Decreased physical activity levels have been reported in those with chronic ankle instability. It is unknown when this decline in activity occurs. Therefore, the purpose of this study was to examine physical activity levels before and one year after an acute lateral ankle sprain (LAS).
Twenty subjects (7 males and 13 females, age = 21.7 ± 2.7 yr, mass = 79.4 ± 18.1 kg, ht = 173.2 ± 9.5 cm) with an acute LAS and twenty healthy subjects (7 males and 13 females, age = 20.4 ± 2.9 yr, mass = 80.6 ± 22.3 kg, ht = 172.4 ± 8.7 cm) participated. Subjects were given activity questionnaires to estimate their physical activity levels the week before they were injured and one year after the injury.
There was a significant interaction (p = 0.001) for the NASA physical activity scale. Subjects in the LAS group scored significantly less at the 1-year mark compared to their pre-injury levels (p = 0.001), and significantly less (p = 0.02) than the healthy group at the 1-year mark.
It appears one year after a LAS subjects are significantly less physically active. Further research is needed to understand why subjects have decreased physical activity, as this decreased activity could lead to the development of other chronic injuries and/or illnesses.
Ankle injury, Physical activity, Exercise
One of the biggest public health issues present today is physical inactivity. Physical inactivity is currently classified as one of the three highest risk behaviors in the development of cardiovascular disease, cancer, and other chronic diseases such as diabetes and obesity [1]. Research consistently demonstrates the numerous physiological health and psychological well-being benefits with regular physical activity [2,3]. Lee, et al. [4] estimated globally 5.3 million deaths per year are a result of physical inactivity. Additionally, the worldwide economic burden of physical inactivity has been found to cost approximately $67.5 billion for 2013 [5]. Knowing the importance of physical activity to maintaining a healthy lifestyle, as well preventing chronic disease development, anything that lowers physical activity levels is concerning. Thus, understanding the impact common musculoskeletal pathologies has on physical activity is crucial towards the maintenance of a healthy lifestyle.
Despite an immense amount of research examining the causes and treatment of ankle sprains and chronic ankle instability (CAI); ankle sprains remain the most common musculoskeletal injury [6]. The first consequence of an initial ankle sprain is the development of CAI. With upwards of 70% of patients who sprain their ankle going on to develop CAI [7]. The second consequence is the development of post-traumatic ankle osteoarthritis. Ankle instability accounts for 80% of post traumatic ankle osteoarthritis cases [8]. Along with this data, we know that approximately 50% of patients that sprain their ankle never seek treatment, so some of this data may be underestimated by the lack of patients seeking treatment and reporting injury [6,9,10]. Even with the high percentage of disability and long term consequences to an ankle sprain, it is often thought of as an inconsequential injury. More recent evidence has started to demonstrate the impact an ankle sprain may have on regular physical activity patterns, and early results point to ankle sprains being a bigger public health burden than traditionally given credit for, and thus needs to be treated as such [11-13].
One of the bigger areas of research in regards to consequences of ankle sprains and CAI development is subjective function via patient reported outcomes. When examining the research, it has consistently demonstrated subjects with CAI score significantly less on subjective self-report scales including the foot and ankle ability measure (FAAM), and the foot and ankle disability measure (FADI), and the FADI sport version [14-18]. Although these questionnaires are based on subjective self-report (assess ability to perform common activities of daily living; walking, going up and down stairs, etc), they have been reported as valid instruments to assess subjective function. In addition to ankle specific subjective reporting, research has also reported subjects with CAI scored significantly less on health-related quality of life (HR-QOL) and had significantly more functional limitations [19]. Additionally a negative correlation was reported between HR-QOL scores and functional limitations. The HR-QOL addresses functioning in everyday life and personal evaluation of well-being [19]. These decreases in subjective self-report and health-related quality of life all may have a negative effect on physical activity levels. It is also possible that if physical activity levels are decreased in those with CAI, the decreased physical activity levels could negatively impact subjective function and HR-QOL. Knowing subjects report changes in their subjective level of function, the need for more objective physical activity data is needed.
Recently, Hubbard-Turner & Turner [12], reported a significantly decreased step count in subjects with CAI compared to a matched control group. The authors also reported functional limitations in the subjects with CAI which may explain the decrease in step count [12]. One of the limitations of this research is the uncertainty of subject's decreased physical activity being caused by CAI. Another study by Hubbard-Turner, et al. [11,13] induced an ankle sprain in a mouse model and followed the mice for their entire lifespan. The authors reported that a single severe ankle sprain significantly reduced physical activity levels across the lifespan compared to mice with a minor ankle sprain and the control group [11,13]. It is unknown if similar results would occur in a human model, but based on the current animal and human evidence, it can be reported that ankle sprains have a negative impact on regular physical activity levels, and continued research is needed.
Based on some limited evidence, ankle sprains, while often viewed as mild injuries, appear to represent a significant public health problem and a major healthcare burden. However, further research is needed to better understand the impact an initial acute lateral ankle sprain has on physical activity levels. The purpose of this study is to examine the physical activity levels before and one year after an initial acute lateral ankle sprain (LAS).
Twenty college students (7 males and 13 females, age = 21.7 ± 2.7 yr, mass = 79.4 ± 18.1 kg, ht = 173.2 ± 9.5 cm) with an initial acute LAS and twenty healthy college students (7 males and 13 females, age = 20.4 ± 2.9 yr, mass = 80.6 ± 22.3 kg, ht = 172.4 ± 8.7 cm) participated in the study. For those with an acute LAS the following criteria had to be met: 1) Be between the ages of 16 and 50, 2) Have a first time lateral ankle sprain or first repetition of a lateral ankle sprain more than 1-year after the last sprain, and 3) Have the lateral ankle sprain occur within the past 72-hours. Exclusion criteria for the acute LAS group included: Chronic ankle instability in the involved ankle, a previous history of ankle surgery, fractures of the foot or ankle suffered at the same time as the lateral ankle sprain, or a condition known to affect pain and/or balance.
Inclusion criteria for healthy controls was the same as the acute LAS group with exception of no acute LAS. Additionally, control subjects must be within ± 10% of an ankle sprain participant's age, height, weight, physical activity level, and be of the same sex. Exclusion criteria for the control group was the same as the acute LAS group.
All ankle sprains were graded based on the following criteria [20]:
Grade 1 (mild): An injury that results in mild loss of function, point tenderness, swelling, and/or discoloration but limited evidence of ligamentous instability.
Grade 2 (moderate): An injury that results in decreased motion, some loss of function, moderate point tenderness, swelling and discoloration, and some ligamentous instability.
Grade 3 (severe): An injury that results in almost total loss of function, diffuse swelling and discoloration, extreme point tenderness, disruption of the ankle capsule, and marked ligamentous instability.
One of the authors of the paper graded the ankle sprains within 3 days of injury. A full assessment was performed (subjective, objective, range of motion, strength, special tests). The special tests included the anterior drawer and talar tilt test. All subjects were given immediate care recommendations (RICE). All LAS subjects were given a handout with post injury rehabilitation and exercise suggestions (ROM exercises, strengthening exercises, etc). Subjects were to perform these on their own, and with no supervision. All subjects provided written informed consent before participation, and the testing procedures used in the investigation were approved by our University's Institutional Review Board.
After reading through and providing informed consent, all subjects filled out three questionnaires. The acute LAS group completed all questionnaires within 3 days of the LAS. Subjects were instructed to complete the activity questionnaires based on the week before the LAS occurred. The control group completed the questionnaires after being matched to an acute LAS participant. They were instructed to complete the activity questionnaires based on the previous week's physical activity levels.
First, all subjects completed the foot and ankle ability measure (FAAM). The FAAM consists of a 21-item activity of daily living and an 8-item Sports subscale [21]. The FAAM has been reported as a reliable, responsive, and valid measure of physical function for individuals with musculoskeletal pathology of the lower leg, foot, and ankle [21]. Next, after completing the FAAM, all subjects filled out the international physical activity questionnaire (IPAQ) short form. The IPAQ is used to obtain internationally comparable data on health-related physical activity [22]. The questionnaire has 7 items to determine the kinds of physical activities as well as the intensity and volume of physical activities the subjects partake in. Lastly, after completing the FAAM and IPAQ, all subjects completed the NASA physical activity scale [23]. The NASA physical activity scale has subjects rate their general activity level for the previous month, using a scale of 0 (Do not participate in regularly programmed recreation sport or heavy physical activity, avoid walking or exertion, for example, always use elevator, drive whenever possible instead of walking) to 7 (Run over 10 miles per week or spend over 3 hours per week in comparable physical activity) [23].
One year after initial enrollment in the study all subjects returned to complete post data collection. Post data collection included filling out all of the questionnaires described above. All subjects were instructed to complete the questionnaires based on the previous week's/months physical activity levels.
All subject demographic and injury related data was analyzed using a one-way analysis of variance (ANOVA) between groups (LAS, Healthy). A two-way ANOVA (group X time) was used to determine any differences in the FAAM, the questions on the IPAQ (Table 1), and the NASA physical activity score. An alpha-level of p < 0.05 was used to determine significant effects for each analysis.
Table 1: Descriptive data. View Table 1
There were no significant differences in demographic data between the groups (age, height, weight) (Table 1). Means and standard deviations of the primary outcome measures are presented in Table 2. There were no significant interactions for the FAAM (p = 0.10) or FAAM sport (p = 0.45). There was a significant difference between groups. Subjects in the healthy group scored significantly higher on the FAAM (p = 0.04) and the FAAM sport (p = 0.01) at the 1-year measurement compared to the LAS group. There was a significant interaction (p = 0.001) for the NASA physical activity scale. Subjects in the LAS group scored significantly less at the 1-year mark compared to their pre-injury levels (p = 0.001), and significantly less (p = 0.02) than the healthy group at the 1-year mark.
Table 2: Mean (± SD) for dependent variables. View Table 2
There were numerous significant interactions for the IPAQ physical activity questionnaire. The LAS subjects scored significantly less on "average time spent performing vigorous physical activity" (p = 0.04) and "average time spent performing moderate physical activity" (p = 0.02) one year after injury compared to before the LAS and compared to the healthy group. Subjects with a LAS also spent significantly less time during an average day walking (p = 0.01), and had significantly less days per week where they pursued vigorous activity (p = 0.02) or moderate activity (p = 0.04) one year after their sprain compared to before the injury occurred, and compared to the control group (Table 3).
Table 3: Effect Sizes between lateral ankle sprain pre and post measure and lateral ankle sprain and healthy group. View Table 3
The subjects with the acute LAS scored significantly lower on NASA physical activity scale at the 1-year mark compared to their pre-injury physical activity levels and the activity levels of the healthy matched control group. The acute LAS group also scored significantly lower on the subjective function (FAAM and FAAM Sport) scales. The decreased self-reported physical activity levels and subjective function is a concern. The american college of sports medicine (ACSM) recommends adults get at least 150 minutes of moderate-intensity exercise per week [24]. This can be met through 30-60 minutes of moderate intensity exercise (5 days per week) or 20-60 minutes of vigorous - intensity exercise (3 days per week). The healthy subjects in the study met the ACSM physical standards, and the acute LAS group met the standards before injury. However, 1-year after the acute LAS, subjects fell below the physical activity guidelines. This is a significant public health concern that could result in physiological and financial concerns for these individuals in the near future. The significant differences in the self-report NASA physical activity score, and IPAQ suggest even 1-year after ankle sprain subjects have not recovered or returned to previous physical activity levels. The significant difference in FAAM and FAAM sport scores likely explains the decreased physical activity levels.
Previously our lab examined physical activity levels in college students with chronic ankle instability (CAI) [12]. We reported significantly decreased step counts, and self-reported physical activity levels in subjects with CAI. One of the limitations of that study was that we did not know the subject's physical activity levels before they developed CAI. Based on the current study, one year after an acute LAS, subjects had significantly decreased physical activity levels compared to their self-report activity levels before the LAS occurred and compared to a matched healthy control group. There were no differences between the pre-injury and healthy group activity levels, so it can be assumed the LAS may have played a significant role in the decreased physical activity levels. Subjects in the current study all reported to the lab three days after sustaining an initial lateral ankle sprain. The subjective questionnaires regarding their physical activity levels before the sprain were administered at that time, so although not truly prospective in nature, this study provides a good understanding of the subjects physical activity levels before they were injured as well as their physical activity level one year after injury.
According to the CDC, regular physical activity is one of the most important things you can do for your health [25]. It can help: control your weight, reduce the risk of cardiovascular disease, reduce the risk for type II diabetes and metabolic syndrome, reduce your risk of some cancers, strengthen your bones and muscles, improve your mental health and mood, improve your ability to do daily activities and prevent falls, and increase your chances of living longer. Based on this study and previous research, a ‘simple' acute LAS may decrease physical activity levels likely due to the subjective self-report symptoms that subjects report. So although an ankle sprain is often thought of a minor injury that doesn't warrant much attention, with improper care and management, the long-term health issues of an ankle sprain may be significant.
Based on research it is known that regular physical activity levels decline with aging in healthy people [26,27]. The public health concern becoming apparent from our research is that decreased physical activity levels that normally decline with aging is accelerated as result of a LAS. Not only is the decline in activity accelerated after an ankle sprain, the regularly expected level of physical activity achieved by that person may not be fully achieved in their lifetime. Figure 1A and Figure 1B demonstrate what may be happening to physical activity levels across the lifespan after an ankle sprain and the consequential development of CAI. We hypothesize this decreased physical activity continues across the lifespan, and then as depicted in Figure 1B, potentially speeds up the need for dependent care, as the decreased physical activity levels raises the risk for the development of chronic diseases. Although these figures are hypothetical, they are based on the lifelong physical activity data measured in mice after an ankle sprain, and based on the human studies conducted. All of these data point to decreases in physical activity levels which again could have significant impact on overall health and wellness if not changed.
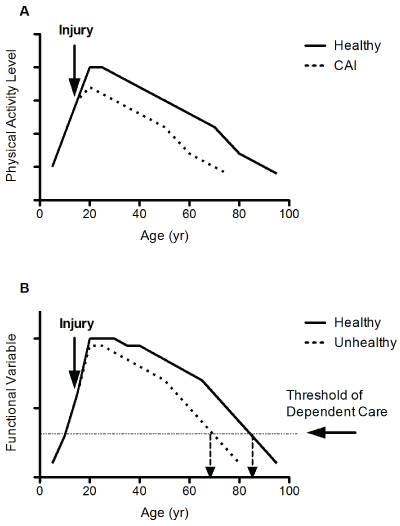 Figure 1: Graphs depicting (A) Impact of CAI on lifelong physical activity and (B) Impact of decreased physical activity across lifespan on physical functional ability.
View Figure 1
Figure 1: Graphs depicting (A) Impact of CAI on lifelong physical activity and (B) Impact of decreased physical activity across lifespan on physical functional ability.
View Figure 1
One of the primary limitations of the current study is the lack of objective physical activity data. All physical activity measurements were based off of subjective self-report. Future studies should look at tracking physical activity levels (e.g. step counts). There is the risk of recall bias in the subjects filling out the activity questionnaires. Additionally, examining health related measures to physical activity including VO2max, and % body fat are needed to understand how this decreased physical activity level may be impacting the body. Lastly, we did not measure body weight at the one year follow-up. It would be interesting to see if body weight changed over that 1-year period. Again, it appears an initial LAS in both an animal model as well as human studies result in decreased physical activity. If that decreased physical activity is also leading to increased body weight, the public health ramifications are even more significant.
Based on the current study subjects who stained an initial acute LAS had significantly decreased physical activity levels 1-year after the injury compared to pre-injury levels and a healthy matched control group. Additionally, subjects with an acute LAS had significantly decreased subjective function 1-year after the sprain relative to a healthy matched control group. The decreased physical activity levels should be a significant concern to health care professionals. Further research is needed to understand why subjects had decreased physical activity levels and subjective function one year after an ankle sprain, as this could be a significant public health concern.
National Athletic Trainers' Association Research and Education Foundation.
No financial conflicts of interest.