Reported infections of SARS-CoV-2 likely underestimate the prevalence of infection in affected communities. Seroprevalence studies allow us to understand how the virus is spreading through this local community and help us to identify people with previous infections known or unknown. This study is an epidemiologic survey to evaluate seroprevalence data in a rural community. Participants were tested between September 2020 to March 2021 using a Biohit SARS-CoV-2 IgM/IgG quick test. The positive findings of SARS-CoV-2 antibodies indicated if individuals were infected at some point since the start of the pandemic. The purpose of this study is to provide us with a better historical view of COVID-19 infection and to determine the variation in prevalence over time. Possible limiting factors to results include testing exposure or antibody prevalence in patients requesting testing. This may not be representative of the population as a whole.
SARS-CoV-2 belongs to a broad family of viruses called Coronavirus. It is one of seven known Coronaviruses that affect humans. Two other coronaviruses that have caused previous outbreaks include SARS and MERS, which emerged in 2003 and 2012 respectively. They all share the same characteristic of being enveloped, positive-sense, single stranded, zoonotic RNA viruses [1]. Transmission is mainly through respiratory droplets especially during speaking [2]. Other modes include airborne transmission during coughing, sneezing, or singing [3]. Direct contact of saliva and fomites are also avenues of transmission [4].
In regard to viral load, the data is inconsistent as to when the peak viral load is. It was first thought that viral load peaked within a week of the onset of symptoms, but those studies used upper respiratory tract samples. Stool and sputum samples on the other hand show a viral peak two weeks after the onset of disease [5]. Although viral load values are still being disputed (i.e. higher viral loads found in throat vs. nasal samples), the positive correlation between viral load and disease severity has been found to be statistically insignificant [5].
PCR and viral cultures pose a strategic disadvantage in mass testing due to cost and time therefore rapid test kits are a more viable choice for seroepidemiological studies. A seroepidemiological survey through SARS-CoV-2 antibody testing would inform us of the level of immunity of the community. Although it does not provide the incidence of SARS-CoV-2, it gives us a more accurate estimate of the true number of infections due to the high proportion of asymptomatic or mild infections [6,7]. As Brazin, et al. points out, North Carolina is largely suburban and rural [8]. It is of interest to discuss factors unique to rural communities like Harnett County that affect the rate and infectivity of the novel SARS coronavirus. These factors include but are not limited to age, types of employment, and even access to public transportation. It is our goal to first find out the seropositivity rate within Harnett County and then we can postulate how different factors unique to Harnett County and State wide-mandates have affected prevalence. Notable North Carolina Directives issued by the governor are provided in the timeline below:
• January 20, 2020 was the first confirmed case of COVID-19 in the United States [9].
• March 3, 2020 was the first reported case in North Carolina [10].
• March 13, 2020 was the first reported case in Harnett County, NC [11].
• March 30, 2020 - May 8, 2020 "Stay-at-home" directives were implemented [8].
• May 5, 2020 - NC enters phase one [12].
• May 20, 2020 - NC enters phase two [12].
• September 30, 2020 - NC enters phase three [12].
• December 17, 2020 - Vaccine distribution for Healthcare workers at Harnett County.
• December 30, 2020 - NC extends phase three [12].
• Biohit SARS-CoV-2 IgM/IgG Antibody Test Kit used is a single-use rapid immunochromatographic test for the qualitative detection and differentiation of IgM and IgG antibodies to SARS-CoV-2 in human serum, plasma and venous whole blood. Intended for use as an aid in identifying individuals with an adaptive immune response to SARS-CoV-2 indicating recent or prior infection.
• This antibody test uses the immunochromatographic method detected by SARS-CoV-2 recombinant N-protein antigen and mouse anti human IgM/IgG antibody. The antibodies in the sample react with the SARS-CoV-2 recombinant N-protein antigen bound to gold particles. The sample diluent allows for a suitable environment for the reaction of antigen and antibody. In a positive result, gold-labelled SARS-CoV-2 recombinant antigen-antibody complex binds to the IgM/IgG test line and the purple/red color is observed. Sufficient specimen volume is assured when a purplish red line forms on the control line.
• Finger Prick blood test-safety lancet to make a finger prick, allow droplets of blood to form and use a capillary tube or pipette to draw blood into the collection vessel by capillary action and test sample immediately after collection. Place blood on the test card, drop two drops of sample diluent, wait 15 min for final test results.
• SARS CoV-2 IgM/IgG complex- 97.5% sensitivity, 99.5% specificity IgM and 100% specificity IgG.
Results of this epidemiological survey show that of this rural area of NC, 419 tests were performed over a 25-week period. The initial wave showed 2.8% of population tested was positive for IgM only antibodies, 1.2% positive for IgG only antibodies and 10.1% positive for both IgM and IgG. Second wave of tests showed 2.92% positive for IgM only, 1.75% positive for IgG only and 9.94% positive for both IgM and IgG.
Demographics of patients in the study included almost double the amount of females to males, a wide age range from two to 89-years-old and a varied range of zip codes within the county (Table 1, Table 2, Table 3 and Figure 1).
 Figure 1: Example of various test results showing COVID-19 nucleocapsid protein IgM and/or IgG antibody rapid serological positive test results.
View Figure 1
Figure 1: Example of various test results showing COVID-19 nucleocapsid protein IgM and/or IgG antibody rapid serological positive test results.
View Figure 1
Tables 1-3: Depicts the variety of demographics of individuals tested. View Table 1-3
• Initial wave: (Sept 14-Dec 9): Percentage in population positive for IgM only, IgG only, IgM and IgG (Table 4 and Figure 2).
 Figure 2: Summary of COVID-19 nucleopcapsid protein IgM/IgG antibody rapid serological test results in First Wave by history of known exposure/infection.
View Figure 2
Figure 2: Summary of COVID-19 nucleopcapsid protein IgM/IgG antibody rapid serological test results in First Wave by history of known exposure/infection.
View Figure 2
Table 4: Summary of COVID-19 spike protein IgM/IgG antibody rapid serological test results in First Wave by history of known exposure/infection. View Table 4
⚬ 248 total tests
⚬ IgM Only: 7
⚬ IgG Only: 3
⚬ IgM and IgG: 25
Important Note:
1) Ten (10) of the 35 IgM and/or IgG positive individuals (28.57%) in the first wave of testing had no known exposure or infection to COVID-19 and had no history of positive PCR test prior to antibody testing.
• Second wave: (Dec 10-Mar 6): Percentage in population positive for IgM only, IgG only, IgM and IgG (Table 5 and Figure 3).
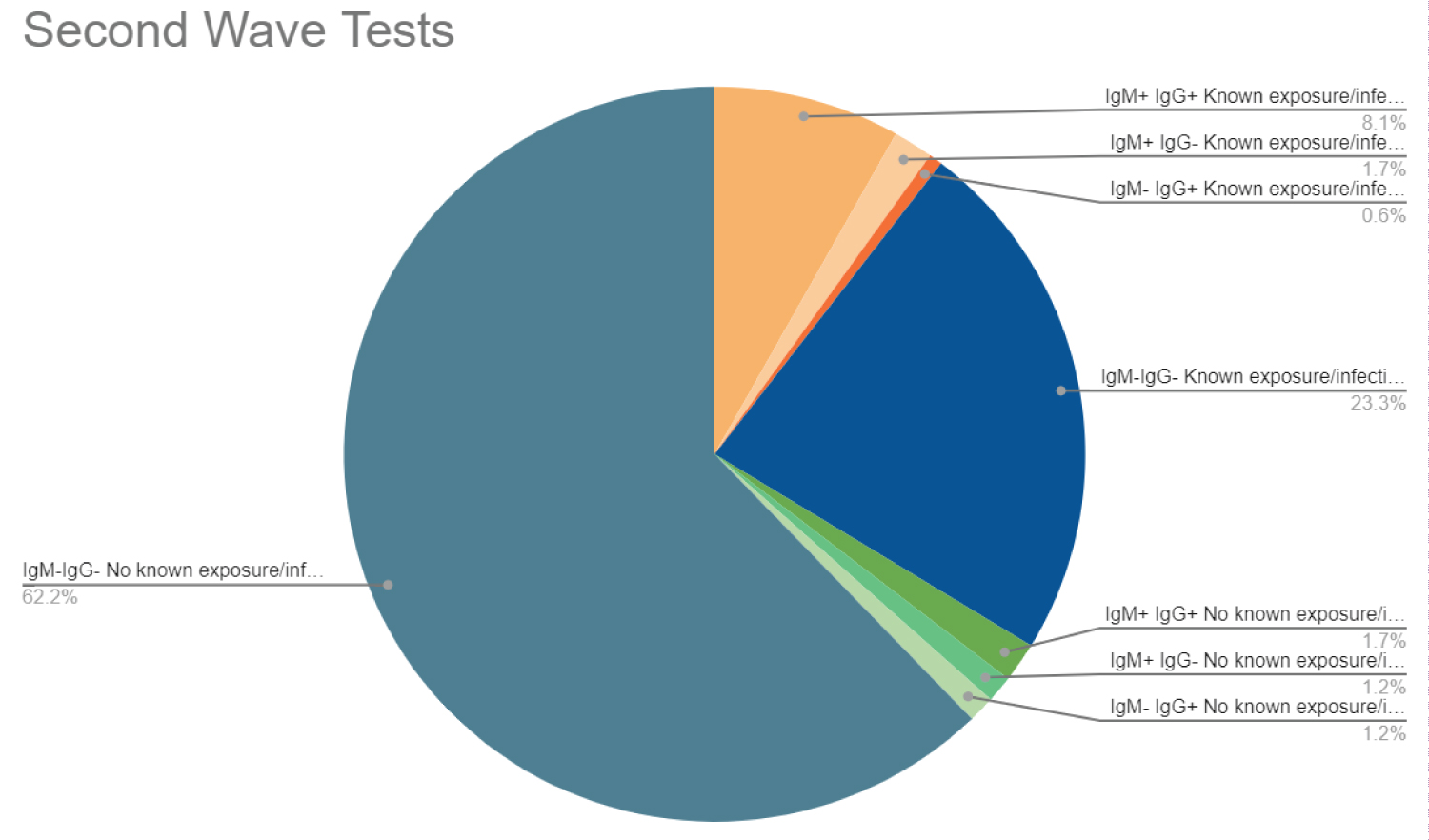 Figure 3: Summary of COVID-19 nucleocapsid protein IgM/IgG antibody rapid serological test results in Second Wave by history of known exposure/infection.
View Figure 3
Figure 3: Summary of COVID-19 nucleocapsid protein IgM/IgG antibody rapid serological test results in Second Wave by history of known exposure/infection.
View Figure 3
Table 5: Summary of COVID-19 spike protein IgM/IgG antibody rapid serological test results in Second Wave by history of known exposure/infection. View Table 5
⚬ 171 total tests
⚬ IgM Only: 5
⚬ IgG Only: 3
⚬ IgM and IgG: 17
Important Note:
1) Seven (7) of the 25 IgM and/or IgG positive individuals (28.00%) in the second wave of testing had no known exposure or infection to COVID-19 and had no history of positive PCR test prior to antibody testing.
While no large-scale antibody testing has been done across the US, the CDC estimates that 83.1 million individuals in the US have been infected with COVID-19 between Feb-Dec 2020 [13]. With the US population estimated to be around 328.2 million it would calculate that approximately 25% of the US population had been infected with COVID-19 [14]. In North Carolina 8.4% of the state population has tested positive (as of 3/12/21). In Harnett County the NC Department of Health Services reports that 7.4% of the population has tested positive [15]. These documented prevalence rates support the initial hypothesis that a rural setting like Harnett County would be lower than the rest of the population based on factors including but not limited to age, types of employment, access to public transportation and travel in and out of the county.
In this study we found a higher prevalence in comparison to the general population of Harnett county. Approximately 14% of the population we tested was positive for COVID antibodies. The most likely reasoning behind this higher prevalence was that those documented positive by the county likely only presented for testing due to symptoms. However, our study tested individuals with or without symptoms and with or without known exposure expanding on our opportunity for possible positive tests.
In our study of Harnett County 14.3% tested positive, with 14.1% of the first wave of testing positive and 14.5% in the second wave. Of those that tested positive 28.3% had no known previous infection/exposure to COVID-19 (28.6% in first wave 28% in second). This is consistent with the hypothesis that many people who are infected with COVID-19 have asymptomatic courses and that the estimated numbers of infection within the United States may in fact be lower than the actual number of those that have been infected with COVID-19.
This study has several important limitations. These include: Persons may not represent the county population as a whole in regards to access to care, interest in seeking care/medical attention, exposure risk, or adhering to prevention measures. This study was not designed to represent the nation as whole but rather provide an insight into the distribution of Seropositive Prevalence of Antibodies against SARS-CoV-2 in Rural Harnett County, North Carolina, which limits the ability to compare across multiple counties.
Laboratory testing was also self-performed a method which is subject to potential biases if samples were not appropriately drawn or results were not properly documented. Other limitations include delay to testing time, difference in number of tests performed in the first wave versus the second wave, more individuals who tested positive for COVID presenting for tests.
This study designed to observe seropositive prevalence of antibodies against SARS-CoV-2 in Rural Harnett County, North Carolina found between both waves of high infection rates 14.3% of the cohort of the 420 individuals tested positive for SARS-CoV-2 antibodies. We further showed that of the individuals tested in this small rural area of NC in both waves of high infection rates almost 30% of individuals that tested positive have no prior known exposure or infection. Our results showed that the need for preventative health measures to limit the spread should still be reinforced as there are many people who had asymptomatic courses of COVID-19 testing positive for SARS-CoV-2 antibodies with no prior exposure/infection showing that many of the estimated infection numbers might be much lower than the actual number of those infected.
None to report.
This project was supported by North Carolina House Bill 1043 COVID-19 Response through Campbell University, Incorporated and a Campbell University School of Osteopathic Medicine (CUSOM) Sub-recipient Award (grant award #25-00).
Provided access to testing kits to allow for study, no further influence on study results.