Controlling multidrug and extremely drug-resistant tuberculosis (M/XDR-TB) poses a grave challenge to public health, globally. Studies repeatedly show that effective M/XDR-TB management goes beyond strategies recommended in global TB control plans, uniformly pointing to patient-centred care as critical to progress in controlling the epidemic. We aim to describe patient-centred care in M/XDR-TB management in Peru, which presented a context where M/XDR-TB remains a persistent problem, even with increased capacity for diagnosis, decreased costs of treatment, and increased financial and human resources.
We used a case-based study design, purposively selecting urban and rural sites with some of the highest M/XDR-TB prevalence in Peru, employing multiple qualitative data sources: 58 M/XDR-TB patient interviews, 5 provider focus groups, and observations in 8 facilities, which we compared for triangulation and verification. Current M/XDR-TB strategy recommendations, health systems factors, and social determinants were the primary parameters in the analytical framework. Our approach emphasizes patient voices to identify the current status and challenges in providing patient-centered care for M/XDR-TB.
Overwhelmingly, patients were demoralized during the M/XDR-TB diagnosis process. Several factors contributed to fear, frustration, and depression, highlighting the crucial need for psychosocial support. Because CHWs and community outreach were available in one site and not the other, we could identify how these services made critical positive contributions to patient experiences. CHWs as part of M/XDR-TB management and care contributed to patient-centredness and to disease control by: 1) Supporting patients to complete treatment by offering more convenient DOT and providing ongoing psychosocial support; 2) Reducing primary transmission of M/XDR-TB and diagnosis delays with active contact tracing, case finding, and patient education.
Our findings reinforce that it is not direct observation of drug ingestion that is important for TB control, but the continuous support from the health system and community that can be conveyed through regular DOT contacts. Patients need interaction, not observation. If TB programs can provide the right kind of patient-centred DOT - flexible, personal, and convenient - patients say that psychosocial, economic, and motivational barriers to successful M/XDR-TB management are diminished.
The spread of multidrug-resistant tuberculosis (MDR-TB) and the emergence of extensively drug-resistant tuberculosis (XDR-TB) pose a grave challenge to health globally [1-5]. Actors in global TB control have responded in multiple ways, many of them high-profile: the Beijing call for action on addressing the MDR-TB epidemic and the WHA Resolution WHA62.15 in 2009; a subsequent mid-term revision of Stop TB's global plan (2011-2015); two Lancet special series on tuberculosis (2010 and 2013), among others. In addition, there has been continuous updating of MDR-TB management guidelines, including: treatment and management (2011 and 2013), diagnosis using Xpert (2010); rapid MDR-TB screening (2008), surveillance (2009), case-finding (2010) infection control (2009), and ethics (2010). These policies and strategies focus on scaling-up access to drug susceptibility testing (DST), second-line treatment, infection control, MDR-TB surveillance, and country capacity to manage drug-resistant TB [1,6,7]. Programs in the 27 high MDR-TB burden countries also identify their bottlenecks in these terms; human resources for MDR-TB and an array of program management issues were the top two bottlenecks reported in 2011, followed by laboratory capacity and case-finding challenges [4]. Central to recommended scale-up efforts is development of better technologies for MDR-TB: more rapid and comprehensive assay tests for types of resistance; new drugs; vaccines [5-7] progress and investments have been made in these areas, the development and application of these technologies to MDR-TB patients lie relatively far in the future.
Research studies over the past two decades repeatedly show that effective management of MDR-TB requires understanding patient and provider factors that go beyond these recommended strategies [1,8-10]. Since Paul Farmer's research in Haiti in the 1990s, studies around the globe have identified the critical role of psychological, nutritional, and community support for effective drug-susceptible TB (DSTB) and MDR-TB management [11-13]. More recently, socio-economic risk factors (malnutrition, smoking, HIV, diabetes, alcohol use, and air pollution) and demographic trends (urbanization) that increase these risk factors have been identified as social determinants that drive the TB epidemic [9].
These studies uniformly point to patient-centred care and management of DSTB and MDR-TB as critical to progress in controlling the epidemic.
"Problem: Persons with infectious MDR-TB and XDR-TB remain in the community for long periods of time because of delayed diagnosis and initiation of treatment with second-line anti-TB drugs; hospitalization of patients with MDR-TB or XDR-TB poses problem of nosocomial transmission and is costly and inconvenient for patients. Proposed solution: Ensure timely diagnosis and treatment initiation for patients with MDR-TB or XDR-TB; implement appropriate models of care, preferably outpatient, to ensure patient-centered care, avoid disease transmission in health care facilities, and make rational use of financial resources". (p.1053).
Nathanson's proposed solution is not new; the enduring challenge has been to identify context-specific and context-neutral answers to "how" to develop appropriate models of patient-centred care that will reduce delays and increase cure. Patient-centred care is not well-defined, however, especially for TB management, which has historically focused on medical interventions. An early global definition of "patient-centred care" highlights taking into account patient's desires and needs for shared decision-making around diagnosis, treatment, and management [14-16]. A patient-centred medication management framework identifies four critical processes: shared-decision-making; effective prescribing for patient understanding of how and when to take medication; patient feedback and communication; and facilitation of medication-taking, including obtaining medicines and taking them at home [17], all of which are highly relevant for MDR-TB management.
In this paper, we use the MDR-TB control strategy recommendations, focusing on program management and health systems components; a social determinants perspective; and, the stated patient-centred care goal as the framework for interpreting findings from a study of MDR-TB patients in Peru. We focus on describing patients' voices regarding their experiences with MDR-TB treatment, to identify what is needed for a patient-centred MDR-TB control strategy.
Peru accounts for 35.3% of MDR-TB cases in the Latin American and Caribbean (LAC) region and has the highest proportion of MDR-TB cases among all reported TB cases (7.1%) [18]. Within Peru, 58% of DSTB, 82% of MDR-TB, and 93% of XDR-TB cases are in Lima and nearby Callao; outside of the capital, MDR-TB is concentrated in the departments of Ucayali, Madre de Dios and Cusco. The past successes of Peru's National TB Program (NTP) in implementing quality DOTS have been well-documented [10,13,18,19] the incidence of DSTB steadily decreased through the early 2000s, which has recently plateaued. Additionally, drug-resistant forms of the disease are posing a challenge to this historically well-performing TB control program [20]. Since 2007, the number of confirmed cases of MDR-TB has remained steady to increasing, with 1663 confirmed cases reported in 2011 [3].
This is despite Peru's national TB program getting a relatively early and comprehensive start with MDR-TB control. Peru received funding from the Global Fund for second line TB medications at a large scale starting in 2004, with oversight and technical assistance from the Green Light Committee (GLC). A National Reference Laboratory (NRL) with XDR-TB diagnosis capacity was established in 2005, with six more laboratories equipped with DST by 2008 [19]. In 2006, the most recent Technical Health Guidelines for the Control of Tuberculosis were approved, which included specific guidelines for managing MDR-TB. In 2008, cost savings on second-line drugs negotiated by the GLC brought the cost of MDR-TB treatment in Peru down from $30,000 to $5,000 per patient, saving the country 5/6 of the estimated US$24 million a year that were spent on MDR-TB antibiotics in 2007 [20]. However, time to treatment has remained around 5 months, despite the laboratory expansion and treatment investments, or around twice the time needed for the bacterial procedures [21].
Although Peru has quite successfully controlled DSTB, invested in laboratory resources and treatment for drug-resistant TB, and is not a high-burden MDR-TB country, the data show that MDR-TB control continues to be a challenge. The aim of this study was to describe MDR-TB management in Peru using the perspective, and voices, of the patients. More specifically, we wanted to identify possible reasons why MDR-TB remains a persistent problem, even with increased capacity for diagnosis, decreased costs of treatment, and increased financial and human resources.
We used a case-based study design, using purposive selection of study sites based on MDR-TB prevalence, and multiple data collection and analysis methods, including facility observations, review of program data and registers, focus groups, and in-depth interviews with patients and providers who became patients.
Two of the highest prevalence MDR-TB areas in Peru were chosen as study sites: urban La Victoria district in downtown Lima, and the rural department of Ucayali. Migration has caused Lima to grow in a disorderly fashion, creating slums in and around the city, including many in La Victoria, which also has the highest TB incidence rate in Peru - nearly 1,000/100,000 in 2010 [20].
The department of Ucayali, in the Peruvian Amazon, is growing with increasing migration from the Andes and other parts of the Peruvian Amazon. Pucallpa, its capital and home to the main river port, is turning into an urban center for Ucayali. All MDR-TB cases registered in Ucayali are located in the province of Coronel Portillo, which includes Pucallpa, where 77.2% of the department's population lives [18].
Data was collected between April and June of 2011. IRB approval was granted by the Pan- American Health Organization Ethics Review Committee (PAHOERC) and the Ethics Committee at the Universidad Peruana Cayetano Heredia in Peru. Observations included assessment of MDR-TB treatment facilities and of patient-provider interactions within the facility setting. Interviews and FGDs lasted between 60 and 90 minutes; observations lasted 7-8 hours per facility.
A patient sampling frame was created by reviewing MDR-TB registries at 8 facilities (5 in La Victoria; 3 in Ucayali) to identify patients receiving treatment at the time of the study. In La Victoria, purposive, maximum diversity sampling was used to select 39 patients for interviews, out of the total of 68 patients registered; our sample included 4 of the 6 registered XDR-TB patients. In Ucayali, 19 of the 21 registered MDR-TB patients were interviewed, and no XDR-TB patients were registered. We will refer to XDR-TB patients as part of the "MDR-TB" group, which is how they are registered.
For this analysis, we focused on patient in-depth interview data to help explain the current MDR-TB situation in the study sites. Interviews were tape-recorded for transcription and analyzed using Atlas.ti software. Interviews were conducted, transcribed, and analyzed in Spanish; English translation took place after analysis. The second author and a local research assistant coded content independently and discussed discrepancies before performing thematic framework analysis. When necessary, data from interviews were compared with FGDs and observations for triangulation and verification.
In La Victoria, TB and MDR-TB incidence decreased between 2005 and 2010; the proportion of MDR-TB incidence among new TB cases also decreased during this time period from 18.1% to 9.3% in 2010 (Figure 1). However, the rate of treatment loss-to-follow-up (LTFU) was 23% in 2005 and remained high at 24% in 2009 (data for 2010 was not complete). The incidence for TB and MDR-TB was much lower in Ucayali compared to La Victoria (Figure 2). The total number of TB cases slightly decreased since 2005 (213 to 191 in 2010), however, the number of MDR-TB cases increased steadily from two cases in 2005 to 21 in 2010, The proportion of MDR-TB incidence among new TB cases reflects also increased from 0.94% in 2005 to 11% in 2010. Treatment LTFU ranged between 5% and 13%, no data was available for MDR-TB treatment LTFU due to a small sample size. Overall, treatment LTFU rates are much higher for MDR-TB than for DSTB, and the peaks in incidence occurred during 2005 in La Victoria and in 2009 in Ucayali.
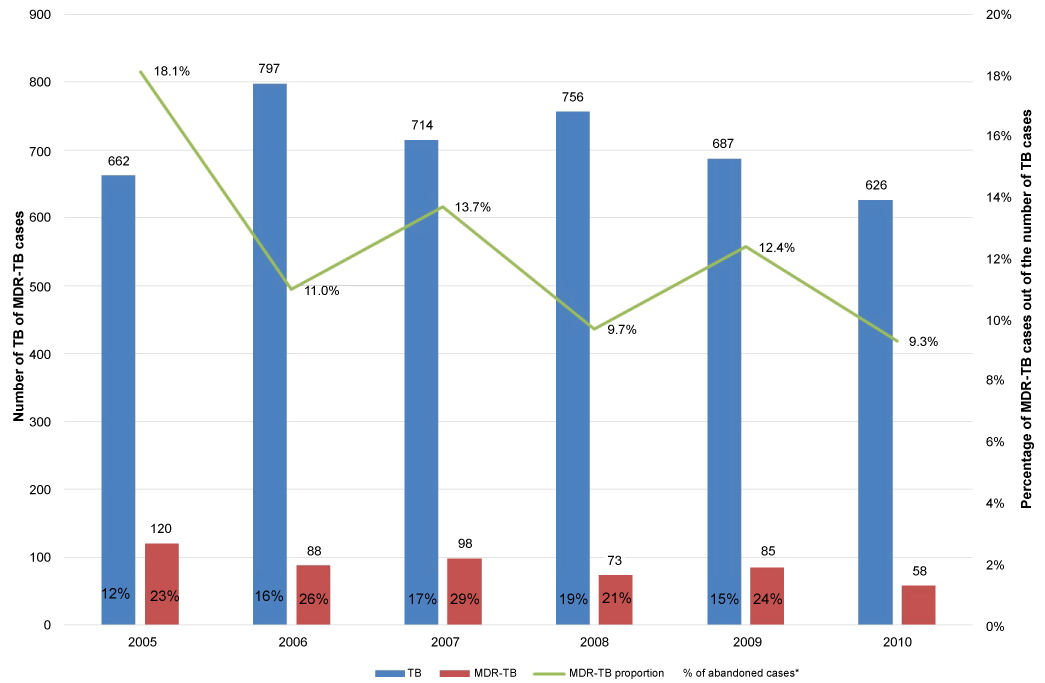 Figure 1: La Victoria: Number of TB and MDR-TB cases, MDR-TB proportion of total TB cases and treatment abandonment from 2005 to 2010.
View Figure 1
Figure 1: La Victoria: Number of TB and MDR-TB cases, MDR-TB proportion of total TB cases and treatment abandonment from 2005 to 2010.
View Figure 1
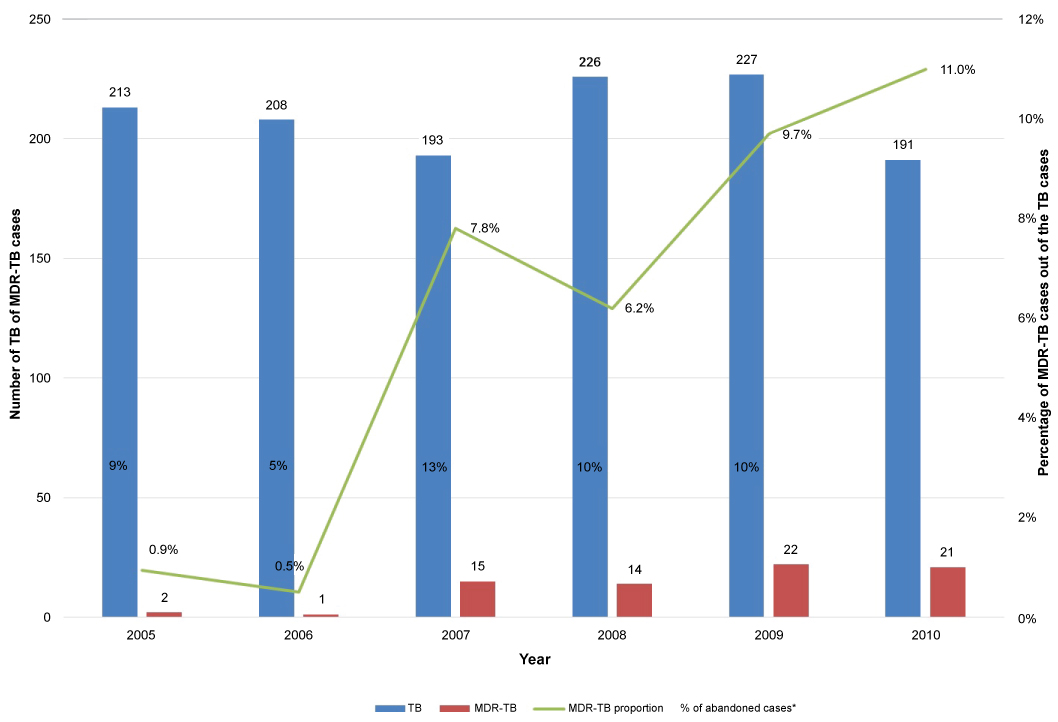 Figure 2: Ucayali: number of TB and MDR-TB cases, MDR-TB proportion of Tb cases, and treatment abandonment from 2005 to 2010.
View Figure 2
Figure 2: Ucayali: number of TB and MDR-TB cases, MDR-TB proportion of Tb cases, and treatment abandonment from 2005 to 2010.
View Figure 2
Patients described several factors that demoralized them during the MDR-TB diagnosis process, especially when they learn that they must wait an additional few weeks after DST confirmation and complete more required tests and visit specialists to receive approval of their treatment before they can finally start taking medications. This is the Peruvian program's process for individualizing the second-line treatment, which may not be fully understood by patients, and therefore creates frustration among patients.
"… [I waited for the diagnosis] for about three months or longer maybe, but she [the nurse] told me that my disease had advanced because I was not taking any medications… so I tell her, if you knew it would advance, why didn't you give me my pills… [the nurse explained that] that is the way it is, first we need to get the order from the ministry, send your medications and what medications we will give you… my lungs must be all destroyed by now, useless probably, I don't know what I am gonna do….[when I was worried waiting] I did not ask any questions, because you know, to get an answer we would need to talk like this, and well, the nurse doesn't have that kind of time…" La Victoria, Female patient, 25
"I am health worker and was in contact with patients… I coughed up a lot of blood one day and was traumatized, and that is when I finally went to the hospital… and I tested positive… when I started treatment I was on first line [medications], a few weeks later they tell me that I had some resistance and changed my medications… and I stopped coughing up blood and was not as tired when I walked… so I thought that was going to be my treatment, but then I got notice that I am multidrug resistant, and then treatment changed again and I was very scared, and so much time had passed… it was 4 months wasted, completely wasted... it was bad, I was devastated because I knew what was coming and I was depressed, but it passed because I knew I was with my mom, there were people who supported me and I wanted to continue with [my studies], that helped me get out of my depression crisis…"
Ucayali, Female patient and health worker, 23
"(my reaction) to the diagnosis was normal, as if I had been bitten by a mosquito… because they (medical practitioners) had not explained anything (about TB or MDR-TB) to me".
Ucayali, Male, 30
In Peru, MDR-TB treatment is provided on an outpatient basis. Most patients must take two doses per day, Monday through Saturday, for a minimum of 18 months. In the study sites, MDR-TB treatment facilities are typically open 6 days per week, from 7:30 am until 12 or 1 pm. For the majority of patients interviewed in both La Victoria and Ucayali, the morning dosage was usually observed in the health facility. The evening dose presented more problems for patients. In Ucayali, MDR-TB treatment was provided only at the regional hospital at the time of the study, and there were no CHWs in place. The distance to the regional hospital for patients ranged from a 5-minute walk to more than 2 hours each way, requiring walking and other forms of transportation. Patients described how money and time costs for transportation became prohibitive. A few patients actually moved closer to the regional hospital in Pucallpa to facilitate obtaining their medications.
"… thank god I had a little money saved up (to cover treatment costs)… I leave home at 5 am to walk and then look for a car to bring me here for about $0.75, then I walk again, after that (taking medications) I have to go to work and pay $1 (for transportation).. sometimes I leave (home) without eating because I am in a hurry to get here, by 8 am".
Ucayali, Male, 52 "(walking) it takes (me) about 30 minutes, and then the motorcar charges me $0.50 for the rest of the way". Ucayali, Female, 35
In La Victoria, most patients were able to walk a short distance to a health facility for the morning dose and make arrangements with CHWs to take their evening dosage at home, work, or another convenient location. If a patient was bed-ridden or required delivery of medication for both morning and evening dosages, exceptions are made to allow CHWs to provide both, "as long as the patient shows commitment to adhering to his/her treatment" [Provider, La Victoria].
In Ucayali, the head nurse is the only person who waits on MDR-TB patients 2-3 nights a week to observe their evening dosages. Many patients were either given their evening dosage in the morning for them to take it on their own or told to return at night if the head nurse was on night shift. During the study period, we observed that at least 9 of the 28 registered patients were inconsistent with the evening doses or had not taken their medications for at least 2 weeks. These system-induced increases in default risk were not noted in La Victoria. Without the CHWs, MDR-TB cases increase pressures on the TB staff and on patients for direct observation, especially for the second of the daily dosages.
"With the number of staff and the distribution of working hours right now, there simply isn't supervision of the treatment that needs to be given to them (patients) in the evenings… the guidelines say we need to supervise treatment morning and evening, which is how the schedule works for drug-sensitive TB cases, but it is not our reality (for MDR-TB cases)…"
Ucayali, Nurse, TB unit
"At night, it (the hospital) is not close anymore…. So, I told the nurse that I cannot come at night, 'if you could just give me (the evening medications) because I have no problem taking them on my own' because I know that there are some people, and I will be honest with you, some don't take their evening medications…"
Ucayali, Female, 27
Nutritious foods are an essential part of MDR-TB treatment, and Peru's TB Guidelines require pyridoxine (vitamins) as a complementary treatment to avoid adverse effects from TB medications. They also recommend a visit to the nutritionist. Food support in the form of baskets of staple foods is also part of MDR-TB program services.
In La Victoria, patients reported 1-2 visits with a during their treatment period. However, nutritionists are not trained to advise complex cases of MDR-TB patients who live in poverty and experience co-morbidities, such as diabetes. Patients often ended up confused by conflicting advice from the nutritionist and their TB care provider:
"Yes, there is (a nutritionist), I had visits with her, but she sometimes tells me 'you shouldn't eat this', but at the health center they tell me I have to eat, if I don't eat I will get sick again, of course they tell me to eat… but the missus (nutritionist) tells me 'don't eat too much flour, too much bread', that I shouldn't eat too much noodles, but I always eat them".
Female, La Victoria, 38, diabetic
In Ucayali, nutritionists were not on staff at the Regional Hospital, but some MDR-TB patients reported receiving food baskets occasionally. In La Victoria, patients said they received food baskets monthly, but since these included only common food staples, patients did not think they helped with recovering from a serious disease like MDR-TB.
"What lacks most (in terms of services) is nutrition, there are many people who come from the [rural sections of Peru]… they are renters and sometimes it (money) is not enough for water, electricity, so they take away from their nutrition (to meet needs)… if you want to heal, you have to eat well". Female, La Victoria, 35
"… more than anything (what is missing in the food baskets is), milk and vegetables, because we know that we need them to get better…"
Female, La Victoria, 40
However, for many patients in La Victoria the contents of the food baskets were not practical because they work all day and eat their meals from street vendors; many do not cook at home. The quality of the rice and beans was also criticized, in terms of costing more to cook than their worth in cooking fuel.
"they (health center staff) give you legumes you can't even cook because they are very hard and a lot of (cooking) gas is wasted…, so I end up buying better ones (legumes) to save on gas".
Female, La Victoria, 26
Peru's 2006 TB Guidelines require that MDR-TB patients meet with psychologists as part of the pre-treatment assessment, to identify existing psychosocial barriers. Nurses are expected to follow-up on emerging problems during treatment, and interviews with the social worker are recommended. Although objectives for these interviews are outlined in the guidelines, it does not specify timing, frequency, methods for monitoring, or content for what to do when complications emerge.
"As you can see, we provide integral patient care here, but in all the services, the biggest problem, or factor, is the emotional (aspect) so this requires going more often to the psychologist…"
La Victoria, Physician, TB unit
"the problem of (treatment) abandonment is a psychological one, there is no one who fills the void and the person feels let down, bad, and there is no one who encourages them, uplifts them, to end the treatment… the other problem is having to stay away from people, hiding (to avoid infecting others)… it is a problem that is very personal".
La Victoria, Male, 21, XDR-TB
In both study sites, patients also complained about the type or lack of psychological support they received. The visits were described as meetings with a psychologist or social worker just to fill out forms. One patient described her experience as a waste of time.
"… (The psychologist) had to fill out a questionnaire, with questions, like 'do you smoke?', 'do you use drugs?', like that… that was it".
Male, La Victoria, 47
Patients said that psychologists did not inspire trust and they did not jointly make a plan to overcome or address any anticipated problems. Study observations validated that pre- treatment assessments often did not occur in a private space for the patient to express their problems.
"I consider this (psychological support)…not sufficient, you are barely in (diagnosed) and they send you to a psychologist, someone you have never met who you probably do not trust at the moment, you come in destroyed (emotionally), perhaps it is not enough, and it is the only time they send you to a psychologist, but not necessarily when they see that you are doing badly (emotionally), I think the psychologist should be smarter… you see, there are many patients who abandon this treatment".
La Victoria, Male, 21
The timing of psychological visits could be planned better to actually meet patient needs. One patient explained, "it was too late, [she] had already passed the most critical moments" [Ucayali, female, 24]. Patients expressed the need for ongoing counseling, especially while enduring severe side effects.
"Psychologically, they (medications) are affecting me, I am sad, I get very sad even when there are people around me, and I want to talk to someone, but I still feel like sadness takes over me and I cannot get rid of it…. I have been to the psychologist twice, but it is not enough…"
Ucayali, Female, 24
"I would like to make a request, and (I hope you) this can reach (authorities) too… I would like there to be a permanent psychologist (counselor) even if twice a week, for everyone who suffers with MDR-TB… people sometimes do not want to take (their medications) just because they lack knowledge or psychological and emotional support".
La Victoria, Male, 32
However, what patients highlighted again and again was the stress and agony of initial diagnosis, starting treatment, and then finding out months later that they had drug-resistant TB, and needed to start another type of treatment. This seemed to be when patients lost their confidence in the health system, and when psychological support could make a real difference.
"…at the beginning it was the worst, things got complicated for me, I got depressed and I cried everywhere, every day, I would think about my children and what would happen to them if I died, I was feeling bad… for about 4 months".
La Victoria, Female patient, 52
"…when I started coughing up blood, that's when I got scared, ran to my house, and they brought me here to the hospital… and I was diagnosed [with TB] but a little more information from the doctors would have been helpful. My sensibility test took 5 months, I only received my notice that I was resistant almost finishing my first treatment,… that really, it made me very mad, I was very mad because I thought that that was something that they should explain to you… that there are different types of TB, but never, I always thought it was just one type, and I didn't even find out from [the hospital], but from the newspaper… [when I found out] I started to cry uncontrollably, like I had been deceived… I got very depressed, I was very depressed because after all that I went for almost 6 months without knowing that, without knowing that I was MDR… I wanted nothing to do with [the hospital] anymore… I returned another 5 months after [diagnosis], when the symptoms came back…"
Ucayali, Male patient, 20
The MDR-TB programs and health systems structure were not the same in the two study sites (Table 1). In Ucayali, only one facility actually provided MDR-TB services, whereas there were five in La Victoria; all study sites had a TB physician. Ucayali did not have dedicated MDR-TB staff at the time of the study; one was trained three months prior to this study.
Table 1: Health system resources for MDR-TB program. View Table 1
The biggest difference between the study sites is in terms of the "peripheral" services of the MDR-TB program: CHWs, nutritionists, psychologists, and community outreach were available in La Victoria but not in Ucayali. Ucayali had no plans for CHWs or nutritionists, or for TB training for the psychologist.
In La Victoria, patients said that the CHWs provided ongoing emotional support to help them successfully continue and complete treatment. CHWs facilitate treatment access, as a more flexible source of medications and direct observation and play to increase the likelihood of successful treatment of MDR-TB. In contrast, Ucayali, where CHWs were not part of regular MDR-TB care, DOT was difficult to administer and the specific needs of patients without family support were difficult to meet, more often leading to irregularity of lack of monitoring of treatment, increasing risk of default.
CHWs also perform weekly active contact tracing for MDR-TB patients in La Victoria, which may be the key factor in bringing down incidence since 2008. In Ucayali, medical staff conduct contact tracing on an ad hoc basis, using their own transportation to take on overtime duties that are neither compensated or recognized. CHWs address 3 of the 4 primary problems MDR-TB patients identified: health system capacity for DOT; provision of psychological support; adequate information about TB, drug-resistance, and treatment processes.
We acknowledge the small scale of this study but posit that it demonstrates type of research that is needed to understand the current MDR-TB management situation. Although we selected a study site that is not a current HBC, Peru had been one, and although it is not an MDR-TB HBC, it faces a stubborn MDR-TB epidemic, with more than 35% of MDR-TB cases in the LAC region. We find that this context provides a rich opportunity for learning, and is not a limitation, but a strength. Peru was also a pioneer site for establishing that community-based MDR-TB management was effective and has invested in MDR-TB control resources for more than 10 years. The study sites are where MDR-TB is concentrated, in urban and urbanizing areas that harbor "hot-spots". Our findings, therefore, show the MDR-TB situation when DSTB control has been successful, and resources and capacity for MDR-TB management have been increasing.
The specific programmatic challenges and gaps identified in this study are likely to be different in other settings, even in Peru, but because findings emerged through examination of actual experiences of MDR-TB patients, it is likely that people suffering from MDR-TB in other settings experience similar fears and frustrations as identified in this study.
TB program data from Peru, including financing data, has been available in less detail since it was removed from the HBC list. Handwritten registry entries and patient histories were not always legible or complete, which could have led to under-reporting of default or total caseload. However, because we focus on patient voices here, we consider that these limitations do not affect the interpretation and relevance of the study findings.
As with many other studies, we find that non-medical factors are extremely important for successful MDR-TB management. We find this even in a context where DSTB has been successfully managed. Overwhelmingly, patients were demoralized during the MDR-TB diagnosis process. Given the complexity of MDR-TB diagnosis, delays are inevitable to some extent. However, patients also arrive at TB programs already scared, tired, and frustrated with care-seeking and illness. These factors contributed to fear, frustration, and depression, highlighting the crucial need for psychological support.
In describing their experiences, MDR-TB patients in urban and rural Peru identify an array of program management, socio-economic, and health systems factors that make it even more difficult for them to manage their diagnosis and treatment processes, especially the mental, physical, and financial side effects, over the course of 18-24 months. First, patients had already spent significant money on medications to soothe their symptoms and visiting public or private providers who did not give them appropriate TB care. They also lost money when they missed work due to their symptoms and time spent in care-seeking. Second, patients described feeling frustrated and scared while waiting for their test results. Third, patients felt depressed once they received positive results for TB. Fourth, patients who initiated first-line treatment for TB for several weeks or months before confirmation of their MDR-TB diagnosis stated that they wasted their time and made sacrifices in vain; they described a difficult psychological process to first accept that they had not been cured after what already seemed like long treatment, and then ready themselves for a much longer and more difficult MDR-TB treatment.
Most of these factors could be addressed through TB programs efforts: 1) Low capacity for providing accessible, convenient DOT of twice-daily medication doses, which incurred financial and motivational costs; 2) Missed opportunity to use DOT to interact with patients and provide psychosocial support and information about the disease; 3) Assessment and re-design of nutritional support to make it more locally attractive and useful.
Because CHWs and community outreach were available in one site and not the other, we could identify how these services made critical positive contributions to patient experiences. The role of the CHW in La Victoria was critical, for DOT of the twice-daily dose of medication that MDR-TB patients must take, and especially for psychosocial support of patients who must manage their treatment and its physical and mental side effects over 18-24 months. Patients described the CHWs addressing 3 primary MDR-TB management challenges that patients themselves identified: low health system capacity for twice-daily DOT; lack of ongoing and timely psychosocial support; accurate and interactive information about TB, including drug-resistance and transmission.
The importance of community contributions to TB care has been proposed and documented for nearly two decades [12,22-27]. Pioneering research in Peru itself demonstrated that ambulatory MDR-TB DOT could be effective; however, the model tested was highly dependent on community-based volunteers [13,28]. Community-based, ambulatory TB care has been shown to be cost-effective, as well, from South Africa to Nepal, Pakistan, Bangladesh, and Ethiopia [29-32]. A systematic review of evidence on DOT effectiveness showed that from the existing trials, DOT did not provide a solution to poor adherence in TB treatment. The trials did show that community support and frequency of contact with a support source, be it a family member, community health worker, or other provider, improved the quality of TB management. MDR-TB treatment effectiveness will likely depend on developing more locally appropriate models of patient-centred MDR-TB care [33,34]. In our study, community-based support as a routine part of MDR-TB management and care contributed to patient- centeredness and to MDR-TB control in two ways: 1) Supporting patients to complete treatment by allowing more convenient DOT and providing ongoing psychosocial support; 2) Reducing primary transmission of MDR-TB and diagnosis delays with active contact tracing, case finding, and patient education.
The most frequently identified problems to be addressed as part of optimizing MDR-TB management and care are the delay in diagnosis of drug-resistance, with ensuing increased risk of infection in the community, and the costs and inconvenience of hospitalization to patients, and increased risk of infection for hospital staff. Our study identifies psycho-social and financial issues that erode trust among patients and erect barrier to continuing treatment to completion as equally important for effective MDR-TB management and care. Locally adapted community-based MDR-TB services, which offer alternatives to facility-based DOT, is the key to successfully addressing all of these problems.
Our findings reinforce that it is not direct observation of drug ingestion that is important for TB control, but the continuous support from the health system and community that can be conveyed through regular DOT contacts.
TB programs should prioritize ensuring that communities receive appropriate and consistent education regarding MDR-TB, that patients receive psychosocial support, especially during the waiting times for diagnosis and treatment initiation, and that nutritional education and assistance is appropriate and consistent, early on and throughout the treatment process. If TB programs find a locally appropriate way to provide the right kind of patient-centre DOT - flexible, personal, and convenient - patients say that psychosocial, economic, and motivational barriers to successful MDR-TB management are diminished.
As we wait for better MDR-TB diagnostic technologies, drugs, and, hopefully, a TB vaccine, the voices of MDR-TB patients tell us what needs to be done. Patient-centred care is not a stop-gap measure until newer and better technologies arrive, but a long-term investment with significant positive returns that our study shows is still needed even in lower-burden settings that have successfully managed DSTB, as in Peru. These are the future scenarios and challenges for current HBCs. MDR-TB patients are saying: We need interaction, not observation.