To examine vitamin D levels in patients diagnosed with fibromyalgia syndrome (FMS).
This study was performed at Riyadh Care Hospitals, Saudi Arabia. The data were obtained from rheumatology outpatient clinic records that routinely measure Vitamin D levels. The total number of patients in this database was 1,072. The gathered data included vitamin D serum concentration, age, and gender, as well as body mass index (BMI).
Patients were diagnosed according to Wolfe, et al. criteria for diagnosing FMS. Vitamin D deficiency (VDD) was defined according to Mayo Medical Laboratories Reference Ranges for Total Serum 25-hydroxyvitamin D [25(OH)D]: Optimal: 25-80 ng/mL; mild to moderate: 10-24 ng/mL; severe: < 10 ng/mL.
Twenty-eight patients were included in the study. The mean age was 37.8 ± 7.0 years. The average BMI was 29.3 ± 4.22. Mean Vitamin D level was 10.23 ± 4.99 ng/mL. The overall prevalence rate of VDD (i.e., 24 ng/mL and below) was high at 96.4% (27/28). In terms of severity, most of the patients (20/28; %) had severe VDD (i.e., below 10 ng/mL) with a prevalence rate of 71.4%. Regression analyses demonstrated that FMS patients with older age (45 and above), and higher BMI (30 and above) had a higher probability of having severe VDD.
The condition of VDD is frequently seen in patients diagnosed with FMS. Patients with FMS, old age, and high BMI had a higher probability of having severe VDD.
Although the sample size of the study is small, the figures are alarming, suggesting that practitioners' need to be vigilant regarding the testing of vitamin D serum levels in this patient population. Screening for VDD is particularly critical for patients 45 years and older or with BMI that is 30 and above.
Fibromyalgia, Vitamin D deficiency, Prevalance, Musculoskeletal pain, Body mass index, Age
Fibromyalgia syndrome (FMS) is a chronic, non-articular, rheumatologic disorder specified with chronic systemic musculoskeletal pains with unknown etiology, morning stiffness, fatigue, sleep disorder, multiple tender points, low pain threshold, symptoms of depression and anxiety, and intestinal dysmotility [1].
The pathogenesis of FMS is still unknown. However, it appears to be related to a neurotransmitter imbalance and upregulation of inflammatory pathways in the central nervous system (CNS), resulting in central amplification of peripheral pain signals [2]. Pain pathways associated with cortical, immunological, hormonal, and neuronal changes in chronic pain, are potentially also influenced by vitamin D levels [3]. The presence of vitamin D receptor (VDR), 1-hydroxylase, and Vitamin D binding protein (VDBP) in the hypothalamus are suggested as mechanisms by which VDD is implicated in the pathophysiology of FMS [4]. Vitamin D is also known to affect several inflammatory pathways associated with the development and persistence of chronic pain [5]. Additionally, vitamin D appears to increase muscle strength through nuclear receptors in muscle tissue. In humans, VDD, if untreated, results in myopathy [6].
Overall, although a cause-and-effect relationship has not been proven, available evidence indicates that vitamin D is a vital regulator of pain pathways involved in FMS pathogenesis. Hypovitaminosis D may be a risk factor for FMS and a way of worsening the symptoms through central and peripheral pathways.
During the last decade, several observational studies attempted to investigate the association of hypovitaminosis D and symptoms of FMS. Initial reports, although included small samples, showed that hypovitaminosis D is frequently seen in FMS. However, not all previous evidence reports similar findings. Previous studies manifest great variation in ethnic, cultural, gender, enviromental, and dietary habits, factors that have a major impact on vitamin D status. Due to the possible influence of genetic, ethnic, environmental factors, and lifestyle on vitamin D levels, we became interested in investigating vitamin D serum levels in FMS patients in Saudi Arabia.
The study design was a cross-sectional analysis of retrospective data. The data were obtained from rheumatology outpatient clinic records that routinely measure Vitamin D levels. Due to the nature of the study, patient consent was not required. The total number of patients in the database was 1,072.
The total number of patients with a confirmed diagnosis according to Wolfe, et al., criteria for diagnosing FMS [7] was 28 out of 1,072 (2.6%). The gathered data included vitamin D serum concentration, age, and gender, as well as BMI. For BMI classification, we adopted the CDC classification [8] as described below:
• If BMI is less than 18.5, it falls within the underweight range.
• If BMI is 18.5 to < 25, it falls within the normal.
• If BMI is 25.0 to < 30, it falls within the overweight range.
• If BMI is 30.0 or higher, it falls within the obese range.
Obesity is frequently subdivided into categories:
• Class 1: BMI of 30 to < 35.
• Class 2: BMI of 35 to < 40.
• Class 3: BMI of 40 or higher. Class 3 obesity is sometimes categorized as “extreme” or “severe” obesity.
We conducted a severity classification [9] according to Mayo Medical Laboratories Reference Ranges for Total Serum 25-hydroxyvitamin D [25(OH)D]: Optimal: 25-80 ng/mL; mild to moderate: 10-24 ng/mL; severe: < 10 ng/mL. In this study, patients with a serum level of 24 and below were classified as having VDD.
To conduct the statistical analysis, we used the following software; BugsXla, WinBugs, OpenMeta, and Minitab 17.
The analysis included 28 patients with a confirmed diagnosis of FMS. Study patients were mostly female (24/28; 85.7%) with an average age of 38.4 ± 6.4. There were 4 male patients (4/28; 14.2%) with an average age of 34.3 ± 10.3. The overall average age of the study patients was 37.8 ± 7.0 years. The average BMI was 29.3 ± 4.22.
The overall prevalence rate of VDD among study patients was high at 96.4% (27/28) with a 95.0% confidence interval (CI) between 89.5% and 100.0%. In terms of severity, most of the patients (20/28; 71.0%) had severe VDD (i.e., below 10 ng/mL) [CI: 54.7%-88.1%]. Seven out of 28 (25.0%) patients (7/28) had moderate deficiency (i.e., between 10 and 24 ng/mL) [CI: 9.0% to 41.0%]. Only one patient out of 28 (3.5%) had a borderline optimal vitamin D level at 26.8 ng/mL (Figure 1).
 Figure 1: Distribution of severity among study patients. About 64.0% of the study patients had severe vitamin D deficiency.
View Figure 1
Figure 1: Distribution of severity among study patients. About 64.0% of the study patients had severe vitamin D deficiency.
View Figure 1
The mean vitamin D serum level was 10.23 ± 4.99, with a median of 8.6 ng/mL. Minimum serum level was 4.1, and the maximum level was 26.6 ng/mL (Figure 2). Furthermore, simulated data showed a point estimate of 9.5 ± 0.85 ng/mL (Credible Interval: 7.8 to 11.28 with a median of 9.5 ng/mL), indicating a high probability of having severe VDD among the FMS population (Figure 3).
 Figure 2: Box-plot analysis of vitamin D serum levels in study patients. The two horizontal lines are showing the references to vitamin deficiency determinations: Severe (below 10); mild-moderate (10-24); and optimal (24-80).
View Figure 2
Figure 2: Box-plot analysis of vitamin D serum levels in study patients. The two horizontal lines are showing the references to vitamin deficiency determinations: Severe (below 10); mild-moderate (10-24); and optimal (24-80).
View Figure 2
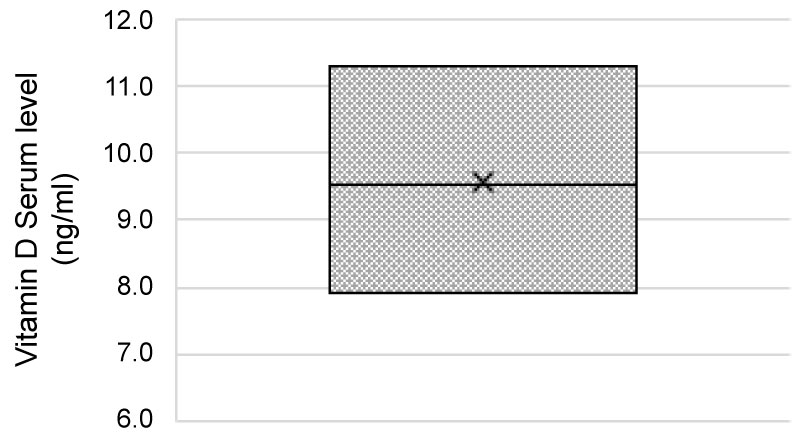 Figure 3: Boxplot graph of the simulated data: Bayesian simulation outcomes of the vitamin D serum level data. The outcomes suggest that FMS patients are very likely to have VDD with expected serum levels between 7.8 and 11.3 ng/mL.
View Figure 3
Figure 3: Boxplot graph of the simulated data: Bayesian simulation outcomes of the vitamin D serum level data. The outcomes suggest that FMS patients are very likely to have VDD with expected serum levels between 7.8 and 11.3 ng/mL.
View Figure 3
To evaluate if there were specific demographics associated with severe VDD, we examined the correlations between vitamin D levels with age or BMI. The data showed a trend towards negative correlation (-0.3) between age and vitamin D serum levels (i.e., older patients tend to have lower serum vitamin D). However, this correlation did not reach a statistical significance (P = 0.16) (Figure 4). A similar correlation was seen with regression analysis of the severity of condition versus age, with data showing that older patients tend to have a higher probability of severe VDD.
 Figure 4: Relationship between serum vitamin D and age. The correlation is negative indicating that older FMS patients tend to have lower vitamin D serum levels.
View Figure 4
Figure 4: Relationship between serum vitamin D and age. The correlation is negative indicating that older FMS patients tend to have lower vitamin D serum levels.
View Figure 4
The correlation between BMI and vitamin D serum levels was also trending negative (-0.22). However, it didn't reach a statistical significance (P = 0.26) (Figure 5). A similar correlation was seen with regression analysis of VDD severity versus BMI, showing that patients with higher BMI tend to have a higher probability of severe VDD (Figure 6). Collectively, the probability of having severe VDD in the FMS patient population was high (> 80.0%) in older patients with higher BMI (Figure 7).
 Figure 5: Relationship between vitamin D and BMI. The correlation is negative indicating that FMS patients with high BMI tend to have lower vitamin D serum levels.
View Figure 5
Figure 5: Relationship between vitamin D and BMI. The correlation is negative indicating that FMS patients with high BMI tend to have lower vitamin D serum levels.
View Figure 5
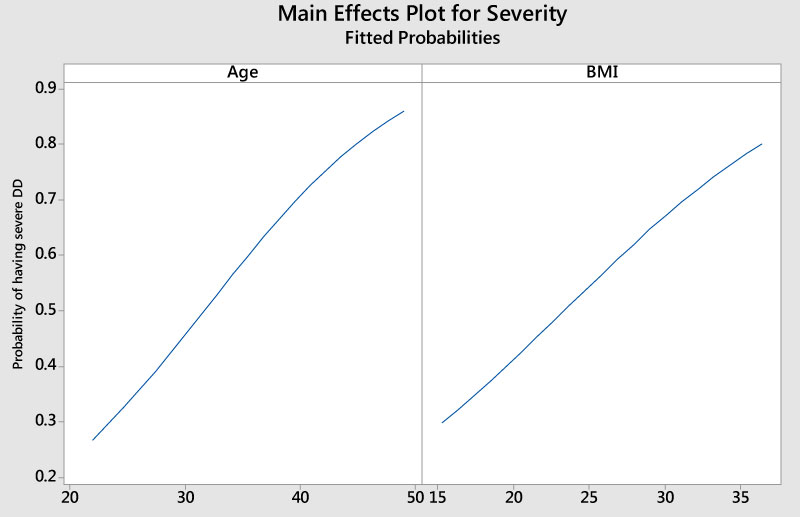 Figure 6: Probability of having severe vitamin D deficiency versus age and BMI in FMS patients.
View Figure 6
Figure 6: Probability of having severe vitamin D deficiency versus age and BMI in FMS patients.
View Figure 6
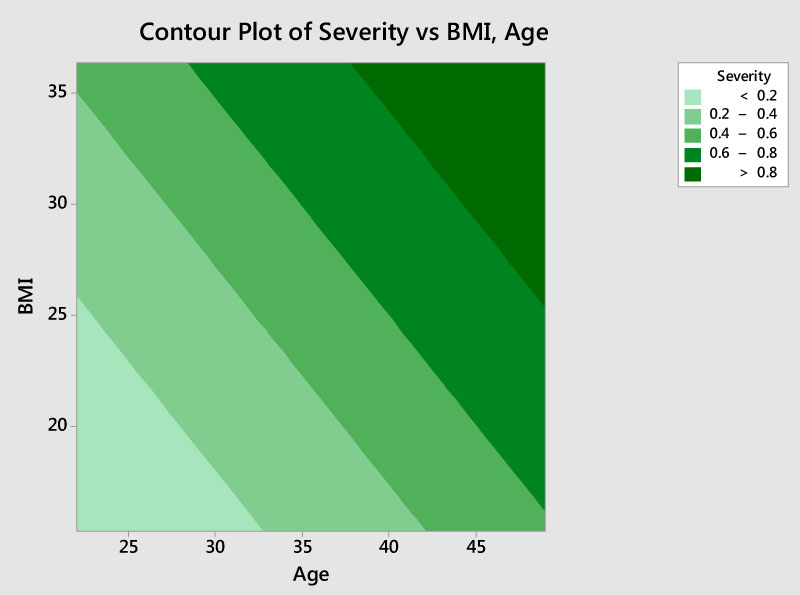 Figure 7: Contour analysis of the VDD severity versus combination of ages and BMI. The graph suggests that old FMS (above 45) with high BMI (above 30) have a high probability (> 80.0%) of having severe form of VDD.
View Figure 7
Figure 7: Contour analysis of the VDD severity versus combination of ages and BMI. The graph suggests that old FMS (above 45) with high BMI (above 30) have a high probability (> 80.0%) of having severe form of VDD.
View Figure 7
Our data regarding the high prevalence rate of VDD among FMS patients is in agreement with previous studies [1,10-15]. In an earlier study, Abokrysha, et al. examined the vitamin D levels in 30 FMS Saudi female patients, and the data showed a mean concentration of 4.76 ± 1.46 ng/mL indicating a high prevalence of severe VDD among this population [10]. Pooled data from our study and Abokrysha, et al., showed a point estimate of 7.4 ng/mL with 95.0% CI between 2.1 and 12.8 ng/mL (Figure 8).
 Figure 8: Pooled data of serum level vitamin D among FMS patients.
View Figure 8
Figure 8: Pooled data of serum level vitamin D among FMS patients.
View Figure 8
In comparison to the healthy population in Saudi Arabia [16], the prevalence rate of patients with VDD in our study was markedly higher (96.4% versus 51.7% [16]), and this difference is statistically significant (difference of 44.8% with a 95.0% CI between 36.6% and 53.0%) (Figure 9). These findings suggest that VDD has a unique and specific interplay with the pathology or clinical presentation of FMS [17]. Aging and obesity are associated with vitamin D deficiency [18]. In our study, we found a similar relationship among the FMS patients (Figure 4, Figure 5 and Figure 6). Our data showed that older and obese patients (BMI > 30) with FMS have a higher probability of having severe VDD (Figure 7). These findings suggest that practitioners should give particular attention to this high-risk subpopulation regarding the screening for VDD.
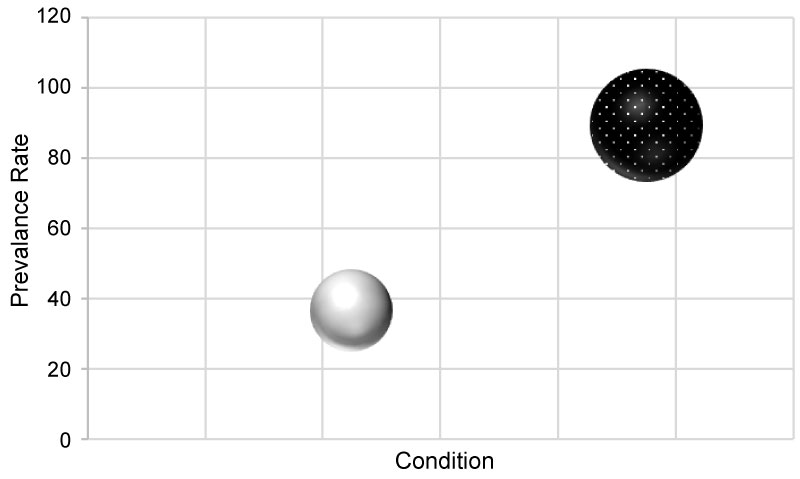 Figure 9: Bubble representation of the prevalence rates of VDD among healthy versus FMS populations. Healthy: Grey bubble; FMS: Black bubble.
View Figure 9
Figure 9: Bubble representation of the prevalence rates of VDD among healthy versus FMS populations. Healthy: Grey bubble; FMS: Black bubble.
View Figure 9
Several studies demonstrated that vitamin D supplementation could significantly improve the quality of life (QOL) of FMS patients [15,19,20]. However, these findings do not mean empirical supplementation of vitamin D for FMS patients without proper testing for VDD. Instead, patients with concurrent risk factors for deficiency should be tested and treated for vitamin D deficiency to protect from risk of osteoporosis and to improve muscular strength [21]. Additionally, considering the relationship between vitamin D, and pain as well as muscle and bone function, it is logical to assume that treating vitamin D deficiency in those patients is likely to reduce the dose and duration of immunomodulating drugs needed for the standard FMS therapy.
This study has several limitations, including the small number of patients; being based on data from a single center in one country; and the lack of control arm. However, the data presented here can pave the way for future studies with a better design and can be of value for meta-analysis data pooling studies.
The prevalence of VDD among the FMS patient population is overwhelming. Moreover, it also tends to be severe. The risk of having severe VDD is notably higher in older females (age above 45) with high BMI (above 30). Together, these data suggest that rheumatologists should pay attention to examine vitamin D levels in all FMS patients. Particular attention is needed towards the high-risk subpopulation, such as patients with multiple risk factors. FMS patients with VDD need immediate replenishment, and careful follow-up to avoid the impact of unwanted complications.