The outbreak of COVID-19 pandemic in the world especially in African continent and Nigeria in particular has created negative effects on humanity. Continuous holding on to some misconceptions about the reality of the virus among people may create further problems for humankind. However, very few studies particularly in Nigeria have actually considered the implications of these misconceptions about the disease in relation to its daily increases; coupled with the fact that many people still hold on to some of these misconceptions in the country. Therefore, this study examined the implications of some common misconceptions among people about COVID-19 pandemic in relation to its daily increases in Nigeria.
This study has documented some of the most common misconceptions about COVID-19 pandemic among few individual persons - both male and female in a neighbourhood area of Ibadan in southwestern Nigeria. These include: "it is white people disease"; "it is an imported disease"; "it is the disease of the wealthy people"; "incessant heat in Nigerian environment will destroy the disease (i.e. hot weather)"; "poor people cannot contract it"; "maintaining physical distancing practice is unnecessary"; "taking local herbs will destroy it"; "taking hot drinks (local gins) will destroy it"; "wearing of face masks is not necessary"; etc. both in rural and urban areas. Daily increase in the cases and fatalities of the virus in the country has been suggested in this study to be as a result of tenaciously holding on to these belief-systems among people. Virtually, all sectors in the country such as health, economy, transportation, agriculture, education, security, politics, religion, family, sport, entertainment, etc. have been seriously affected and still being threatened by the virus. Consequently, the negative impacts have been enormous on people' jobs/works, businesses, family life and social relations thus creating more harms than benefits.
Therefore, positive change in people' health-related behaviours becomes imperative through effective and active public enlightenment and awareness creation with strict compliance to the prescribed preventive measures being put in place by the key stakeholders regarding the virus. This will go a long way in influencing positive health-related behaviours among people, getting rid of some misconceptions about the disease that may trigger larger community transmissions as the efforts to discover new vaccines or drugs for COVID-19 pandemic treatment continue.
COVID-19 pandemic, Virus, Disease, Misconceptions, Effect, Health belief-systems, Nigeria
COVID-19: Coronavirus Disease 2019; SARS-CoV2: Severe Acute Respiratory Syndrome Coronavirus 2; SARS-CoV: Severe Acute Respiratory Syndrome CoV; MERS-CoV: Middle East Respiratory Syndrome CoV; CoVs: Coronaviruses; nCoV: novel Coronavirus; NCDC: Nigeria Centre for Disease Control; WHO: World Health Organisation
There is no doubt that virtually the whole world is already in the midst of COVID-19 pandemic especially in African continent and Nigeria in particular. Coronavirus disease pandemic otherwise known as COVID-19 pandemic started in Wuhan, China in December; 2019. The starting point of the virus was Hunan seafood market, Wuhan, China [1]. The novel coronavirus (2019-nCoV) was pronounced a public health emergency of international concern and tagged COVID-19 pandemic [2-6]. The serious global emergency of the virus caused its declaration as a pandemic [7] and this is based on growing number of cases notification in China and other countries [4]. The virus is spread from person to person through direct contact and it is highly infectious and can be transmitted through droplets and close contact with infected people that are coughing, sneezing, respiratory droplets, and moreover it remains a bat-related epidemic [1].
However, there is an issue of cases of asymptomatic individuals with the virus. Thus, COVID-19 pandemic can present as an asymptomatic carrier state, acute respiratory disease and pneumonia affecting patients in all ages [8]; which play a major role in the rapid transmission of the virus among people thereby posing more serious health problem [9]; severe cases are more likely to be among older people with increased underlying diseases compared to mild cases [8]. Thus, classification of patients with COVID-19 is based on a combination of clinical, epidemiological and laboratory findings [10]. Moreover, healthcare settings or public places are a potential source of viral transmission through frequent touching of surfaces. Also, the virus can remain infectious for up to 9 days on surfaces [11].
Since the outbreak of the virus, many human deaths have been reported daily across the world. The cases of the virus continue to increase despite the global efforts to contain it [3]. So far, no vaccine or drug has been discovered for its treatment [12]. That is, effective treatment for the virus is not available [8]. Currently, there is no available vaccine against SARS-CoV-2 [13]; no definite treatment for SARS-CoV-2 is available [14]. The complete clinical classification of the virus is not yet fully understood [15] but enhanced surveillance and further investigation are ongoing [16]. The success of the current research activities on possible treatment for the virus is yet to be seen [17]. Hopefully, the vaccines or drugs would be made available on time.
In spite of the daily increases in the cases and dead rates due to COVID-19 pandemic in the world and the global efforts to contain the virus; it has been reported in some part of the world especially in African continent such as Nigeria, Ethiopia and Asian region - India, etc. that there are some misconceptions about the virus among people [18-21]. Continuously holding on to some misconceptions in the midst of COVID-19 pandemic may create more harms than benefits. Thus, its consequences might be enormous and have negative impacts on humanity. This remains a serious concern.
It is obvious that the daily increases in cases and fatalities about COVID-19 pandemic in the world has continued to create enormous threats to virtually all sectors - economy, transportation, education, agriculture, religion, politics, security, etc. in the society; despite the concerted and collaborative efforts being put in place to control its spread in the world especially in African continent and Nigeria in particular. In fact, it is already having negative impacts on almost every sector in the society. Some of these negative impacts on the society have been reported [1,14,17,22-24]. Thus, concerted efforts with quick and active responses from major stakeholders in the world in fighting the virus become important.
However, very few studies in Nigeria have actually considered or examined the implications of these misconceptions about the disease in relation to its daily increases; coupled with the fact that many people still hold on to these misconceptions in the country. Therefore, this study examined the implications of some common misconceptions about COVID-19 pandemic in relation to its daily increases in Nigeria.
Since the outbreak of the virus in the world; many researches (studies) have been conducted and still being carried out in order to give detailed explanations about the virus including its aetiological and epidemiological elements and classifications. Coronavirus disease pandemic started in Wuhan, China in December, 2019 [1]; its starting point was Hunan seafood market, Wuhan, China [1]. Previously it was named as novel coronavirus disease 2019 (2019-nCoV) [25]. After less than four weeks, it spread from Wuhan to other parts of China and to the world at large [26]; a novel coronavirus that took not only the China but the entire world by surprise and has continued spreading widely to other parts of the world [22,27,28]. Since then, thousands of cases and fatalities due to the virus have been reported daily across the world.
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) was reported to have been responsible for COVID-19 pandemic [25,29]; named by WHO from (SARS-CoV-2) to 2019 (COVID-19) [22] and is a highly transmittable and pathogenic viral disease [29]. Different from both MERS-CoV and SARS-CoV; 2019-nCoV is the seventh member of the family of coronaviruses that infect humans [16]. Its main symptoms include fever, fatigue and cough, which are similar to that of SARS CoV and MERSCoV infected cases [22]; coughing, sneezing, respiratory droplets, etc. [1].
Both SARS CoV and MERS CoV are the two highly transmissible and pathogenic viruses that emerged in humans at the beginning of the 21st century [30]. It is likely that both viruses originated in bats [30,31]; that is, SARS-CoV and MERS-CoV had been discovered in bats in the world [30]. So, continuous spreading out of viruses from their natural places to humans and other animals is largely due to human activities such as urbanisation and mechanisation of agricultural practices etc. [30]. Strong indication of human-to-human spread and sustained human-to-human transmission has been reported [32]; occurred among people with close contacts since the middle of December 2019 and gradually spreading out within a month afterwards [33].
Currently, no scientifically, medically or clinically approved vaccine or drug has been discovered for its permanent treatment [12]; no definite treatment for SARS-CoV-2 at the moment [14], no clinical treatments or prevention strategies are available for any human coronavirus [30]. Though, trials of drugs to prevent SARS-CoV-2 infection have started in some countries in the world such as USA, Spain, etc. [14]. Since this virus is new, much knowledge about this novel virus is limited [1]. There is still limited knowledge and research regarding the COVID-19 pandemic related-health issue [25]. The complete clinical classification of the virus is not yet fully understood [15]. In fact, the trend of the virus majorly depends on suspected and isolated cases [34]. So, enhanced surveillance and further investigation about the virus are ongoing [16].
From the inception of the outbreak of the virus in the world; many unverified information and beliefs have been going round especially in African continent and Nigeria in particular probably due to insufficient information about the behaviour and characteristics of the virus. Misconceptions are misleading and erroneous pieces of information. They could be regarded as mistaken thoughts or ideas that have been trending in society, mostly leading to malpractices in terms of health beliefs and health seeking behaviours [35]. Thus, there are many misconceptions regarding COVID-19 pandemic and people tend to believe every little thing that is circulated in the society without confirming it [21]. Some studies have reported some of these misconceptions about the virus among people.
Moreover, it has been reported that many people believed that; "exposing yourself to the sun or to temperatures higher than 25 ℃ will prevent the virus", "the ability to hold your breath for 10 seconds or more without coughing or feeling discomfort means you are free from COVID-19 pandemic or any other lung disease", "drinking alcohol protects you against COVID-19 pandemic and is not dangerous", "COVID-19 virus cannot be transmitted in areas with hot and humid climates", "religious chants can kill the virus", "if I am young and healthy; I don't need to follow precautionary steps or physical distancing", etc. [21].
Similarly, a study in Nigeria reported that some people believed that "COVID-19 pandemic is not real", others "believed that it is indeed real but cannot affect the poor or those who do not travel beyond the country", thinking that "some sorts of alcoholic substances and concoction could cure the virus or prevent them from getting infected", "believing that it is a "rich man's virus" and therefore it cannot affect the poor masses". Others believed that "COVID-19 pandemic cannot survive in a region around the equator as the temperature would kill it" [18]. Also, another study in Nigeria reported that one of the most frequent responses on misconceptions about COVID-19 pandemic is that "the virus was created in a laboratory" [19]. Moreover, another study in Nigeria has reported that some people believed that COVID-19 pandemic was "a biological weapon designed by the Chinese government" and "consuming gins, garlic, ginger, herbal mixtures and African foods/soups as preventive measures against COVID-19 pandemic" [20]; though, both studies in Nigeria were not peer reviewed. That is, the studies were not certified by peer review process as authors reported [18-20]. However, their studies cut across both rural and urban areas. Also, the findings (that is, the three reports from Nigeria) are a clear indication that misconceptions about the virus are still prevalent in the country.
Contrary to the common belief from social media that "the economically poor countries such as many African countries and India will be to some extent less affected by COVID-19 pandemic than the high-income countries such as the USA, UK, France, Italy, etc." has been proved wrong [36]. This is because; the virus has been spreading widely regardless of countries' economic status. So, the belief that economically poor countries have better immunity is mere misconception [36]. Also, a study among US and UK participants "believed that children were at an especially high risk of death when infected with SARS-CoV-2" and "thought it was necessary to stop eating at restaurants belonging to the Chinese" [37]. However, both World Health Organisation body and other major stakeholders from different countries in the world especially in African region and Nigeria in particular have not ceased in dismissing some of these misconceptions about COVID-19 pandemic among people as false and misleading.
Moreover, it might be the most difficult thing to address if people continued spreading rumours about the COVID-19 pandemic and not cooperating with government officials [21]. Apparently, no single method could address all the myths, fallacies and misconceptions regarding health issue in society [35] but different approaches.
On the other hands, some studies have reported on people knowledge about the virus to be having good knowledge especially in African continent and Nigeria in particular. For instance, an online survey among residents between ages 18-39 years in North Central part of Nigeria reported that majority (99.5%) of respondents had good knowledge of the virus, mainly acquired through the internet/social media and Television respectively. Also, the majority (79.5%) of respondents had positive attitudes to the prescribed preventive measures such as practising social/physical distancing, wearing of face mask, etc. believing that social media contributed immensely to their knowledge [38]. Similarly, another study in Nigeria tentatively affirms that Nigerians aged 15-70 years have high knowledge of the virus and TV and Radio are their main sources of information about the virus [20].
Some studies outsides Nigeria have also reported high knowledge and good preventive practices about COVID-19 pandemic such as among Malaysians [39]; Pakistanis [40]; adult people residing in the United States and the United Kingdom [37]; among student population (both male and female) in Italy [29]. Though, some of these studies were not certified by peer review process as authors reported [29,40]. On the contrary, a study among chronic disease patients in Ethiopia revealed that many of the patients had poor knowledge and practice about COVID-19 pandemic. Some of the major preventive measures such as physical distancing and avoiding visiting crowded people and places were perceived as very difficult things to do among the participants. Low educational level, living in rural area and low monthly income were significantly related to their poor knowledge and poor practice about the virus [12].
Generally, it has been observed that many people are still having some misconceptions about coronavirus disease pandemic despite the huge number of cases and fatalities being reported daily in the world. This study examined and documented some of the common misconceptions - belief-systems about COVID-19 pandemic among few individual persons - both male and female in a neighbourhood area of Ibadan in southwestern Nigeria. These include: "it is white people disease"; "it is an imported disease"; "disease of the wealthy/rich people"; "incessant sunny/hot and heat weather in Nigerian environment will destroy it"; "the poor people cannot contract it"; "maintaining physical distancing practice is unnecessary"; "taking local herbs will destroy it" "taking hot drinks (local gins) will destroy it"; "wearing of face masks is not necessary;" etc.
Thus, some of these misconceptions have actually made many people to openly disregard the prescribed preventive measures being put in place, such as compulsory wearing of face mask in public places; maintaining physical distancing of at least 2 metre apart from other people; regularly hand washing with soap or alcoholic-based agents; never touching your eyes, nose, mouth whenever you are not too sure of the cleanliness of your hands; immediately report whenever you or your neighbours show COVID-19 pandemic-related signs or symptoms, etc. These belief-systems and misconceptions might have both serious medical/clinical and social consequences for people.
Consequently, the negative impacts have been enormous on their jobs/works, businesses, family life and social relations. Obviously, they are not comfortable with these negative effects despite the fact that; they still hold on to some misconceptions about the virus. It is possible that sustaining or continuing with this type of belief-systems during the COVID-19 pandemic period will go a long way in creating more harms than benefits. Currently, all the 36 states in Nigeria including Abuja the Federal Capital Territory, have reported confirmed cases of the virus [41].
In Table 1, the first cases of coronavirus from 31st December, 2019 to 20th January, 2020 were reported [42].
Table 1: Countries, territories or areas with reported confirmed cases of 2019-nCoV, 20th January 2020. View Table 1
While the first cases of deaths from the virus were reported on 22nd January, 2020 with six deaths from Wuhan [43].
However in Table 2, as at 30th June, 2020; 10,185,374 cases (163,865) and 503,862 deaths (3,946) have been reported globally; while in African continent, 297,290 cases (8,943) 6,010 deaths (131) respectively including other regions [44].
Table 2: Situation in numbers (by WHO Region). View Table 2
From Figure 1, the trends of the virus from 30th December, 2019 to 30th June, 2020 have been rising steadily but it appears the curve is coming down gradually in late June 2020.
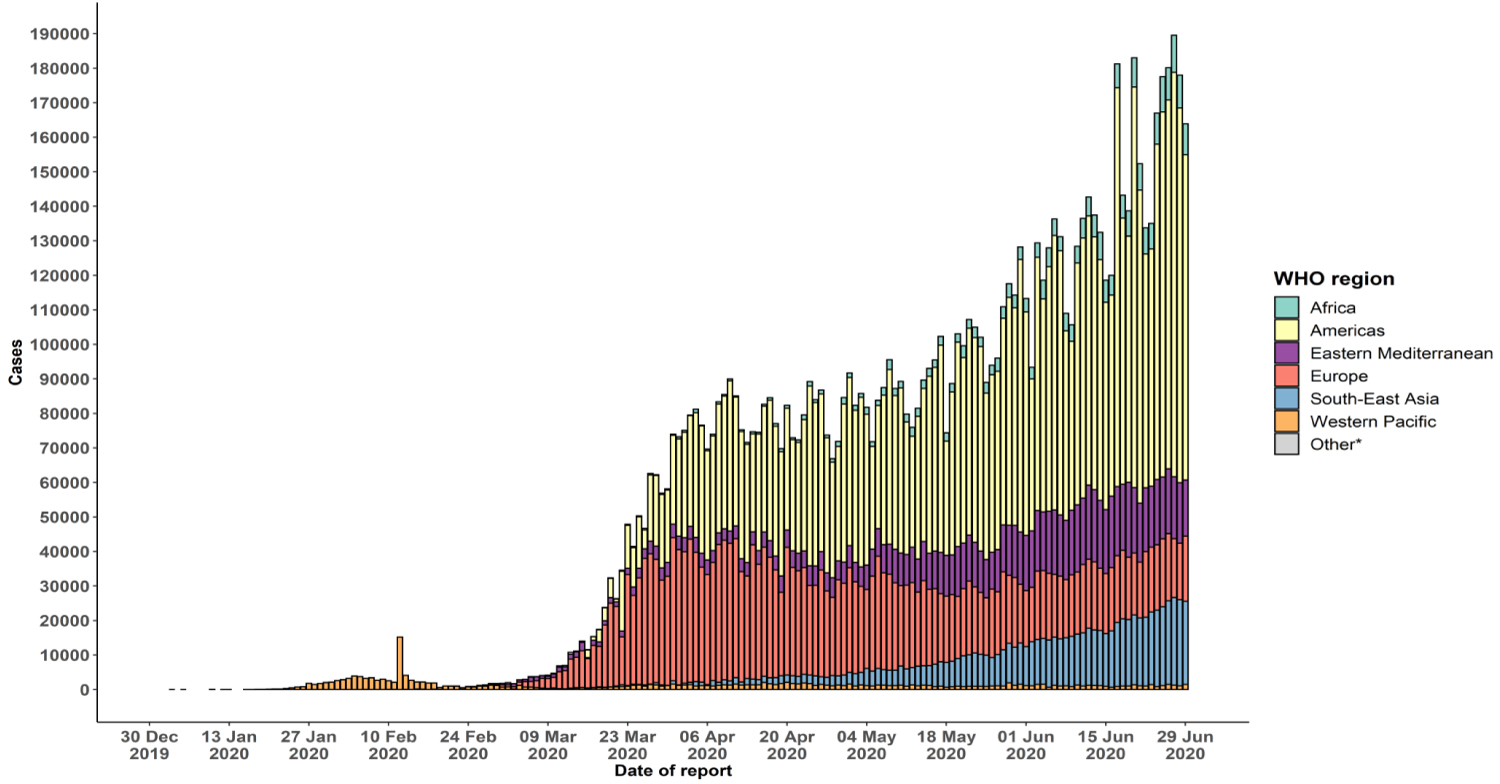 Figure 1: Number of confirmed COVID-19 cases, by date of report and WHO region from 30th December, 2019 to 30th June, 2020.
Figure 1: Number of confirmed COVID-19 cases, by date of report and WHO region from 30th December, 2019 to 30th June, 2020.
Source: World Health Organisation, 2020: June 30 update.
View Figure 1
The widespread of the virus does not spare African continent. Many countries in Africa have been battling with the virus. The first cases were reported in Algeria on 25th February 2020, since then the virus has continued to increase in cases and fatalities [45]. Figure 2 shows the daily number of confirmed cases of the virus from 25th February to 23rd June 2020.
 Figure 2: Daily number of confirmed COVID-19 cases in the WHO African Region by country from 25th February to 23rd June, 2020 (n = 236,909).
Figure 2: Daily number of confirmed COVID-19 cases in the WHO African Region by country from 25th February to 23rd June, 2020 (n = 236,909).
Source: WHO African Region, 2020: June 24 update.
View Figure 2
From Table 3, more than 20 countries in Africa have recorded more than 1000 cases of COVID-19 pandemic each with South Africa ranks the highest (106108 cases) followed by Nigeria with 21371. Likewise, South Africa also has the highest death rates (2102 reported deaths) from coronavirus disease. On the other hands, Uganda, Eritrea, Namibia, Lesotho and Seychelles have not recorded any case of death from the virus. Out of 236909 reported cases of people with coronavirus diseases in the continent; 120089 people have recovered from the virus. Unfortunately, 5824 health practitioners alone in the continent have contracted the virus perhaps due to the nature of their work. They are actually the ones treating people with the virus. Moreover, South Africa tops the list with 2084 health workers that have contracted coronavirus disease in Africa. Thus, it is important to note that sustaining safe and quality care during this pandemic relies on the health and mental wellbeing of the frontline health practitioners [23].
Table 3: Number of confirmed COVID 19 cases in the WHO African Region, 25th February to 23rd June 2020 (n = 236,909). View Table 3
As at 30th June, 2020; the figures have been reported to have increased to 297290 cases (8,943) and 6010 deaths (131) respectively in Africa [44]. The rate at which the virus is spreading and rising in African continent is quite alarming though unlike the more developed countries such as the USA, Italy, Spain, UK, France, etc.
Nigeria is the largest country in the continent of Africa; also by extension has the largest black population of people in the world with over 200 million people. The population of Nigeria stands at 200,964 million in mid-year population; projected to be 262,977 million in 2030; 401,315 million in 2050 and 732,942 million in 2100 respectively [46]. Obviously, the Nigerian population trends tend to be on the increase rapidly. Thus, Nigeria population becomes significantly important when it comes to discussing the issue of COVID-19 pandemic in the world especially in Africa.
Situation report of COVID-19 outbreak in Nigeria from 29th February, 2020 to 30th June, 2020 was examined to show its trends. A case of COVID-19 pandemic was first confirmed in Nigeria on 27th February 2020 in a 44-year-old Italian citizen in Lagos who then returned from Italy and was the first case to be reported in Nigeria since the outbreak of the virus in China. He was later referred to Infectious Disease Hospital, Yaba, Lagos and COVID-19 was confirmed on 27th February [47]. Since then, it has been a daily record of people who contract the disease. Meanwhile, Nigeria recorded the first death from the coronavirus pandemic on the 23rd of March 2020 [48].
Since the first case of confirmed coronavirus patient on 29th February, 2020 and the first recorded death on the 23rd March, 2020 to 30th June, 2020; cases of COVID-19 pandemic and deaths have been on the increase. Just within 3 months; 590 people have so far died from the virus [49]. Table 4 showed the situation updates of COVID-19 Pandemic in Nigeria as at 30th June, 2020.
Table 4: Situation updates of COVID-19 Pandemic in Nigeria as at June, 30, 2020. View Table 4
The distribution of the cases and fatalities of the virus cut across both rural and urban areas particularly in Nigeria. However, the daily report being given out by the Nigeria Centre for Disease Control/The Presidential Task Force on COVID-19 Pandemic currently seems the agency is more interested in reporting the cases and fatalities of each state without categorising it whether it is from rural or urban centres. However, due to larger concentration of many people in cities where there is higher level of social contacts; it is likely that the virus would be more prevalent in urban areas. In fact, the first confirmed case of the virus actually started in city - Lagos, Nigeria. Therefore, the cases are more prevalent in urban areas.
Thus, there is tendency that the virus will continue to spread widely; if people are yet to grasp the reality, seriousness and severity of the virus. Unfortunately, the virus has started having serious and negative impacts almost on every sector in the society [5]. Further stressed that the virus can potentially weaken health systems in many African countries including Nigeria particularly the primary healthcare due to poor health system.
Intentionally disregarding the formally prescribed preventive measures for COVID-19 pandemic probably dues to tenaciously holding on to some misconceptions about the virus may prevent many people from perceiving the virus as real, serious and life-threatening. Of course, there is tendency for its daily increases in cases and fatalities among people. In fact, the Presidential Task Force for COVID-19 Pandemic in Nigeria has suggested several times that intentionally disregarding or flouting the formally prescribed preventive measures for COVID-19 pandemic might have been responsible for its daily increases in cases and fatalities in the country. Therefore, increasing in the cases and fatalities without scientifically approved vaccines or drugs for its treatment at the moment may continue posing more challenges for humanity.
The COVID-19 pandemic across the world indicates a global threat [1]; also a global health threat [22]. It is a major public health concern for humankind causing more hospitalisation and death, particularly for people of middle and old age in the affected countries [1,12]. Obviously, it has become a clinical threat to people and healthcare workers worldwide [1]; as well as its serious effect on social and economic development [17]; with severe complications to humanity [25]; resulting in high morbidity, mortality and disruption of life [28] that requires a global response that would involve all countries [1] because of the major challenges it has posed all over the world [50].
Moreover, it is obvious that COVID-19 pandemic has the capacity to create more serious socio-economic and political problems for humanity [14]; seriously affecting the global economy [1]; including its health and security impacts on African continent [23]. It is believed that its impacts would affect both small and medium-size companies more sharply and the economies of some developing countries would suffer more [14]; making people losing jobs and income everyday with no sign of returning to normalcy [14]. The increasing in the cases and fatalities of the virus has affected socio-economic activities due to imposing physical distancing measure with strict compliance at different levels in many African countries [24].
Furthermore, the consequence of the virus has created social anxiety among families and households among African citizens. It is likely that most African countries will experience economic recession after COVID-19 pandemic because; many African countries heavily rely on petroleum products in terms of global supply chain [24]. In fact, the virus has been regarded as the most crucial global health disaster of the century facing humanity [1]; due to serious health, economic, environmental and social impacts it has created for humankind [1].
Thus, continuous restrictions on movements of people and total or partial lockdown in Nigeria as part of some prescribed preventive measures for instance will impose a significant economic burden on people wellbeing [51]. Also, staying in isolation for a long time might create severe and devastating economic impacts on people [17].
Also, the COVID-19 pandemic survivals might experience social stigma from the society [14]. Moreover, lack of proper awareness and fear of stigma could make people with suspected cases refuse to come out voluntarily to be tested [51]. Health workers in particular face some serious challenges such as both mental and physical stress thus leading to temporary separation from their families, also experiencing stigma and the pain of losing patient's and colleagues. Even, many of them have acquired the virus and some have lost their lives [23]; leading to a global health crisis, particularly to handle critically ill patients [52]. Moreover, the experience of psychological impacts such as the prevalence of insomnia, depression and posttraumatic stress symptoms among Nigerians during COVID-19 pandemic have been reported [53].
Moreover, depending on online lectures due to COVID-19 pandemic might raise serious challenges on the quality of education system at all levels. This is because; some teachers who are used to teaching live classes will need to engage in novel methods to achieve effective teaching outcomes, which may affect the quality of tertiary education. Also, students in remote and rural areas may not have the network capacity, thereby leading to a loss in educational opportunities [17]. Obviously, this is an indication of what is playing out in many African countries including Nigeria at the moment.
The rapid increase in the cases and fatalities of the virus is already affecting the critical healthcare services especially in African continent and Nigeria in particular [27]; infecting and killing many people without a possible vaccine or drug for its treatment at the moment [54]. However, older people with chronic cardiovascular-related diseases were more affected in a retrospective study [26]. It is very critical for people with any form of underlying illnesses. These categories of people are more susceptible to the virus. Moreover, dealing with this new virus is particularly challenging and requires complex decision making and leadership from the key stakeholders - government and medical leaders [28].
The role of human and financial resources and technological advancement through capacity building are crucial for how well countries with their health institutions will cope with the challenge of the virus [28]. Generally, African countries including Nigeria have weak economic and health systems and obviously make them more vulnerable to the negative impacts of the virus. The effects would be more serious; if the cases and fatalities of the virus continue rising [7]; without scientifically approved vaccines or drugs for its treatment.
There is no doubt that virtually the whole world is already in the midst of the virus especially in African continent and Nigeria in particular. The main focus of this study has been on the implications of some and documented misconceptions about COVID-19 pandemic in relation to its daily increase in cases and fatalities in Nigeria. Though, it is already having negative impacts on virtually every sector in the society such as health, economy, transportation-commerce, education, agriculture - food insecurity, family, religion, politics, security, sport activities, etc. This remains a serious concern for humankind at the moment.
Moreover, this study has documented some common misconceptions about COVID-19 pandemic among people in Nigeria. It is observed that many people still hold on to some of these misconceptions. Holding on to some of these misconceptions have actually made many people to openly disregard the prescribed preventive measures being put in place to contain the disease. Similarly, some studies have corroborated the documentation of some common misconceptions about the virus in this study [18-21,36]. Relatively, their findings/reports have lent credence to the fact that many people still hold tenaciously onto some of the common misconceptions being reported in this study though in various forms. Their studies cut across both rural and urban areas.
However, some of these studies particularly in Nigeria were not peer reviewed and were online surveys. That is, the studies were not certified by peer review process as authors reported [18-20] but then their findings (especially the three reports from Nigeria) are a clear indication that misconceptions about the virus are still prevalent in the country. It is likely that sustaining or continuing with this type of belief-systems during the COVID-19 pandemic period will go a long way in creating more harms than benefits for humanity. Though, some of these misconceptions have been proved to be false [14,21,36] but many people still feel reluctant to change their belief-systems about the virus.
On the other hands, some studies have also reported on knowledge level of people regarding the virus in Nigeria and in other countries. The works of [38] and [20] from Nigeria have equally rated Nigerian people as having high knowledge about the virus with Television, Radio, internet/social media as their main sources of information respectively. Similarly, other findings from Malaysia, Pakistan, USA/UK, and Italy have also reported good knowledge and practices about COVID-19 pandemic among their participants [23,29,39,40]. A contrary study from Ethiopia among patients suffering from chronic disease showed their participants had poor knowledge and practice about COVID-19 pandemic [12].
Moreover, some of the studies particularly from Nigeria have ranked Nigerian people as having high knowledge about the virus. This is encouraging and possible to some extent. But then, many people still hold on to some of the common misconceptions about COVID-19 pandemic in the country. However, having high knowledge about a particular issue through any medium may not necessarily influence or change people's belief-systems and behaviours if not convinced. So, having knowledge alone may not totally bring about the desired positive behaviours - strict compliance with all the prescribed preventive measures. It is apparent that the acclaimed knowledge about the virus does not translate into changing their health behavioural patterns particularly in the country. Other factors may as well play crucial role, such as socio-economic, socio-cultural factors, geographical location, etc.
Furthermore, the global report of COVID-19 Pandemic in Table 1 above shows the first cases of coronavirus from 31st December, 2019 to 20th January, 2020 [42]. While the first cases of deaths from coronavirus disease were reported on 22nd January, 2020 with six deaths from Wuhan [43]. Since then, thousands of cases and fatalities from COVID-19 pandemic have been reported daily across the world including African continent and Nigeria in particular. The trends of the virus in Figure 1 from 30th December, 2019 to 30 June, 2020 [44] have been rising steadily but it appears the curve is coming down gradually in late June 2020.
In African region, the first cases were reported in Algeria on 25th February 2020, since then the virus has continued to increase in cases and fatalities [45]. Likewise, in Figure 2 and Table 3 [45], the trends of the virus in the region from 25th February to 23rd June 2020 have been on the increase. It ranked Nigeria the second after South Africa in the continent with highest cases of COVID-19 pandemic [45]. The rate at which the virus is spreading and rising in African continent is quite alarming though unlike the more developed countries such as the USA, UK, etc.
The situation in Nigeria is not quite different from other countries in African continent in terms of COVID-19 pandemic; with its first reported case on 27th February 2020 [47]. Since then, it has been a daily record of people who contract the disease. Meanwhile, Nigeria recorded the first death from the coronavirus pandemic on the 23rd of March 2020 [48]. As at 30th of June 2020 in Table 4, just within 3 months; many people have lost their lives so far from the virus [49] and an end to COVID-19 pandemic is not certain at the moment [17]. However, increase in trends of the virus cases in the world could be due to lack of proper preventive measure [26]. This might not be too far from the reality.
The hierarchical discussion of this study from the global level to African continent and Nigeria in particular is necessary to show the trends of the virus in the society based on some official data. It is obvious from the available data (information) on COVID-19 pandemic stated above which cuts across the world, African continent and Nigeria in particular that continuously increase in cases and human fatalities of the virus without curable vaccines or drugs at the moment may create further problems for the entire society. Likewise, tenaciously holding on to some misconceptions about the virus especially in African continent and Nigeria in particular may prevent many people from perceiving the virus as real, serious and life-threatening. Obviously, there is tendency that the virus will continue to spread widely; if people are yet to grasp the reality, seriousness and severity of the virus.
Unfortunately, the virus has started having serious and negative impacts almost on every sector in the society. The implications are enormous cutting across all sectors in the society which include: Economy; religion; education; agriculture - food insecurity; transportation - commerce; health; security; family; sport activities etc. to mention a few. There is no doubt that the virus has badly affected many people. Nigeria is no exception; thus creating devastating social, economic and political problems as a result [1,14,17,51]; raising serious challenges on the quality of education system and educational opportunities at all levels [17]; including the health sector [23,27,52]. If caution is not taken; African countries would go into unavoidable recession after COVID-19 pandemic [24].
From the Nigerian perspective, the inter-state movement ban on people has had negative impacts on the economy, transportation and commercial activities in the country. Many people have been laid off of their jobs by their employers because of the inability to make profits and pay wages or salaries. Gathering together of large people in the worshipping places has been hindered due to COVID-19 pandemic thus creating negative effects on religious activities including entertainment activities. Agricultural activities are also affected almost leading to food insecurity in the country. Health sector is not left out due to daily increases in the cases of the virus. Health sector is becoming overstretched at the moment. The banning on schools at all levels has seriously affected the educational sector. Students at all levels have not been able to attend classes for sometimes due to the virus. Also, COVID-19 pandemic has some negative impacts on security. There is an increase in the cases of criminal activities in the country - raping, kidnapping, army robbery attack, fraudulent activities, etc. The family structure is also affected. Many people finding it difficult to cater for their families thus leading to domestic violence. These are the clear manifestations of the negative impacts of the virus on people in the country.
Obviously, these negative effects have caused some psychological impacts - the prevalence of insomnia, depression and posttraumatic stress symptoms among Nigerians during COVID-19 pandemic [53]; including mental and physical stress among health practitioners thus leading to temporary separation from families, stigma and the pain of losing patient's and colleagues [23]. The survivals might experience social stigma from the society [14]; fear of being stigmatised could have prevented people with suspected cases of the virus from coming out voluntarily for testing [51]. In many cases, this is what is playing out in the country.
It is believed that continuously holding on to some of these common misconceptions about the virus among many people might have been responsible for daily increases in the cases of the virus. This is because; often times many people deliberately flout the formally prescribed preventive measures being put in place. Moreover, the daily increase in the cases and fatalities due to COVID-19 pandemic in Nigeria has continued to baffle the key stakeholders especially the government at all levels. However, government is aware that the total or partial lockdown in some states in order to prevent the widespread of the virus has almost crippled the economy and its negative effects on people well-being in the country.
Similarly, people are not comfortable with the negative effects the preventive measures being put in place due to the virus have had on their jobs/works, businesses, family life and social relations. But then, people should not misuse the opportunity of gradual relaxation of some of these preventive measures to what people can easily adhere to such as compulsory wearing of face mask in public places; maintaining physical distancing of at least 2 metre apart from other people; etc. If the cases and fatalities of the virus continue rising; its effects would be more serious [7]; without scientifically approved vaccines or drugs for its treatment at the moment.
Therefore, re-strategising the officially preventive measures being put in place by the stakeholders becomes imperative. With strict enforcement of the measures. There is an urgent need for total behavioural changes in people' attitudes and belief-systems to uptake the "new normal" - the currently intended or desired behaviours in the society. Thus, concerted efforts should be put in place in order to achieve it. People must be made to understand or realize the importance of these intended behaviours (the preventive measures) for COVID-19 pandemic containment in the society. Intentionally disregarding the formally prescribed preventive measures for COVID-19 pandemic among people should not be tolerated and be totally discouraged and frowned at.
However, the formally preventive measures are simply the personal efforts and responsibilities required of an individual person to follow but need to be strictly enforced by the authority for maximum compliance. So, whoever tends to flout the prescribed measures should be strictly punished. It is also important for both parties - the stakeholders (government at all levels, NGOs, corporate bodies, etc.) and the citizens to carry out their responsibilities. Apart from strictly enforcing the prescribed preventive measures; government at all levels should be more responsible in providing adequate social supports (both short and medium-term palliative measures) for people.
Moreover, the role of the recovered victims (patients) of COVID-19 pandemic is paramount to openly share their ordeal and experience about the virus to people and how they survived it. That is, the COVID-19 pandemic survivals. They should be encouraged without feeling stigmatised to come out voluntarily in large numbers to be part of the stakeholders. Thus, this strategy can be another way of positively influencing behavioural patterns of people to take ownership of their health-related behaviours.
Both government at all levels and the citizens are expected to change their behavioural patterns towards the virus [55] whereby well-informed messages could be packaged about COVID-19 pandemic in order to minimise its widespread [37]; changing in perceptions, beliefs, values and human understanding becomes crucial [14]. Also, the collaborative effort of countries in African continent to tackle the increasingly widespread of the virus will promote public health capacity building, training and research [56]. Indeed, this is a welcome development.
It is therefore more crucial that vigorous attempts to change the narrative of some misconceptions about the virus in the continent and particularly in Nigeria should remain a top priority in their agenda. Pending when the scientifically, medically and clinically proven vaccines or drugs for its treatment has been finally discovered in the world. However, without positive behavioural changes in people' belief-systems and attitudes to completely dismiss some of the common misconceptions about the virus; their concerted efforts may prove futile.
This study has been able to examine and document the implications of some common misconceptions about COVID-19 pandemic in relation to its daily increase in cases and fatalities in Nigeria and its negative effects on people well-being. This study has extended the frontiers of knowledge about the virus and actually contributed to the already existing body of knowledge on COVID-19 pandemic in the world particularly from Nigerian perspective. However, the study relied on neighbourhood views (opinions) about the disease. Though the suggestion that the continuous holding on to some common misconceptions about the virus is responsible for its daily increase in the cases and fatalities among people have not been statistically proved in this study as the main cause. Further studies can be conducted in the research area to significantly determine other factors that are primarily responsible for its daily increase in cases and death rates in Nigeria.
Holding on continuously to some common misconceptions about coronavirus disease (COVID-19) pandemic among people has been suggested to be largely responsible for the daily increase in cases of COVID-19 pandemic and its fatalities particularly in Nigeria. This rapid increase in cases and fatalities of the virus has already been having serious negative effects on people jobs/works, businesses, family life, social relations and the economy of the country. There is need for positive change in people' belief-systems and health-related behaviours about the virus. This will be through effective and active public enlightenment and awareness creation by the major stakeholders - government at all levels with strict compliance with the prescribed measures for the virus. Therefore, concerted efforts of the stakeholders at all levels to change this narrative of misconceptions among people become significant. This will go a long way in influencing positive health-related behaviours among people, getting rid of some misconceptions about the disease that may trigger larger community transmissions as the efforts to discover new vaccines or drugs for COVID-19 pandemic treatment continue.
None.
All the health practitioners and researchers who are working tirelessly to contain COVID-19 Pandemic in the world.
Not applicable.