River blindness is a skin, and an eye disease caused by Onchocerca volvulus and vectored by a female hematophagous blackfly. The study aims to evaluate the distribution of the clinical signs of river blindness and the efficacy of Ivermectin in the treatment of river blindness in Idogun. Observational studies in epidemiology which involve the use of structured questionnaire to obtain useful epidemiological information from the respondents, physical assessment via palpation from head to ankle was used to assess clinical signs from the respondents and skin snip test was used to evaluate the prevalence of the disease. The efficacy of the drug was evaluated and express in percentages. Of the 384 respondent examined, only 192 of them showed various signs of river blindness However, it was only 108 (28.1%) respondents with the signs that demonstrated O. volvulus microfilariae in their excised skin snips. The clinical signs observed among the respondents include: Skin depigmentation such as dermatitis, leopard skin, papules, pruritus and self-inflicted injury while ocular signs include cataract, ocular lesion and partial blindness. Among these clinical signs, papules, and pruritus were the most dominant in the community. Prevalence of the clinical signs was observed to vary significantly among the age groups and gender (P < 0.05). The efficacy of the drug after 6 and 12 months of treatments shows that the drug was more effective at age groups 10-50 years than the age groups 51-90 years. Ivermectin was observed to be efficacious in the treatment of the disease. However, to achieve eradication of the disease, the drug may be administered at 0.15 mg/kg twice a year.
River blindness, Clinical signs, Ivermectin, Idogun
River blindness is a leading cause of preventable blindness and a severe pruritic skin condition in endemic areas. The disease is caused by filarial worm (Onchocerca volvulus) and transmitted by Female blackfly (Simulium spp). River blindness is the cause of clinical and epidemiological burden of skin disease in Africa [1]. An estimated 40 million people are at risk of the infection worldwide with about 2 million at risk of being blind. The disease is endemic in 28 countries in Africa, 6 countries in the Americas and in Yemen. Some 18 million people are estimated to be carrying the infection worldwide with over 99% of them living in Africa [2]. In Africa, hyper endemic villages can have infection rate of about 100% while 10% of the entire village may be blind, including up to 50% of those aged 40 years and above [1]. In West Africa, blindness is more commonly reported in the savannah and woodland areas, whereas depigmented skin disorders are more frequent among the forests dwellers. Forty percent (40%) of all cases of onchocerciasis occur in Nigeria with more than 32 million Nigerians estimated to be at risk of the disease [1]. It has been estimated that of the 15 million people infected with Onchocerca volvulus and living in endemic countries outside the onchocerciasis control program, 6.4 million live where parasite strains are relatively pathogenic to the eye. 8.6 millions reside where forest strains cause severe skin disease but less eye disease than savannah strains [3].
The clinical symptoms seen in human onchocerciasis are as a result of the developmental stages of the parasite (Onchocerca volvulus) and the inflammatory responses produced by the host to the parasite. These symptoms vary from host to host and from one geographical region to another. The symptoms do not manifest in the host until the third larval stage of the parasite (microfilaria) matures into an adult worm [1]. Hence, the symptoms appear in the infected host between 9 months to 2 years after initial blackfly bite. The clinical signs of river blindness are as a result of the interaction of the drug with the microfilarial stage of the parasite which results in tissue inflammation and damage [4]. Formation of papules in the skin is caused by the conglomerate of adult worms found in subcutaneous nodules (onchocercomata) which results to different dermal and epidermal pathologies. These pathologies are complicated by a self-inflicted trauma which arises from the intense pruritic nature of the infection.
River blindness is best known for its eye infection which can affect many parts of the eye, sometimes leading to an irreversible damage and complete blindness. Another factor that could play major role in the development of the pathology and clinical signs of the disease, is the obligatory endosymbiotic bacterium Wolbachia, which is always abundant in all the developmental stages of the O. volvulus [5-7]. Usually, clinical symptoms are not present during prepatent period (period between infection with infective larvae and the production of microfilariae by fertilized worms). The prepatent period for onchocerciasis varies from 7 months to more than 2 years [8]. The time from invasion by infective larvae to the development of clinical signs (incubation period) is usually longer than the prepatent period and may last for many years; it is longer for the manifestation of the ocular disease than the dermal presentations [9]. The study aims to assess the clinical manifestations of onchocerciasis among the age groups and gender and evaluate the efficacy of Ivermectin in the treatment of Onchocerciasis in Idogun community of Ondo State.
The study was conducted from January to December 2016 in Idogun; an endemic community for onchocerciasis in Ose Local Government Area of Ondo State, Nigeria. Idogun community has a land area of 1,465 km2 and a population of 144,901 [10]. The community predominantly consists of Yoruba ethnic group; other ethnic groups include: Igbira, Hausa, Igbo and Fulani. The major economic activities in the community are farming, hunting, trading, artisans and civil services. The community also consists of two main seasons: A rainy season (April-October) and dry season (November-March).
Prior to the commencement of the research, approvals for the study were obtained from the disease control of the Ondo State Ministry of Health, Primary Health Coordinator in Ose Local Government Areas (OSHREC/22/01/2016/090) and community head. Similarly, informed consent of the respondents was obtained after focus group discussion in a native language where the subjects were made to know the advantages and disadvantages of their participation in the study.
Demographic information such as age and gender was obtained from the respondents using structured questionnaire. Also, respondents were palpated and examined clinically from head to the ankles for dermal and ocular symptoms of onchocerciasis such as leopard and lizard skin, darkened skin, scratch marks, papular skin rash signs of acute onchodermatitis [11]. A slit-lamp was used to examine ocular symptoms such as eye lesion and cataract. The respondents were physically examined for the presence or absence of the following clinical symptoms using the method of Basile, et al. [12]:
Nodule assessment (subcutaneous nodules or bumps on skin): Each subject was palpated from head to toe using both hands with gloves with special attention to rib cage, iliac crest, greater trochanters, knees and scapular for nodules.
Leopard skin/depigmentation (patchy skin depigmentation) assessment: This clinical feature was assessed by examining the lower limb for the presence or absence of the depigmentation on the skin.
Degree of pruritus (body itching): This was physically confirmed from the subjects and recorded as present or absent.
Excoriation (self-inflicted scratch marks): The trunks, buttocks and lower limbs of the respondents were examined for these obvious self-inflicted scratch marks as described by Basile, et al. [12].
Bloodless skin snips were aseptically collected from the iliac crests of the respondents who presented with palpable nodules using sterile blood lancet and razor. The snips were immediately placed in 0.5 ml normal saline in a microtitre plates and left for 4 hours to allow the microfilariae to migrate out of the tissues. The solution was centrifuged at 2000 rpm for 15 mins, the sediment was smeared on sterile slides and stained with Giemsa at pH 6.8. The smears were examined for microfilariae under X40 objective lens of a microscope. Number of snips positive for the microfilariae was noted among the age groups and genders.
The ivermectin which is the drug of choice for onchocerciasis was administered to the respondents who had never taken the drug before. The individuals for the test were clinically examined for papules and skin snips were taken from them. The skin snips were examined under the microscope to establish infection. The weights of the individuals were taken with the aid of weighing balance and the drug was administered orally using WHO approved standard [4]. The standard informed that 0.15 mg/kg should be administered twice a year and each dose of the drug weighed 3 g. Hence the average dose per body weight was calculated using the below formula:
The efficacy of ivermectin was determined by comparing the prevalence of infection before and after treatment divided by the prevalence before treatment multiply by 100 i.e
Data obtained from the questionnaires, physical examination and laboratory diagnosis were subjected to Chi-square, t-test and One-Way ANOVA analyses using Statistical Package for Social Sciences (SPSS) version 21.0.
Various degrees of clinical symptoms as observed in this community range from a cataract to self-inflicted injuries (Figure 1). Of the 384 respondents that were clinically examined for dermal and ocular manifestations of the disease, 192 of them showed various degrees of these symptoms. Cataract was absent among the respondents while dermatitis was absent only in age groups 10-40 years. Likewise, leopard skin and lizard skin were absent in age group 10-30 years. Partial blindness which is an ocular manifestation of the disease was only found among the age group 51-60 years. Self-inflicted injuries were found to be common among age group 21-40 years. Papules and pruritus were the most dominant clinical symptoms as they were found in all the age groups but pruritus had the highest percentage occurrence in the community. It was generally observed that prevalence of clinical symptoms varied significantly among age groups (p < 0.05). This was evident in Figure 2 where the prevalence increases from 11-40% as the age increases from 10-60 years and later decreases above 60 years. Noteworthy in the study is age group 51-60 years with the highest percentage of clinical symptoms (40%). It was also observed that not all patients with clinical symptoms were positive to skin snip test. This was demonstrated in this community; out of 192 respondents with the clinical symptoms only 108 respondents were positive to the skin snip test.
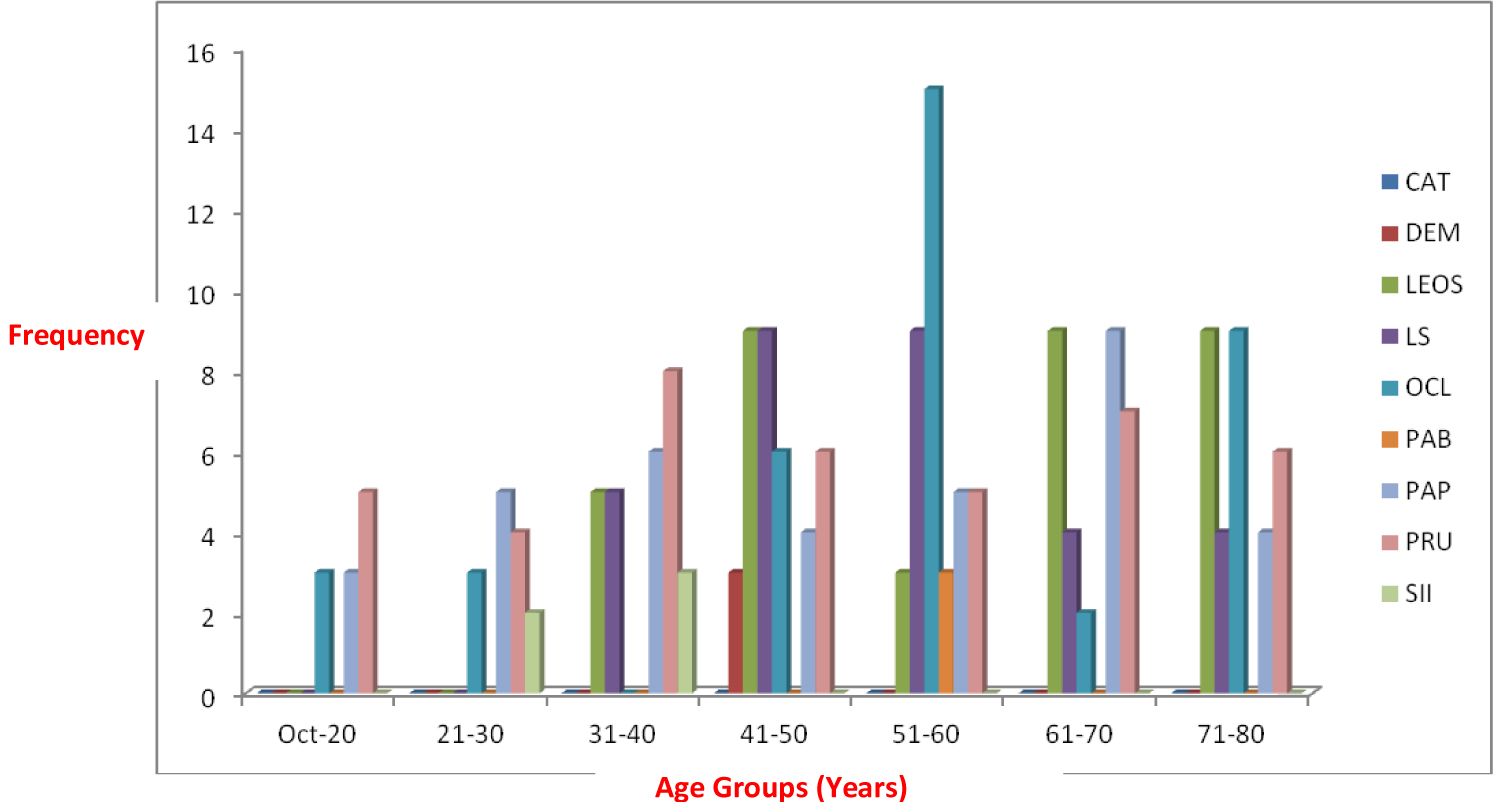 Figure 1: Clinical symptoms of onchocerciasis among the people of idogun community.
Figure 1: Clinical symptoms of onchocerciasis among the people of idogun community.
Keys: CAT: Respondents with Cataract; DEM: Respondents with Dermatitis; LEOS: Respondents with Leopard; Skin LS: Respondents with Lizard Skin; OCL: Respondents with Ocular Lesion; PAB: Respondent with Partial Blindness; PAP: Respondents with Papules; PRU: Respondents with Pruritus; SII: Respondents with Self-Inflicted Injury.
View Figure 1
Prevalence of the clinical symptoms was also significantly different between genders (p < 0.05). The percentages of all the clinical symptoms with the exception of ocular lesion were higher in males than the females (Figure 2).
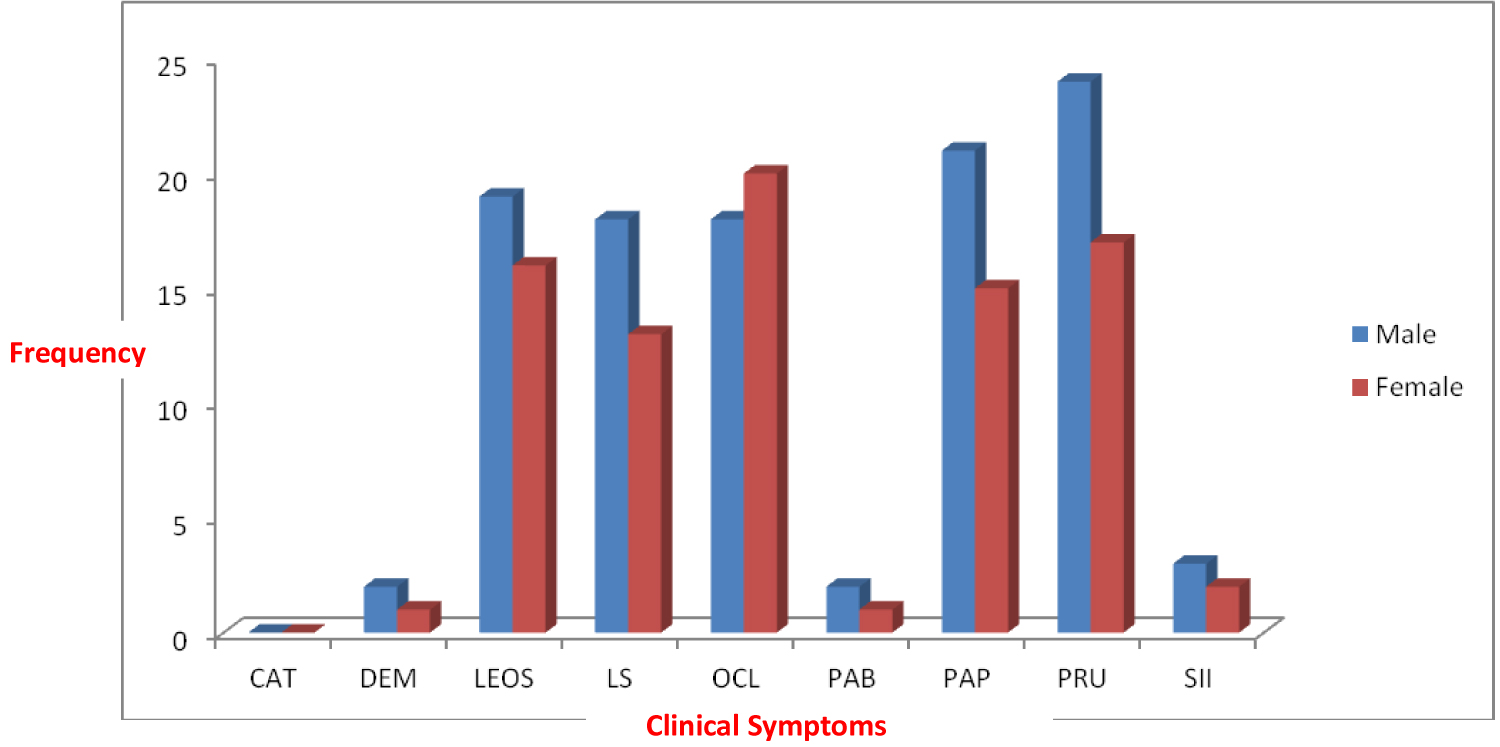 Figure 2: Clinical symptoms of onchocerciasis between sex distribution in idogun community.
View Figure 2
Figure 2: Clinical symptoms of onchocerciasis between sex distribution in idogun community.
View Figure 2
The skin snips aseptically collected from 384 respondents revealed that 192 of the respondents showed varying degrees of clinical symptoms of onchocerciasis while 192 showed no clinical symptom. The clinical symptoms were observed to vary significantly among the respondents (T = 4.518; P = 0.001; P < 0.05); However, it was only 108 respondents with the clinical symptoms that were positive to skin snip test for the O. volvulus microfilariae; Furthermore, skin snips collected from respondents with dermatitis, pruritus and self-inflicted injury showed prevalence of 33.3%, 31.7% and 40% respectively (Table 1). Skin snips obtained from respondents in the community with depigmentation of skin such as leopard skin and lizard skin showed 54.3% and 80.6% prevalence respectively. Meanwhile, skin snip from respondents with ocular lesion and papules recorded prevalence of 52.6% and 69.4% respectively. No prevalence was recorded in this community for respondents with cataract and those that manifested no clinical symptoms. The highest prevalence (100%) was obtained in the skin snips of the respondents with partial blindness (Table 1).
Table 1: Prevalence of Onchocerciasis among the Respondents with Clinical Symptoms in Idogun Community. View Table 1
The efficacy of ivermectin among the study group showed that the efficacies of the drug varied significantly among the respondents in Idogun (F = 18.000; P = 0.000; P < 0.05). The drug was observed to be more effective at age groups 10-50 years than the age groups 51-90 years. As observed from Table 2, the highest efficacy (33.5%) after 6 month treatment was recorded in age group 31-40 years while the lowest efficacy (0%) was recorded in age group 71-80 years. Generally, increase in drug efficacy with varying degrees was observed among the age groups after 12 months treatment. Efficacy after 12 months treatment showed that age group 21-30 years had the highest efficacy (87.5%) while the lowest efficacy (16.5%) was observed in age group 71-80 years. Age group 81-90 years was not considered in the efficacy test because all the individuals in this age group were negative to the infection.
Table 2: The Efficacy of Ivermectin among the Respondents in Idogun Community. View Table 2
The results of the study reveal two categories of the clinical manifestations: Dermal and ocular manifestations. The dermal manifestations observed in the community include dermatitis, leopard and lizard skin, papules, pruritus and self-inflicted injury while the ocular manifestations include cataract, ocular lesion and partial blindness. Pruritus/itching also known in the community as 'inarun' (fire from heaven) and 'kuruna' (craw-craw) has been found to be the most distressing clinical symptoms in Idogun community. The local names given to the disease is not peculiar to this community, other endemic areas have also attributed their local names to the itching caused by the disease. For instance, the disease is known in Ghana as 'ahokeka' (body itch), in Uganda as 'ayila yila' meaning persistent itching [14], 'mara' (skin itching) and 'roto' (little frog) in Sierra Leone [15]. However, it was observed that the prevalence of onchocerciasis in the study community was higher among the respondents with partial blindness, lizard skin and papules than the respondents with pruritus and self-inflicted injury. It was also noted that partial blindness and lizard skin were clinical manifestations that were observed in subjects after a long period of exposure to the infection and consequently manifest at older age groups among the study population. This finding is supported by the report of Fox [16] and Diemert [17] which observed in their various studies that blindness and depigmentations are clinical symptoms that manifested at older age groups. Similarly, higher prevalence was recorded among respondents with papules which are dermal manifestations that resulted from the inflammatory response of the host to the parasite or the effect of the drug (ivermectin) on the microfilariae of Onchocerca volvulus.
It was further observed from the study that the clinical symptoms of the disease peaked at age 51-60 years, this concur with the reports of Adewole and Ayeni [18] in Ise-Orun Local Government, Ekiti who observed peak prevalence of onchocerciasis among age group 56 and above. Meanwhile, the report of the study was slightly contrary to the reports of other authors [19,20]. Both authors in their separate researches reported that the peak period of onchocerciasis is at 41-50 years of age. In addition, most dermal symptoms observed among the study group manifested in the respondents with lower age groups although these symptoms persist to higher age groups. In contrary, the ocular symptoms of the disease manifest as the patients advance in age without any effective treatment. This suggests that cutaneous symptoms are dermatological changes which manifest in the patients years before the onset of ocular symptoms [16,17].
The study further shows that the clinical symptoms of the disease were more among the males than the female gender. This implies that the males are more exposed to the blackfly bites than the females, this is because the male gender especially the older age group engages more in socio-economic activities such as farming, lumbering, fishing, hunting etc. This suggests that the males are more exposed to the blackfly bite more than the females, as the males engage in socio-economic activities such as farming and hunting as noted in the community than their female counterpart. These activities predisposed them to the infection than the females. This result on gender was supported by the work of Adewole and Ayeni [18].
Noteworthy in the study is the three records of partial blindness which were found among the two male genders and one female gender. This also buttresses the fact that partial blindness resulted in patients with high frequency of exposure to the blackfly bites and high microfilarial load (intensity) in the host.
The study revealed that the efficacy of the drug was significantly different among the age groups (p < 0.05). The drug was found to produce significant effects among the age group 10-50 years than the age group 51-90 years in the community at 6 months and 12 months post-treatments. These differences might be as a result of increase in microfilarial load (intensity) as the infected individuals advanced in age without treatment. The total efficacy as observed after 6 and 12 months post treatment in Idogun are 10% and 38.8% respectively. This suggests that for the microfilariae to be completely eliminated from the infected persons the drug must be taking continuously for many years.
The study identified age groups 51-60 years as age group that is more susceptible to onchocerciasis. Hence, it is suggested that in community directed treatment with ivermectin (CDTI) this age group should be given more attention. Furthermore, the three respondents with partial blindness also belong to this age group buttress the fact that the older age groups in endemic areas have higher chance of manifesting the ocular manifestations than the younger age groups. Therefore, there is need for more public sensitization among this age group especially those with the clinical symptoms informing them of the need to consistently take the drug in order to avoid permanent blindness. The study further suggests that lizard skin and partial blindness could be used in rapid diagnosis of the disease in endemic areas as papules from individuals with these clinical symptoms showed more than 75% prevalence compared to other clinical symptoms. The low efficacy of the drug observed across the age groups at six month post treatment suggests that the drug has a slow rate of eliminating the microfilariae and hence the drug should be taken twice a year and consistently for many years to further reduce the morbidity of onchocerciasis and prevent blindness in the endemic areas. Therefore consistent monitoring of the drug distribution in the endemic areas should be intensified to ensure that the infected individuals use the drug (Ivermectin) twice in a year.
The author declares no conflicting interest for this study.
The author is grateful to the King of Idogun, Chief Ajileye, the chairman, Public Health Committee and Mrs. Adelakun the Public Health Coordinator in Idogun for their support towards the successful execution of the study.