair bound, 1 = Able to get out of bed/chair but does not go out, 2 = Goes out.
Psychological stress. "has suffered psychological stress or acute disease in the past 3 months?". Response 0 = Yes, 2 = No.
Neuropsychological problems. Response 0 = Severe dementia or depression, 1 = Mild dementia, 2 = No psychological problems.
Body mass index. Response 0 = BMI less than 19, 1 = BMI 19 to less than 21, 2 = BMI 21 to less than 23, 3 = BMI 23 or greater.
Screening score (maximum of 14 points). 12-14 Normal nutritional status, 8-11 points at risk of malnutrition, 0-7 points malnourished.
A Mini-Cog is a composite of three item recall and clock drawing, developed as a screening test for cognitive function in a community sample of culturally, linguistically, and educationally heterogenous older adults [13].
Three domains include three-word registration, clock drawing and three- word recall, with the following interpretation and scoring:
Word recall. 0-3 points, 1 point for each word spontaneously recalled without cueing.
Clock draw: 0 or 2 points. Normal clock = 2 points. A normal clock has all numbers placed in the correct sequence and approximately correct position (e.g., 12, 3, 6 and 9 are in anchor positions) with no missing or duplicate numbers. Hands are pointing to the 11 and 2 (11:10). Hand length is not scored. Inability or refusal to draw a clock (abnormal) = 0 points.
Total score. Total score = Word Recall score + Clock Draw score.
A cut point of < 3 on the Mini-Cog™ has been validated for dementia screening, but many individuals with clinically meaningful cognitive impairment will score higher. When greater sensitivity is desired, a cut point of < 4 is recommended as it may indicate a need for further evaluation of cognitive status.
Due to the exploratory nature of the study and time restrictions, descriptive prospective study analysis is used. A power analysis is used using the data gathered from the questionnaires. Data gathered from the interviews were compared to the national statistics and comparisons made with the Kungholsmen Project study and a local study done in an urbanized setting [9,17].
Data gathered will serve as baseline information for future research.
Sample size computation will be based on Slovins's Formula, it is computed as,
n = N/(1+Ne2)
Whereas:
n = No. of samples
N = Total population
E = Margin of error
The sampling technique that is utilized in this study is quota sampling wherein certain elements are selected from each age category. An estimate of 100 or less population of senior citizens in Barangay Mayamot are provided by the rural health unit (Figure 4).
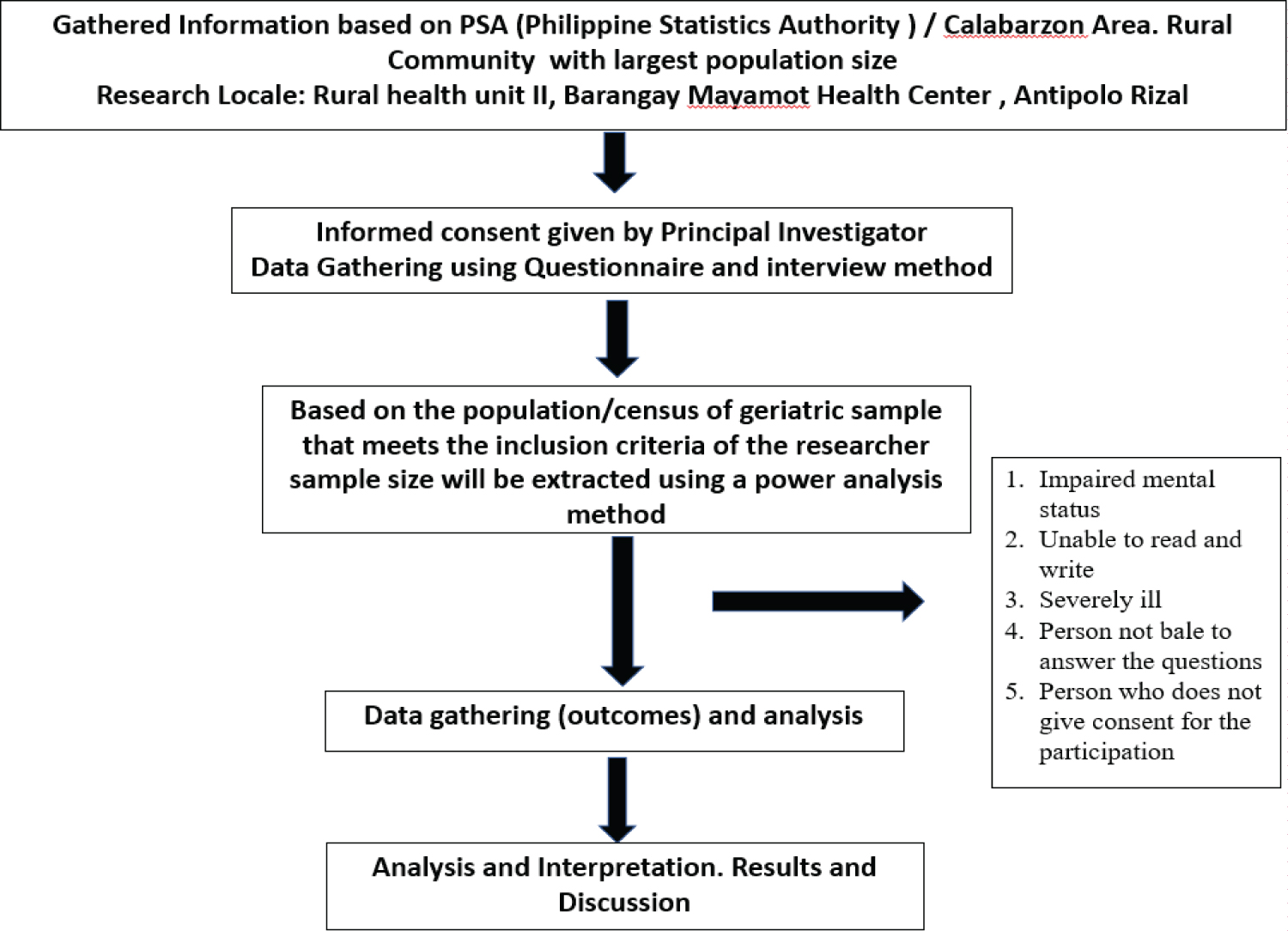 Figure 4: Framework on process of data gathering, assessment, and interpretation of results.
View Figure 4
Figure 4: Framework on process of data gathering, assessment, and interpretation of results.
View Figure 4
Participants of the study were asked to sign informed consent before the interviews were conducted. Informed consent included verbiage that allowed all data gathered from the interviews to be used for the sake of the research and that strict confidentiality was observed at all times.
All information provided during the interview remained only between the participant and the interviewer. Initials of the subjects were written on the questionnaires merely for the sake of differentiating data from one another but not in relation to the subject. A token of appreciation is given to each participant at the end of the interview (sanitation kit and snack). The study has no conflict of interest.
Due to the ongoing pandemic, the COVID-19 Inter-Agency Task Force on Emerging Infectious Diseases (IATF) has strict protocols leading to lesser number of respondents that can be accommodated, such as not allowing 65-years-old and over individuals from going out of their residences and limitations on social/mass gathering [15]. Time constraints that will result to shorter interaction with the respondents, also in addressing their other concerns. In the last quarter of the study, an unfortunate surge in cases of COVID-19 has emerged, hence a stricter protocol has been established in 2 weeks to almost a month. In line with these, the target population of 100 was reduced to 84 since senior citizens were not allowed to go out of their respective household.
The original floor plan design in this study was revised, since a number of study population has been limited in the actual set up due to the observance of social distancing in a mass gathering.
The following chapter presents primary findings of this research investigation. The presentation, interpretation and analysis of the data are based on the objectives set forth in this investigation.
Objective Number 1: To determine the clinicodemographic profile among community- dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
Table 1 depicts the clinicodemographic profile of the 84 senior group collected from Barangay Mayamot. The mean age of the population is 62.9 with a standard deviation of 1.5 ranging from 60 to 64-years-old with majority of the sample being women (77.4%). Body Mass Index (BMI) records showed that a greater number of the participants (71.4%) were of normal weight with the next most prevalent BMI classification being overweight (23.8%).
Table 1: Clinico-demographic profile of geriatric sample. View Table 1
Of the 84 elderly participants in the study 70 of them had at least one form of comorbidity, with hypertension (61) as the predominant chronic disease followed by Diabetes Mellitus (20), heart disease (10), Arthritis (13), with 14 respondents who answered they do not have any comorbidity. Comorbidity occurred in 70 participants and multimorbidity in 10 of them.
Objective Number 2: To determine the lifestyle factors that affect the longevity among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A (Figure 5).
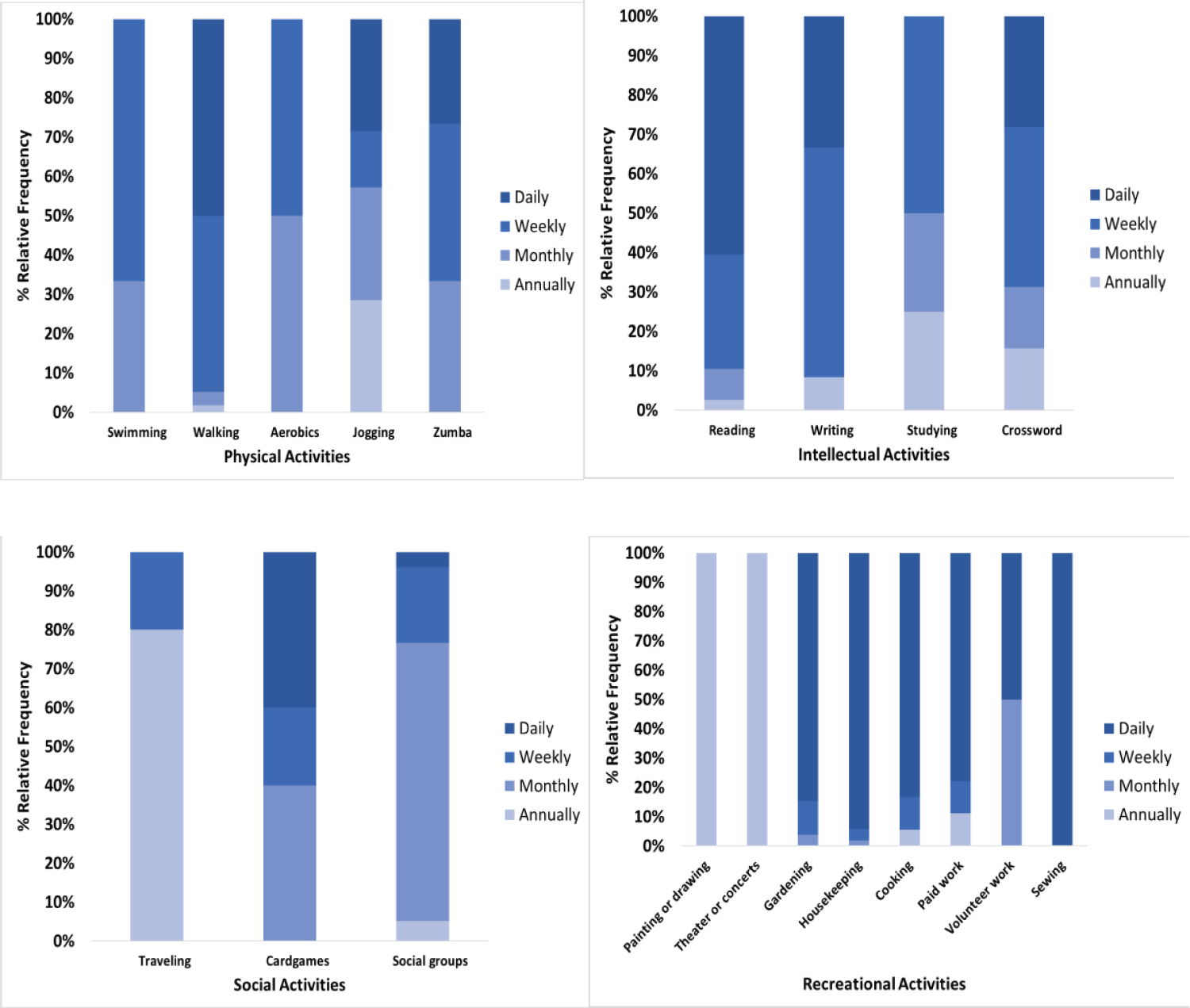 Figure 5: Shows the distribution of different physical activities, intellectual activities, social activities and recreational activities among the geriatric sample.
View Figure 5
Figure 5: Shows the distribution of different physical activities, intellectual activities, social activities and recreational activities among the geriatric sample.
View Figure 5
Table 2.1 shows the distribution of lifestyle factors previously mentioned, responses grouped according to three categories, leisure activities, Smoking and alcohol consumption. Leisure activities were further subcategorized under mental, social, physical and productive. In terms of participation, the most prevalent for seniors was productive activities with all 84 participants performing one or more activity that helped either their family's finances or day-to-day housework on a regular basis. Housekeeping, gardening and cooking were the most frequently done activities with 50 (59.5%), 22 (26.2%) and 15 (17.9%) of the seniors participating in both activities on a daily basis.
Table 2.1: Distribution of lifestyle factors among geriatric sample. View Table 2.1
The next most participated in activity was mental, with 84 (100%) the geriatric sample taking part in one or more of this type of pursuit, with the most prevalent mental activities being reading at (38/84 or 45 %) doing crossword at (32/84 or 38%). Majority of the senior group, 79 (75%) participated in some form physical activity, with walking (58%) being the most prevalent activity followed by dancing classes in the form of Zumba (15%).
Among the different categories of leisure activity, the study population was least engaged in social activities. Only 19 (18%) of the sample participated in any form of social pursuits with 8 of the subjects reporting their sole social activity as playing card games with friends.
Majority (85.7%) of the participants reported that they had never smoked. Eight (9.6%) report that they continued to smoke at the time of the study, while 4(4.8%) participants were former smokers with 1-6 pack years consumption.
Lastly for lifestyle factors, Majority (82.1%) of the senior sample did not consume alcohol in their lifetime Table 2.2.
Table 2.2: Distribution of lifestyle factors among geriatric sample. View Table 2.2
Objective Number 3: To determine the socioeconomic factors that affect the longevity among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A (Figure 6).
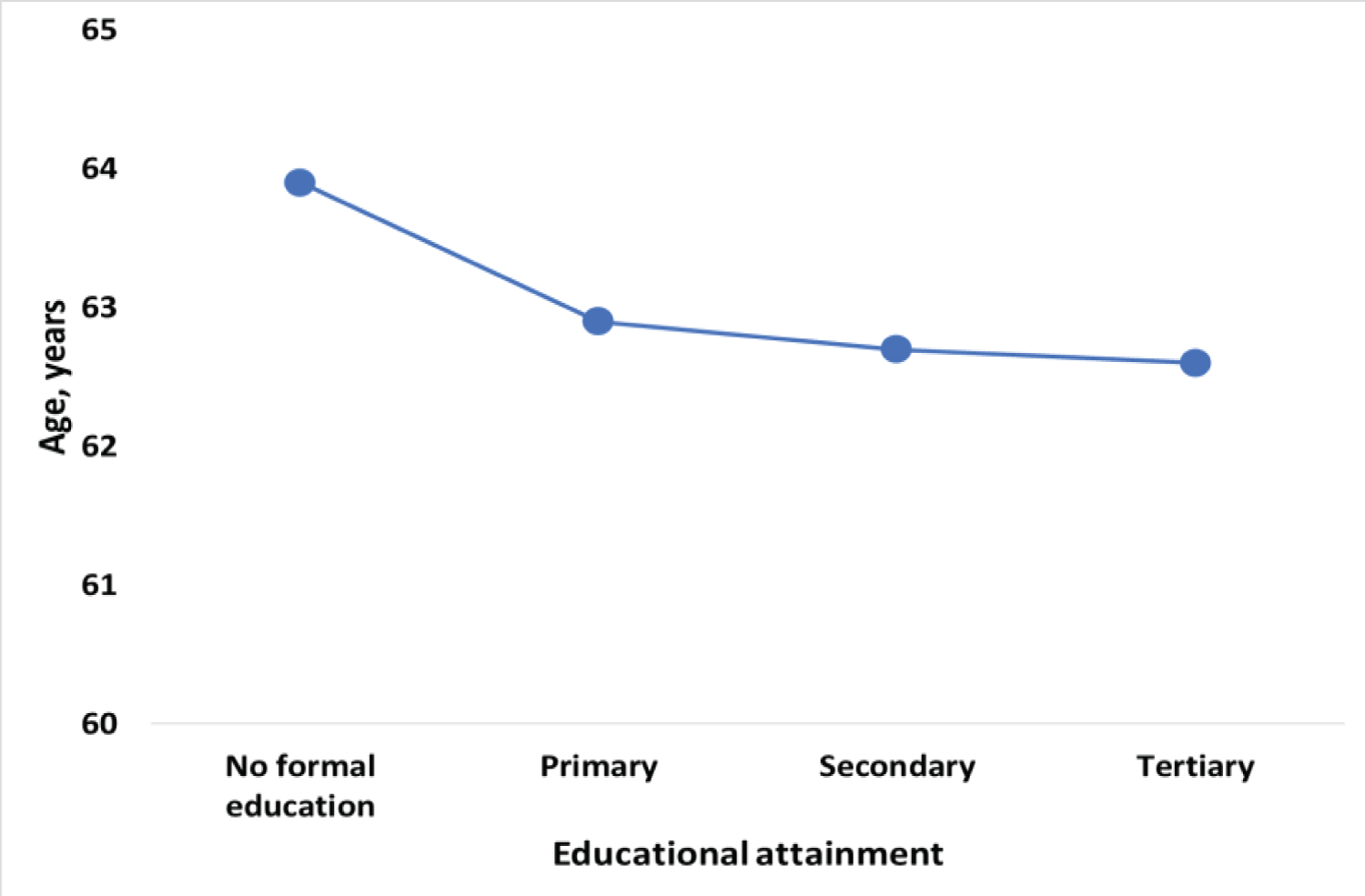 Figure 6: Shows the distribution in years of the geriatric sample related to their educational attainment.
View Figure 6
Figure 6: Shows the distribution in years of the geriatric sample related to their educational attainment.
View Figure 6
Table 3 depicts the distribution of social factors by each defined category. Social network was divided according to living status in which subcategorize into living with spouse only, living with children and both, with other relative and non-relatives. Majority 78 (92.9%) of the geriatric group had a rich social network which exhibits living in with the 1st degree relatives followed by those with moderate social network or living in with other relatives (17.9%). Only 6 of the respondents reported having a limited or poor social network which suggests that they have no longer have a spouse and that they do not have any children or if they did, they were not satisfied with their interactions.
Table 3: Distribution of social factors among the geriatric sample. View Table 3
Thirty-one (36.9%) of the 60 to 64-years-old senior population had up to primary level of education with 31 (36.9%) attained secondary education and 12 (14.3%) attained a tertiary level of education. It is important to note that unlike the studies that have been previously conducted, a new category had to be created under educational attainment, no formal education. Ten of the 84 participants did not attend any formal schooling. Tied to this finding is the type of job variable as 13 of the 10 participants who did not have any formal education also did not have any job history. The greater number of participants (57 or 67.9%) held a blue-collar position for majority of their working lives and only a minority (14 or 16.7%) had white-collar jobs.
Objective Number 4: To determine the nutritional status using the mini nutritional assessment-short and cognitive screening among community-dwelling older adults in Barangay Mayamot, Antipolo, Rizal, Calabarzon, Region IV-A.
Table 4.1 depicts the mini nutritional status assessment of the 60 to 64-years-old senior population. Seventy-six (90.5%) are not at risk of malnutrition while 7 (8.3%) are at risk. It is important to note that 1 out of 84 participants recorded as malnourished.
Table 4.1: Distribution of nutritional status among geriatric sample. View Table 4.1
Table 4.2 showed the mental status of the participants, which was also included in the inclusion criteria. All the participants passed the said category.
Table 4.2: Distribution of mental status assessment among geriatric sample. View Table 4.2
In this descriptive study of 84 senior citizen participants several data jump out as relevant when compared to other studies conducted on the oldest of the old, among them is the gender distribution, leisure activities, smoking, nutritional status, comorbidities and longevity.
Comparing with the results of the previous study done in an urbanized location there wasn't a marked difference in terms of gender distribution between the results of the study in rural (22.6% male and 77.4% female) and the urban (39.05% male and 60.95% female) with the most recent census of the PSA (44.2% male and 58.8% female). While this confirms the national life expectancy and the current body of research that women live longer than men. It should be noted that the urbanized study done by Rocamora M.D. includes people age 70 and up, however in this study only senior citizens ages 60 to 64-years-old were included in accordance with the IATF protocol, since the study was done during the pandemic.
In addition, the average life expectancy of males based on the Philippine statistics is 57.4 compared to the 63.2 of women. With the said statistics in mind, one would presume that there would be a greater gender discrepancy in the participants of study considering the baseline age of the study is 12.6 years over the general life expectancy of male seniors in the country. This suggests an improvement in the life expectancy of males, however without restrospective evidence to support it, this may only be inferred.
Lifestyle factors and longevity: Lifestyle factors gathered for the study are similar to the baseline data of the Kungholsmen Project study that the study was based on. The Swedish study found statistically significant relationships between longevity and two lifestyle factors, specifically, smoking and leisure activities.
When compared to the Urban study results done in Tondo Manila, it showed that mental and productive leisure activity are higher in the population study with almost a hundred percent participation in both activities. In this research study done in a rural set-up, 42.9% participated in the mental activities and 41.7% participated in the physical activities on a daily basis. As compared with the urban study done, (75%) of its population participated in physical activity. This could be explained by the strict safety protocol implemented during this study period. It is also important to note that the Swedish counterpart only recorded 8.4% participation in physical activities.
These because physical, mental and productive activities have been positively linked to longevity. Findings in leisure activity are incredibly relevant considering the regular participation of the study population and the positive relationship found between leisure activity and longevity, however due to the limitation of the study group in this research, the oldest of the old from the urban counterpart suggests that the senior citizen from the sample can have considerably higher life expectancy as compared to the rural area in the context of age group.
Aside from regular participation in leisure activities one major factor that could affect the longevity of the senior citizens would be apt provision of healthcare and medical assistance. Deficiency of appropriate services and medical supplies can be the cause of decreased life expectancy instead of the characteristics of the population.
Even though the findings of the study concerning leisure activity are encouraging, due to the pandemic the number of leisure activities available for them to do is very limited. Since the answers are based on the respondent's current living situation, the impact of these activities on the senior's overall health cannot be properly evaluated. The lack of historical data regarding any other activities they could have participated in a few years ago before the study period was not recorded.
Table 5. Based on the data gathered, 72 out of 84 respondents said that they never smoked. It could be due to the lifestyle awareness as to how smoking affects one's health. In addition to this, most of the respondents are female, which based on WHO statistics that only 9% of the female population are smokers, hence they are less likely to use tobacco products.
Table 5: Rizzuto, et al, Rocamora M.D., and results comparison. View Table 5
It is noteworthy that the high percentage of non-smokers can be connected to the number of people who didn't have any lung disease as a comorbidity. With this result, it can be interpreted either as a great number of smokers in this generation of seniors had already experienced the fatal effects of smoking, or there's an awareness factor within the study population that has decreased the prevalence of smoking-related diseases.
Nutritional status and comorbidity: A large number of research have confirmed that nutritional status can increase life expectancy and improve quality of life among the elderlies. The assessment of the nutritional status among the study population noted that 23.8% and 3.6% belong to the overweight and obese side respectively. With this in mind the recorded data who are at risks of malnourishment is 8.3%. Comparing with the majority of population in the study who are found to be at a normal nutrition, which suggest that maintaining a good nutritional status has significant implications to health and wellbeing. Meanwhile over and under nutrition increases health risk among elderlies, however in this study there was no correlation in the longevity. This can be due to limited number and restricted age of the participants that were evaluated.
On the other hand, almost 83.4% of the study population has comorbidity at this point time. Among the comorbidities, hypertension (72.6%) is the most prevalent followed by diabetes mellitus (23.8%), then arthritis (15.5%) and cardiovascular diseases (11.9%). Despite only having a quarter of the population as overweight and obese the high number of people with hypertension may be related to the dietary and lifestyle choices of the study population which could be a significant part of further evaluation on the future studies.
Socioeconomic factors and longevity: Socioeconomic factors were divided into 3 categories, living status, educational attainment and job history. Household in the Philippines are composed of extended family members. In this study, participants were evaluated regarding their social network and regarding their living status, most of them are living with their first-degree relatives. However, it was found out that the average age is not correlated with the living status.
Educational attainment and job history were found to have no correlation with age. Majority of the participants were able to reach up to secondary school, with most of them were found to have blue collar jobs. Results were inversely related in terms of educational attainment as average age of no formal education group is higher compared to the average age of participants with primary to tertiary education. This could be of a great interest, in which a retrospective study could be used. A further exploration on the review of literature is also suggested in how unemployment and no formal education can affect the life span of an individual.
Research study among geriatric population is limited in our country hence it is interesting to learn and explore this field of medicine. Factors such as environmental, psychosocial, and biological can heavily influence the longevity of one's life. It is a trait that can be studied using quantitative methods such as surveys. The original goal of the study was to understand and analyze the lifestyle and other factors such as nutritional status and socioeconomic factors that affects longevity. However, further studies with a larger population should be conducted to help in determining whether these lifestyle choices, socioeconomic factors do affect the larger population, or is it just localized.
Given the baseline data collected in urban and rural areas conducted in our country, the information garnered from this study can prove useful to future researchers who wish to revisit this particular sample and establish the sought-after relationships that this research could not. Hopefully, this study will further inspire more people to continue the research that the other researchers have started. It can be used as a baseline for a much bigger study, in a much bigger population, with more opportunities to collect accurate and reliable data in a period without limitations due to a pandemic (Appendix).
Based on the conclusion drawn from the study, the following recommendations are forwarded:
1. A follow up study with the respondents within the next 5 to 10 years can be conducted, to further assess, confirm, and improve the results of the initial research that this research was not able to do.
2. Further exploratory studies on the three categories of geriatric population, namely young old, middle old and old-old, to accommodate and evaluate information of the senior population within the Philippine setting.
3. A review on the relation of cognitive function and longevity, and additional screening and/or confirmatory materials that can help in the evaluation as the factors that can affect quality of life among elderlies.
4. A review on the complete comprehensive geriatric assessment of all elderly in which includes all sample population and its effects on longevity.