Given a previous review on emu oil from 2014, which concluded a lack of clinical trial evidence, these authors set out to summarize the literature with regard to emu oil use for non-specific pain management. Non-specific pain management was selected as Google Trend data suggest that emu oil may be commonly amongst the general population for the treatment of non-specific pain. Using PRISMA guidelines, three randomized, controlled trial studies were identified, which found either no statistically significant difference between emu oil and placebo for pain relief or used a compound, which made it impossible to state that emu oil by itself was responsible for pain reduction. Upon review, there is currently no clinical evidence that emu oil has a therapeutic benefit for the treatment of non-specific pain.
Topical, Pain management, Musculoskeletal, Emu oil
Emu oil has a medicinal history dating back to the native aboriginals of Australia, who used the oil to expedite wound healing and pain management [1]. While farmers had previously seen emus as a source of exotic meat for sale, using emu oil for its purported medicinal benefits has proven to be a boon for the emu farming industry since the late 1990s [2]. The large flightless native Australian bird is harvested for its fat deposits, which are then centrifuged and filtered to create purified emu oil for commercial distribution [1]. According to one publication in 2013, a single emu yields 250 ounces of oil, which may be sold for $10 an ounce [2].
Over the past two decades there has been a surge in interest associated with emu oil products [2]. A Google search for "emu oil" in 2010 returned 710,000 results, while a search in 2020 for "emu oil" produced 102,000,000 results - a 43% increase [3]. Despite an increase in revenue and general interest, there has yet to be a scientific study which successfully identifies the mechanism of action of emu oil [1]. Emu oil has been described in modern scientific literature for a wide spectrum of medicinal purposes, including but not limited to: Pain [1,3,4], wound care [1], bowel inflammation [5], vulvodynia [6], and chemotherapy induced mucositis [7]. Assessing the therapeutic effect of emu oil use is difficult, as studies must also account for variances in approach to the harvest, fat processing, cream storage, delivery method, and potentially even the diet of the emu from which it was harvested. Without a standardization of processing from emu to patient, one cannot reliably determine therapeutic benefit for specific medical indications.
Emu oil is not an FDA-approved medication [8]. There is no identifiable database of diagnoses for which emu oil is most commonly prescribed. To date, the most thorough review of evidence for emu oil benefit was published in 2014 and cited its potential application to mitigate the following conditions: Mucositis, inflammatory bowel disease, auricular inflammation, cancer chemotherapy-induced bone loss, adjuvant induced arthritis, hypercholesterolemic effects, skin and hair growth, moisturizing and cosmetic properties, wound care, and pain [1]. We used Google Trends data from 2016-2020 to compare each of these conditions, taking worldwide Internet searches as a surrogate for product usage amongst the general public. Results suggested that emu oil might be used most commonly for pain. Without the ability to further sub-type our search for specific types of pain given the limitations of Google Trends, our review sought to determine whether there is clinical trial evidence to support the use of emu oil for non-specific pain management.
This study was Institutional Review Board-exempt. The study was performed in accordance with the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Outcomes: Any scale that either subjectively measured pain or attempted to objectively measure pain. Pain must have been either a primary or secondary end-point measure in the study.
Studies: Randomized controlled clinical trials
We performed a systematic search for clinical trials involving emu oil for any indication published between 2008 and 2019 without language restriction. We elected to broadly investigate the medical literature, with knowledge from previous studies that the evidence base was likely to be minimal. Our intent was such that by including all emu oil clinical trials, we would be able to identify studies which used pain as a primary or secondary endpoint.
The search was performed using the filter "Therapy," general search term "emu oil," publication types "clinical trial" and "review," and medical subject headings (MeSH) "Humans". We searched PubMed, Cochrane Central Register of Controlled Trials, and Web of Knowledge. We also examined the reference lists of published studies, review articles, and meta-analyses to identify other eligible studies. Search results were confirmed by two individual independent reviewers. Internet searches concluded in December 2019.
Studies were initially assessed based on title and abstract for eligibility. Exclusion criteria during the initial screening process included: Publication of abstract only, reviews, and animal studies. Studies that appeared to meet criteria were selected for full text review. At the next level of screening, inclusion required that the clinical trial incorporated a pain measure as an endpoint or as a component of a scaled measurement tool.
Using PRISMA guidelines, thirteen studies were identified, none of which were removed due to duplication. Five articles were excluded on the basis of title or abstract. The remaining eight articles were assessed for eligibility-four were excluded because pain was not an outcome measure, and one was excluded due to lack of peer review. The final three studies were accepted for qualitative review [9-11] (Figure 1).
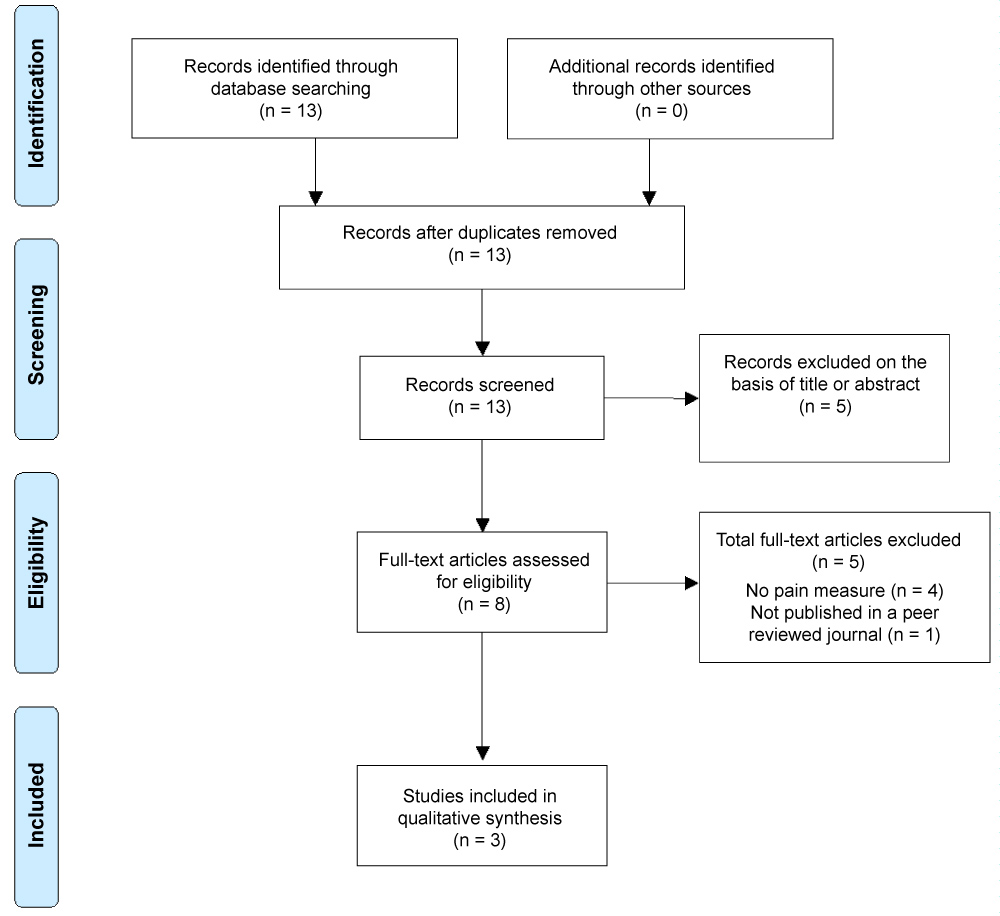 Figure 1: PRISMA flow diagram.
View Figure 1
Figure 1: PRISMA flow diagram.
View Figure 1
The first study was a double-blind, placebo-controlled trial that evaluated emu oil's effect on decreasing joint pain related to adjuvant aromatase inhibitor treatment in postmenopausal women with stage I to III breast cancer who were receiving aromatase inhibitor (AI) therapy for at least three months and had one to three joints with subjective worsening pain (a known side effect of AI therapy) [9]. Eighty-seven women met the inclusion criteria and were randomized to receive placebo oil or emu oil. Selected joints were treated with emu oil three times daily in specified amounts using a measuring device. Of the eighty-seven enrolled, fourteen ceased treatment within three weeks of registration due to a variety of reasons unrelated to toxicity of treatment. The primary outcome was subjective pain improvement as measured by the visual analog scale (VAS) and brief pain inventory (BPI) questionnaire. Baseline VAS and BPI scores were taken at the day of randomization and after eight weeks of therapy. The authors found that there was no statistical difference between the groups for joint pain by the VAS (p = 0.45) or by BPI (p = 0.76). This study appears to represent a common use for topical emu oil, at least anecdotally, with regards to joint pain. However, due to the specificity of the pathology reviewed, the results are generalizable only to that patient population.
Another study was a double-blind, placebo-controlled, single-site pilot study of adults with histologic evidence of breast cancer to assess "ultra emu oil" versus placebo in the prevention of radiation dermatitis in a cohort who were to undergo radiation therapy as part of their treatment plan [10]. Forty-five patients were enrolled and randomly selected to receive treatment with either emu oil or placebo (a cottonseed oil-based substance similar in consistency to emu oil). Three participants were unable to complete the study. The remaining forty-two participants were asked to use 1.5 mL of oil twice daily for the duration of radiation therapy and for the six weeks following radiation therapy. The primary outcome was dermatologic, but used the Skindex-16, which is an analog scale of symptoms and functional endpoints. The symptom subscale within the Skindex-16 assesses itching, burning or stinging, hurting, and irritation within its question set. In this study, the authors found that patient-reported Skindex-16 Area Under the Curve (AUC) scores, including each subscale score, tended to be lower in emu oil patients (AUC = 7.2) than in placebo patients (AUC = 10.4). However, this finding was not statistically significant (p = 0.29). Overall, quality of life was slightly better in the emu oil group, but again, not to a significant degree.
Finally, Twidwell and Levine performed a study to evaluate the safety and efficacy of a newly developed topical treatment for acute phase Peyronie's disease [11]. Called H-100, this compound consisted of nicardipine, superoxide dismutase, and emu oil. Participation criteria included patients with documented Peyronie's disease of less than twelve months duration, who had not used any treatment in the past six months and were able to get an erection without the use of a phosphodiesterase inhibitor. Twenty-two men were recruited and randomly assigned for treatment with either emu oil or placebo. Both groups received respective intervention for three months, after which all twenty-two men were treated for three additional months with H-100. Penile flaccid stretch length, penile curvature, and pain (using a VAS) were measured at monthly intervals. All participants completed the study. Pain was reduced in both groups, although more notably in the H-100 group. At three months, the H-100 group showed a statistically significant reduction in pain compared to baseline (p = 0.03) (Table 1).
Table 1: Quality appraisal. View Table 1
In the Rollman, et al. study on emu oil and radiation dermatitis, the Skindex-16 never directly uses pain as an endpoint [10]. It could be argued that the symptom subscale is synonymous with pain, as it asks participants to evaluate burning or stinging, hurting, and irritation, but pain is never specifically identified as the focus of study. Moreover, this study used a specific type of emu oil referenced as "ultra emu oil". It is unclear how this product differs from other emu oil products used in this review. Also of note, Twidwell's Peyronie's disease study used emu oil in a mixture with two other products, nicardipine and superoxide dismutase [11]. While pain scores were reduced, the independent effects of emu oil on pain relief cannot be determined, given the presence of two other chemically active ingredients in the compound.
While there may be specific populations for which there is evidence to support pain relief with topical emu oil, there currently appears to be no evidence in clinical trials to broadly conclude that emu oil has therapeutic benefit in the treatment of non-specific pain.
Disclosure Statement: There are no conflicts of interest to disclose on the part of any of the authors. There were no sources of financial support for this study.