The novel coronavirus (COVID-19) has been a major public health trait across the world since its first emergence in Wuhan, China in 29th December 2019. The fact that the disease is new little has been known about the virus and factors contributing to the fast spread of the virus. WHO recommendations to control the spread of the virus are universal and needs contextualization further analysis of contributing factors at country level. Hence, countries across the globe implemented different controlling strategies to reduce the number of people infected by the virus. However, the virus has been spreading rapidly in an alarming rate across the globe. Ethiopia is among the countries where the virus has been spreading very fast. The government of Ethiopia declared a 5-month State of Emergency in an effort to limit the spread of the coronavirus (COVID-19) on 14th April 2020, however, the virus has been spreading in all regions of the country. In this review, factors that might contribute the spread of the novel coronavirus directly or indirectly in Ethiopia were analysed. These factors are poor knowledge and practice of the hygienic condition of the public during service delivery, day to day personal activities, socioeconomic nature of the society, political instability and the knowledge, attitude and practice of HCWs are mentioned. Strong intervention measures should be taken to mitigate the contributing factors that are tremendously important to control the spread of the novel coronavirus in the country. In addition, research should be conducted to know the level of impact of each contributing factor in Ethiopia.
Corona virus, COVID-19, Ethiopia, Pandemic
The emergence and fast spread of the deadly novel coronavirus (COVID-19) nowadays has become an alarming tone for all human kind across the globe to check its life style and forced to follow a new way of life that probably reduce the spread of infectious agents. There are numerous factors contributing to the spread of infectious agents in any country across a globe [1-3]. This might be associated with the geographical location, the socioeconomic status of the society, the level of awareness of the society and the health system of the country to combat emerging and re-emerging diseases and other related factors.
Development of effective herd immunity limits the spread of disease indirectly, which is conferred by immune to susceptible individuals in a given population. However, the development of effective herd immunity against the novel coronavirus depends on numerous factors and these factors are very difficult to be achieved in all environmental settings. The factors that hamper the development of effective herd immunity against of SARS-CoV-2 was well described by Papachristodoulou and his friends and concluded that long term natural immunity to SARS-CoV-2 is ambiguous, herd immunity may depend on effective vaccination. To this end, the urgent development of an effective vaccine tremendously crucial to control the pandemic [4].
The outbreak of endemic and pandemic emerging and re-emerging infectious diseases in any country in most cases occurred without preparedness and development of strategies to control the disease. The lack of preparedness to combat the outbreak along with the low understanding of the causative agent makes the problem more complex and difficult to treat.
It is evident that there is no approved drug that completely cures the novel coronavirus, although Dexamethasone has been used in many countries across the globe to treat ventilated COVID-19 patients. On the other hand, there is controversy regarding the potential antiviral activity of Chloroquine and Hydroxychloroquine (HCQ) against the novel coronavirus (COVID-19) infection and comprehensive studies that encompass large clinical trials should be conducted to assess the efficacy and safety of antimalarial treatments in patients with COVID-19. Otherwise, the mere recommendation and implementation of these drugs to treat COVID-19 patients may lead to unintended results [5].
The first emergence and outbreak of the newly emerged novel coronavirus in Wuhan, China in December 29, 2019 caused deaths of many peoples in the world. The virus is spreading very quickly in almost every country across the globe, infecting more than 22,639,650 peoples and caused 792,197 deaths at the time of writing [6].
The first coronavirus (COVID-19) case was reported in Ethiopia on 13 March, 2020 and the victim later identified was a 48-year-old Japanese citizen who came to the country from Burkina Faso a week earlier. Since then, the virus infected more than 34,058 peoples and caused 600 deaths till the time of writing. As the global trend shows the virus has been spreading quickly and predicted to affect many citizens of the country (Figure 1). According the report of the Ethiopian ministry of health the virus has been spreading in all regions of Ethiopia and will continue to spread unless strong implementation of controlling measures are implemented [7].
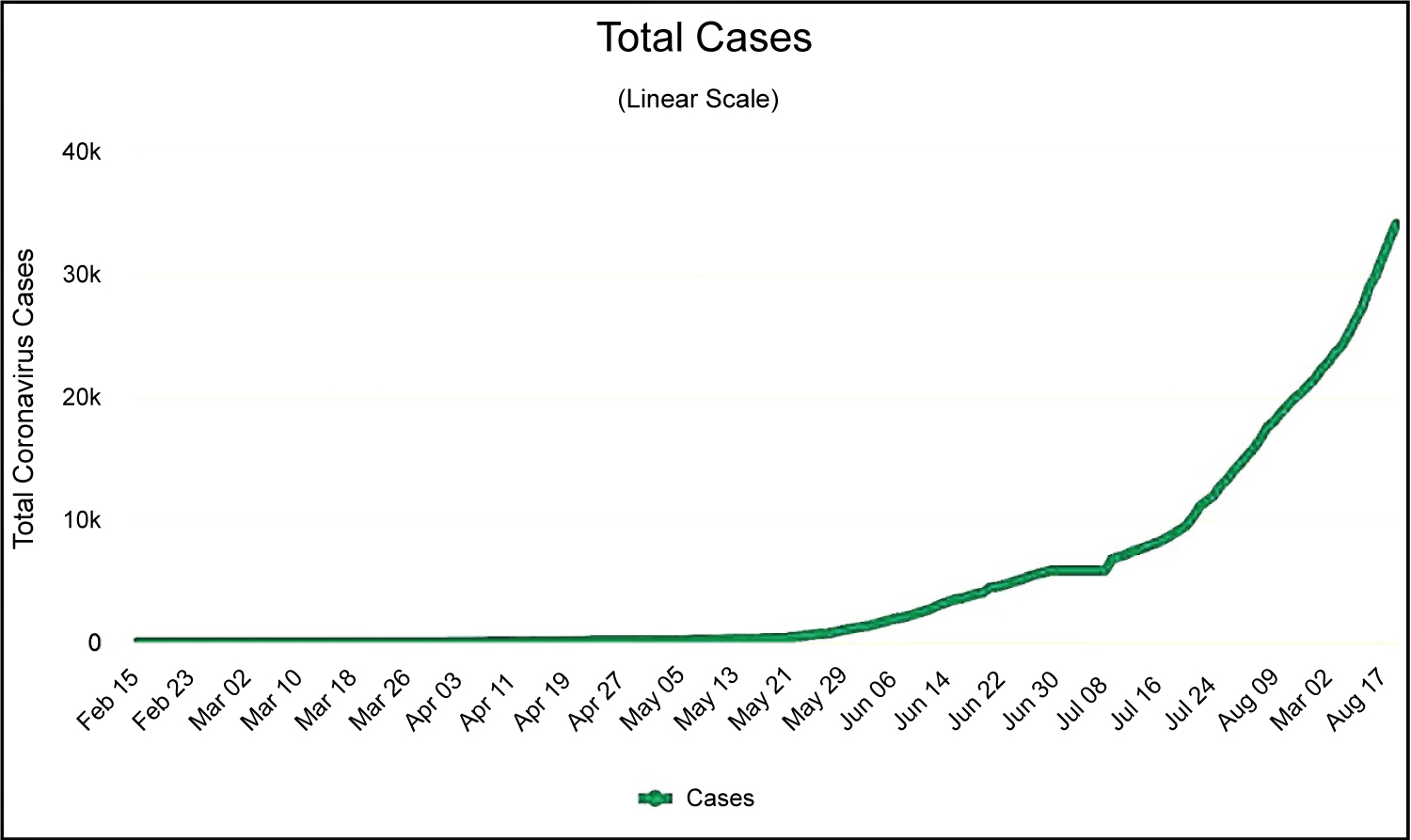 Figure 1: Total Novel Coronavirus (COVID-19) Cases in Ethiopia up to July 27, 2020. Source: https://www.worldometers.info/coronavirus/
View Figure 1
Figure 1: Total Novel Coronavirus (COVID-19) Cases in Ethiopia up to July 27, 2020. Source: https://www.worldometers.info/coronavirus/
View Figure 1
As a global trend shows, the rate of transmission of the novel coronavirus is high in and out of health institution in the community. The routes of transmission are many and many have also been under investigation. The significant high transmission rate of COVID-19, absence curative medicine and vaccine with significant total deaths it caused makes all countries across the globe to shift their primary agenda toward controlling the pandemic. Most of the countries across the globe devised possible prevention methods and have been implementing since WHO declared the virus as a pandemic. The earlier the implementation of the preventive strategies of COVID-19 of the countries, the less spread of the virus with lower total deaths in many countries has been observed [6].
The preventive strategies implemented vary from country to country except the common ones. In Ethiopia, the government has been implementing various preventive strategies [8]. Among the various preventive strategies, awareness creation of the public regarding personal protection, identification and banning/closing/of potential risk areas and others have been implemented. Although the potential risk factors so far identified and intervened by the government are the common preventive methods implemented by many countries across the globe, it is quite important to identify other probable contributing factors that might easily contribute spread of the virus and other infectious agents contextually based on the nature and life style of peoples in a given area. In this view, hypothesizing possible contributing risk factors for the spread of COVID-19 in Ethiopia context is tremendously important in the journey of controlling the pandemic. To this end, the main objective of this review is to analyse the potential possible risk factors that might be associated with the fast spread of the novel coronavirus in Ethiopia.
Ethiopia is a developing country in East Africa and a home of greater than 114,963,588 million peoples (2019) belongs to more than 80 ethnic groups. Ethiopia is the 2nd most populous country in Africa next to Nigeria and the 12th from the world [9]. The 2019 population density in Ethiopia is 115 people per Km2 (298 people per mi2). Ethiopia is a landlocked country with total land area of 1,000,000 Km2 (386,102 sq. miles), and bordered by Sudan and South Sudan on the west, Eritrea on the north, Djibouti and Somalia on the east, and Kenya on the south. The current Birth rate is 31.467 births/1,000 population and death rate is 6.395 deaths/1,000 population and population growth rate is about 2.57% in 2020. The majority of the Ethiopian population lives in scattered rural communities and depends on agriculture as their daily livelihood, only 21.3% of the population (2020) live in urban areas [9]. Ethiopia has a federal system of government comprising 10 regions (Afar, Amhara, Benishangul-Gumuz, Gambella, Harai, Oromiya, Sidama, SNNPRR (Southern Nations, Nationalities and People's Region), Somali and Tigray) and two city administrations (Addis Ababa and Dire Dawa). The regions are divided into zones, which are then broken up into Woredas in rural areas, or sub-city administrations, and Kebeles at the village level. The Woredas are key local government units in each region and are responsible for the provision of basic services [10]. According to World Bank report, Ethiopia is the fastest growing economy in Africa but also one of the poorest, with a per capita income of $790. Ethiopia goals to reach lower-middle-income country status by 2025. Ethiopia unemployment rate for 2019 was 2.08% and specifically, youth unemployment rate for 2019 was 3.23%. Like other developing countries, due to the poor economy of the nation the level of service delivered to the public are generally poor and the life quality of the majority of citizens is compromised. The poor living style of the citizen exposes the public to unhealthy life and exposure to infectious diseases. So far, different factors associated with the spread of different infectious agents were identified by different scholars. These factors are associated with the nature, habit, socioeconomic status of the peoples and some of these were presented.
Street-vended foods are defined as foods and beverages prepared and/or sold by vendors in the streets and other public places for immediate consumption or consumption at a later time without further processing or preparation [11]. This definition includes fresh fruits and vegetables, which are sold outside authorized market areas for immediate consumption.
Although street-vended foods have potential benefits, it is also recognized that street-food vendors are often poor and uneducated and lack appreciation for safe food handling. Consequently, street foods are perceived to be a major public health risk. Various studies conducted across the globe indicated there are wide types of pathogenic bacteria, virus, fungi and protozoans were recovered from street vended foods [12-17]. Although viruses are likely the most common cause of unhygienic food associated disease, but are rarely studied and confirmed as of the short period and self-limited nature of the sickness. Moreover, the difficulty of laboratory investigation and high cost of viral studies lead to a lack of clinician investigation and hence largely underreporting. In contrast to virus, bacteria are the most common documented cause of food borne illness.
In Ethiopia wide type street-vended foods have been widely used. These include local bread ('ambasha' and 'kita'), raw fish, chilli ('awaze'),"kitfo", macaroni, egg sandwich and many others [18-21]. Different studies conducted in Ethiopia showed that street-vended foods were contaminated by potential pathogenic bacteria which include Salmonella spp., Shigella spp, and Staphylococcus aureus [18,21,22]. In one study conducted in the capital city, Addis Ababa, Salmonella typhimurium, Shigella flexneri and Staphylococcus aureus grew in street-vended food samples for hazardous levels indicating unhygienic handling and preparation [19]. Many of the studies concluded that street foods are heavily contaminated with micro-organisms and are potential sources of food borne infections. Another study conducted in Hawasa town showed E. coli was the most frequent bacteria isolated from street vended food followed by Salmonella species and S. aureus [16]. Similarly, a study conducted in Jijiga town indicated most of the street vended foods had pathogenic bacterial contaminations which include E. coli, S. aureus and Salmonella species [22]. Apart from bacteria, viral contamination of street vended foods also reported in different parts of the world [23]. This shows that street vended foods might be the potential risk way through which pathogen transfer in the community and hence the novel coronavirus might also transmit from infected person to health while using them.
In addition to microbial contamination, street vended foods also create a situation in which many people gathered at one place which in turn favours the fast spread of the novel coronavirus. Coffee ceremony is the best example in which people gathered in one place to drink coffee. It is commonly practiced activity in almost all parts of Ethiopia both in urban and rural in daily basis. The gatherings of many people at one place and unhygienic condition of the cups have been noticed during this coffee ceremony and these result the possible transmission of infectious agents from person to person. Therefore, avoidance of such places and mass awareness and keeping the hygiene of the utensils might be important to reduce the risk of infection.
In general, if a community is to have the full benefits of street-vended foods with minimal risk of foodborne disease, government intervention is required to ensure that the standard of safety for such foods is the best attainable in the context of the prevailing local situation otherwise it remained a threat to public health and contribute to the spread of emerging and re-emerging diseases.
In Ethiopia, raw meat has been consumed widely in almost all age groups in all parts of the country. Many studies reported that raw meat contains different species of bacteria and elements which have potential health hazards. Eating raw meat is uncommon and unacceptable scientifically, although it remains difficult to break this tradition in Ethiopia. Meat can harbor different types of microorganisms. Vast species of pathogenic bacteria that include Salmonella spp., Staphylococcus spp., Shigella spp were isolated from ready to consume meat collected from different meat shops and restaurants in different parts of Ethiopia [24-26]. The viral transmission through eating raw meat also reported. The deadly severe acute respiratory syndrome (SARS) coronavirus (SARS-CoV), a novel virus that caused the first major pandemic transmitted from animals to human through eating exotic game food animals such as civets [27]. The contamination of the novel coronavirus (COVID-19) might occur during transportation and processing the meat as it has not occurred in hygienic conditions. Further transmission from infected animals might also suspect as the virus recently recovered from different animals in the USA [28]. To this end, the public may get infected when a person eats the contaminated raw meat purchased or served from meat shops and restaurants. Hence, strong measures should be taken to exclude raw meat from the food menu in a restaurant and regular supervision and controlling rules and regulation should be set by the government and mass awareness is critical to discourage consumption of raw meat by the public. In addition, surveillance studies are crucial to know the level of the problem.
Khat (Catha edulis) leaves are a legal stimulant widely used by many peoples in Ethiopia [29,30]. The fresh leaves consumed without washing or any treatment and hence the possibility of causing disease to human is high. The khat (Catha edulis) leaves can easily get contaminated with pathogenic microorganisms during harvesting through human handling, harvesting equipment, transport container, wild & domestic animals. There is opacity of data, on this regard and future studies should be conduct to know the microbial dynamics of khat (Catha edulis) leaves. Studies indicated different types of pathogenic virus, bacteria, spores of fungi and worms were isolated from surface of leaves [31-35]. Infection of a healthy person is by eating raw leaf and viral infection might be through touching own noise and eye by own infected hands. In Ethiopia, khat (Catha edulis) is chewed in groups and these gathering further enhance person to person transmission. Hence, the novel coronavirus is contagious and can easily transmit from infected to healthy peoples through khat directly via infected khat (Catha edulis) leave and indirectly by favouring people gathering. To this end, strong controlling measures should be taken in order to avoid peoples gathering for chewing khat and awareness creation of the mass extremely important to avoid infection through contamination while consuming unhygienic leaf of khat (Catha edulis). Further, studies on isolation and identification of medically important microorganisms necessary for the further understanding of colonizers of khat (Catha edulis) leaves (Figure 2).
 Figure 2: Fresh khat (Catha edulis) leaves on sale in market (a) khat (Catha edulis) leaves and shoots wrapped in banana leaves (b).
View Figure 2
Figure 2: Fresh khat (Catha edulis) leaves on sale in market (a) khat (Catha edulis) leaves and shoots wrapped in banana leaves (b).
View Figure 2
Ethiopia is among the countries with poor public transportation facilities [36]. Ethiopia has the lowest motorization rate globally, with only two cars per 1000 inhabitants in 2014 [37]. Private vehicle owners are very low and a great majority depends on mass transportation, which includes taxes, buses and train. Even the mass transportations are scares and peoples are forced to use overloaded buses and trains which expose them to infection of viruses and other pathogenic bacteria.
Peoples get infected by a contagious virus while using mass transportation system either from contaminated vehicle body parts or and droplets generated while infected person sneeze. Hence, sharing of the public transportation with infected individuals without protections leads to fast transmissions of the novel coronavirus among the healthy community. To this end, the government should take all necessary regulatory measure to insure public safety in a sustainable manner. In addition, mass awareness should be crucial to avoid the public use of mass transportation and implementation of using masks and hand sanitizers while using public transport should be compulsory.
The lack of Electronic markets to get essential goods for daily basis in Ethiopia is a great concern during the pandemic. The modern e-market and home delivery system are almost absent and those present are also limited in the capital city and also not affordable to the majority of the population. To this effect, peoples are forced to out from their home to buy most of their daily basic goods and difficult to keep people in their homes during the pandemic. Moreover, in the majority of the small cities in Ethiopia, there is a unique tradition that peoples of a given city or kebeles conventionally use specific place on specific days for selling and buying of different agricultural and industrial products. This creates a multitude of peoples in a given area which enhance physical interaction and create a situation that does not allow implementation of social distancing strategy and hence contribute to the spread of the novel coronavirus. In addition, the use of currency note during transaction might also favors transmission of the virus. Study conducted in USA indicated that the novel coronavirus remained stable on Bank Notes for at least 8 h at 22 °C and 4 h at 37 °C [38]. To this end, in Ethiopia context, markets should be taken as a potential area that creates flattering conditions for transmission of the novel coronavirus. Person to person transmission might be through aerosol and sharing of contaminated materials during buying and selling. Therefore, regulatory bodies should take necessary measures to avoid crowding and create awareness to implement social distancing. In future, the government should work on encouraging the public sector in promoting modern market and e-commerce in Ethiopia not only for the sake of modernization but also taking as a strategy to combat the spread of diseases.
In Ethiopia there are many unavoidable public gatherings that the society inherited from its ancestors. The bases of these gatherings are for the sake of common mutual benefits that include economic and psycho-social benefits [39]. The different unavoidable public gathering include attending of funeral ceremonies, traditional festivals, religious gathering are mentioned. The government of Ethiopia declared a 5-month State of Emergency in an effort to limit the spread of the coronavirus (COVID-19) on 14th April 2020 and among the various measures implemented the banning of all public gatherings of more than four people primarily mentioned [40]. However, this measure has not been implemented or uniformly throughout the country for various reasons and hence it remains a trait for the spread of the pandemic. These public gathering occasions are almost unavoidable in the society unless strong controlling measures implemented by the local government. Transmission of the novel coronavirus from person to person is through sharing common staffs and aerosols during these social gatherings. Therefore, mass awareness along with strong regulatory measures should be crucial to reduce the fast transmission of the virus.
The economic background of the majority of the Ethiopian population is below the poverty line that leads to poor way of life and increase variability to infectious diseases as well as the pandemic novel coronavirus. The absence or poor access to personal protective equipment (PPE), large family size with poor housing, mobility of the citizens to win daily bread and engaging in very risky working conditions that allows them for infection are among the major factors that contribute to high chance of infection in the society. Studies conducted in USA during this pandemic indicate that peoples with low socioeconomic status are highly vulnerable to the infection of novel coronavirus [41-43]. Therefore, strong and continuous intervention is extremely crucial to support the poor during the pandemic, either wise a dire consequence will happen.
Addis Ababa, the capital city Ethiopia is a hub of international organizations and African union and hence high international travel. The movement of peoples from different parts of the world to Addis Ababa is high and this might increase the chance of spreading of the COVID-19. The first two case reports of COVID-19 in Ethiopia are the best indication. The movement of peoples to and from neighboring countries Djibouti, Somalia land, Kenya, Sudan and south Sudan are also a great concern.
Many cross-border drivers were tested positive for COVID-19 since the outbreak in Ethiopia. Specifically, the movement of cross-border truck drivers to and from Djibouti is high and need strong controlling measures. A notification note on COVID-19 situational update released on 19 May 2020 from Ethiopia health minister indicated that among the total 14 confirmed positive cases one is a cross border truck driver with travel history. Some of them were discovered after they travel many miles though different area of the country. Many of Ethiopian citizens who were illegal and legally migrated to Arab countries for various reasons were banished to Ethiopia and these might also enhance the spread of the virus if they were infected prior to their arrival. Ethiopia is also a host of many immigrants from neighbouring countries South Sudan and Eritrea and this can also contribute to the spread of the pandemic. The continuous movement of immigrants and the poor security system across the border might increase the chance of spreading the virus. Hence, strong controlling measures should be taken to monitor the movement of peoples across the borders of neighbouring countries.
The collaboration between Ethiopia and the neighboring countries are tremendously important to minimize the spread of the novel coronavirus. The government of neighboring countries should work together by setting common strategies in order to implement controlling measures (For example: closing and opening of borders, establishing quarantine and COVID-19 testing centers) to mitigate the spread of the pandemic between the neighboring nations. There should be cautious while implementing controlling measures. For instance, Reducing flows of people while keeping borders open for transportation of goods extremely important for the people of neighboring nations. Hence, collaboration based on mutual understanding between the neighboring nations will be crucial and mandatory in the fight against a pandemic.
Generally speaking the direct association of weather condition and spread of the novel coronavirus has not been known. However, it might contribute to the spread of the pandemic indirectly in a country with very poor infrastructure facilities like Ethiopia. In Ethiopia there is a long rainy season, which commonly starts from June and ends in September. The poor transport infrastructure in the country might become an obstacle during rainy season to give humanitarian service in the rural part of the country and contribute to the spread of the virus. Although there is no study so far indicating the contribution of climatic condition for the spread of virus, in study conducted in Taiwan water-borne infections, extreme torrential precipitation (> 350 mm/day) was found to result in the highest relative risk for bacillary dysentery and enterovirus infections when compared to ordinary rain (< 130 mm/day) [44]. In another study conducted in USA SARS-CoV-2 the incidence of disease declines with increasing temperature up until 52 °F and is lower in warmer versus cooler temperatures [45]. Infectious diseases, which include malaria, have been so prevalent during this season in Ethiopia which will worsen the condition. Therefore, strong intervention plan and its execution to control the disease are strongly crucial.
Strong and coordinated leadership tremendously crucial for prevention and controlling of the novel coronavirus since little have been known about the disease. According to a recent analysis of fragile state index 2013-2020 Ethiopia is ranked as 21st from the world, showing that an alert to any political crisis [46]. According to a recent analysis, coronavirus crisis is actually increasing the risk of political instability. The probable for the virus to wreak havoc in fragile and conflict-affected states is very high [47]. It is evident that political instability leads to poor service delivery with very less coordination. The poor commitment to control the pandemic among the political, less coordination among the health sector, increasing violence, demonstration and other similar factors will contribute to the spread of the virus. Although there is no report that indicate association of mass gathering and spread coronavirus, lack of implementation of social distancing and improper use of masks during mass protests obviously contribute the transmission of virus from asymptomatic infected person to health person. In Ethiopia mass demonstration of the public was observed during the occurrence of the pandemic in the capital city as well as most parts of Oromia region following the assassination of known Ethiopian singer Hachalu Hundessa on 30th June 2020. The close contact of the mass during demonstration and not using of PPE contribute the spread of the virus. Therefore, strong mutual understanding and commitments of the political organizations in the country is strongly crucial to fight the pandemic and wellbeing of the people they are struggling for, otherwise it complicates the situation leading to more difficult condition.
Ethiopia is among the countries with low coverage of public health institution with very poor medical facilities [48]. Although the government of Ethiopia is striving to establish treatment and quarantine centres of COVID-19 across the country, it is very low with respect to population proportion. The low coverage of health institution will increase the number of people lacking treatment which will lead to increase mortality. The less medical facilities in the health institution will increase the chance of death of patients that might be recovered. Therefore, the strong intervention plan and international support is extremely crucial to decrease and further more to circumvent spread of the pandemic.
Global health programs have been supporting Ethiopia in response to COVID-19 outbreak, through the Ethiopia Field Epidemiology Training Program (EFETP) graduates and residents. EFETP residents and graduates are supporting the country in various ways that include enhanced surveillance within facilities and the community, which includes house to house surveys, mortality surveillance, and hospital-based pneumonia surveillance. The EFETP residents are involved in top data analysis and visualization, drafting protocols and guidelines, and undertake virtual trainings. According to the country report, more than 100 residents and 40 graduates are actively engaged in the active case search, contact tracing, point of entry screening, and laboratory testing at the national and regional level [49].
Health care workers are primary essential workers in the chain of controlling the pandemic. They are also among the groups that have a high chance of infection by the novel coronavirus. During the pandemic high infection of health care workers were reported in different countries [50-53]. The knowledge, attitude and practice of medical staff are vital in any health care system to control the spread and treatment of patients [54]. Knowledge regarding the virus, pre and post-infection and how to treat patients is extremely crucial. The fact that the disease is new, updating the knowledge of health professionals in a regular basis is important to prevent infections and treatment of patients. The less informed medical staff fails to implement new knowledge to control the virus, porn to infection and increase death due to the virus. The attitude of health professionals, especially who is working in treatment centre is vital to control as well as treat patients. The positive attitude of health professionals is so crucial and a base for putting their knowledge to practice. The low attitude of the health professional might be due to lack of updates knowledge about the virus, poor availability of PPE that will increase chances of infection and also might be due to lack of good professional commitment or the combination of these. Therefore, trainings should be given to the health professionals on a regular basis, they should get consistent access of PPE and incentive packages should be studied and implemented that might positively affect the attitude of health professionals. Implementation strong monitory and evaluation system is also mandatory on regular base to evaluate the level of practice of the health professionals in the health care system.
In the current scenario of Ethiopia, controlling of the pandemic needs understanding of socioeconomic, cultural and political situation of the country to identify and tackle factors contributing to the spread of the virus. To this end, only the synergy of governmental organization, non-governmental organizations, political organizations, social institutions, religious organization and international institution will stop further spread of the pandemic either wise it remains a trait for years.