Due to their osteopenic bone, specific fracture patterns involving the quadrilateral plate are very frequent in acetabular fractures in elderly patients. This has led to a growth in the use of both anterior intrapelvic (modified Stoppa) approach and infra and supra-pectineal quadrilateral buttress plates was seen in recent years.
All cases of acetabular fractures of patients aged > 65 treated with supra-pectineal quadrilateral buttress plate between 2015-2020 were retrospectively reviewed. Letournel classification was used and fracture reduction was classified according to Matta criteria in post-operative CT scans. The WOMAC Index e Harris Hip Score (HHS) were applied to assess functional outcome.
5 acetabular fractures in 5 male patients. A fall from standing height was the mechanism of injury in 4 of 5 patients. Anterior column was the most frequent fracture pattern (3/5) and gull sign was present in those 3 cases. Modified Stoppa was the most frequent used approach. Anatomic reduction was achieved in 2 patients, imperfect in 1 and poor in 2 patients. The mean HHS was 87.6 and the mean WOMAC index was 20.6.
Open reduction and internal fixation can provide good outcomes in elderly acetabular fractures when anatomic reduction is obtained. The modified Stoppa approach is useful as it provides better visualization and direct access to the quadrilateral plate. The supra-pectineal quadrilateral surface buttress plate allows for fixation of the anterior column along the pelvic brim and fixation to the medial surface of the posterior column providing a strong buttress to the quadrilateral surface.
Acetabular fractures, Quadrilateral plate, Modified stoppa, Suprapectineal buttress plate
With an aging population, the prevalence and burden of all osteopenic fractures is expected to continue to rise. Specifically, in patients over the age of sixty, there has been a 2.4-fold increase in the incidence of acetabular fractures over the past quarter of a century [1]. In this age group not only the patient conditions are different but also the mechanism of injury and fracture pattern differ from those of younger patients. Associated traumatic injuries are also less frequent. Low-energy falls from a standing height account for roughly half of the fractures [1]. Osteopenic patients who fall on their side experience an impact through the greater trochanter, which results in a superomedial vector force. This mechanism results in anterior column displacement, quadrilateral plate involvement, medialization of the femoral head, and superomedial roof impaction, which creates the so-called gull sign on an anteroposterior pelvic radiograph [2]. This mechanism of injury is the reason why in this age group, and accordingly to Letournel classification [3], associated both-column and fractures involving the anterior column (anterior column-posterior hemitransverse and isolated anterior column) are the most common fracture patterns [4].
Elderly patients with an acetabular fracture should be treated as any other older patient with a fragility fracture of the hip. Operative reduction and stabilization of displaced acetabular fractures are now considered the accepted treatment for these injuries to decrease the risk of posttraumatic arthritis, allow early mobilization and improve functional outcome. Standard methods of fixation include combinations of pelvic reconstruction plates and lag screws applied to the anterior and posterior columns from either an anterior and/or posterior approach [5].
The involvement of the quadrilateral plate has been considered as an important factor contributing to the complexity of surgical reconstruction of acetabular fractures [6,7]. To address the challenge of reduction and fixation of this specific anatomic area advances in surgical approaches, namely anterior intrapelvic (modified Stoppa) approach, and implants have been developed and the use of quadrilateral surface buttress plate has grown. Nevertheless, few and mainly retrospective studies with limited number of patients are available in the literature.
The objective of this retrospective case series was to evaluate the short-term clinical and radiological outcome of supra-pectineal quadrilateral surface buttress plating in the treatment of acetabular fractures with quadrilateral surface involvement.
The trauma registry of our institution was retrospectively reviewed for all acetabular fractures in > 65-years-old patients with quadrilateral plate involvement that were treated with open reduction and internal fixation with supra-pectineal quadrilateral surface buttress plate from 2015 till 2019 and had a minimum follow-up time of 1 year. Institutional board review was obtained for this study.
5 patients were included in the study. Patient demographics including age, sex, and mechanism of injury were documented. Concomitant injuries, temporary treatment, time to operating theatre for the acetabular reconstruction, surgical approach, surgery time, estimated blood loss and early and late complications, were collected. In February 2020 all patient were clinically evaluated and the Western Ontario and McMaster Universities Arthritis (WOMAC) Index and the Harris Hip Score were applied irrespective of post-operative time.
Two orthopaedic trauma surgeons reviewed and classified the fractures using pre-operative pelvic and acetabular radiographs and CT scans, according to the Letournel classification. The presence of the gull sign, which represents osteopenic superomedial roof impaction by femoral head medialization as describe by Anglen, et al. [8], was also documented and the fracture was characterized as either demonstrating this feature or not. Fracture reduction was classified accordingly to Matta criteria on post-operative CT-scans: Residual gap and step displacement were measured along the articular surface at the level of the weight-bearing dome seen at the three planes (coronal, sagittal or axial) and was recorded in millimeters, and the highest of the three values was used to grade the reduction according to one of three categories: Anatomical (0-1 millimeter (mm) of displacement), imperfect (2-3 mm) or poor (> 3 mm) [9-11].
Open reduction and internal fixation was performed by the same senior trauma surgeon. Patients where operated on supine position for anterior intrapelvic (modified Stoppa) and ilioinguinal approaches. In one case a Kocher Langenbeck approach was also used after an ilioinguinal approach and the patient was positioned in lateral decubitus. Femoral skeletal pin traction and proximal femur lateral pin traction were used to assist reduction as needed. After open reduction, internal fixation was achieved using a supra-pectineal plate from the Matta Pro Plating System (SPS Matta Pro Pelvis and Acetabulum System, Stryker).
Post-operative mobilization protocol consisted of immediate toe touch weight bearing (up to 6 weeks), followed by partial weight bearing (6-12 weeks), and full weight bearing thereafter. Physiotherapy included gait training and quadriceps/abductor strengthening exercises starting immediately postoperatively. Range of motion exercises were added at six weeks post-operatively. Chemical (enoxaparin 0.5 mg/kg/day) thromboprophylaxis was given for six weeks. Outpatient follow-up included clinical and radiological review.
5 patients were included in the study. Table 1 resumes the information regarding each patient. All patients were male, the mean age was 68.8 years (65-76 years), mean follow-up time was 18.6 months (12-39 months). 4 patients had left acetabular fracture and 1 right acetabular fracture. A fall from standing height was the mechanism of injury in 4 of 5 patients; anterior column was the most frequent fracture pattern (3/5) and the gull sign was present in those 3 cases. Modified Stoppa was the most frequent used approach. Anatomic reduction (< 1 mm) was achieved in 2 patients, imperfect reduction (2-3) in 1 and poor reduction (> 3 mm) in 2 patients which required a total hip arthroplasty for symptomatic hip osteoarthritis at 1 year follow-up. Cement was needed in plate pubic screws to augment bone purchase in 1 patient. All patients were able to walk without support after rehabilitation. The mean HHS was 87.6 (77-95) and the mean WOMAC index was 20.6 (14-42) (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, Figure 9 and Figure 10).
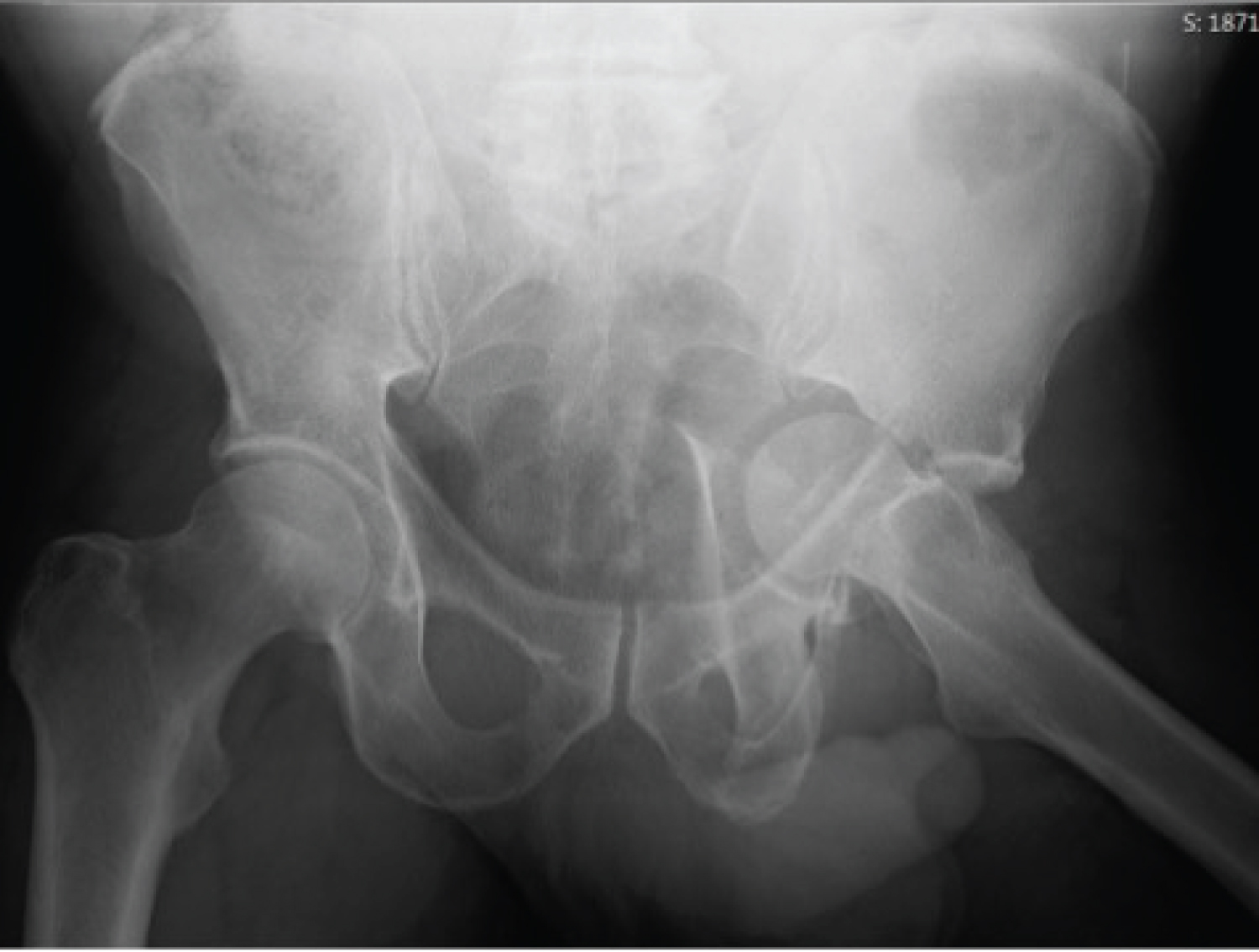 Figure 1: Case 1 admission AP pelvis X-ray. View Figure 1
Figure 1: Case 1 admission AP pelvis X-ray. View Figure 1
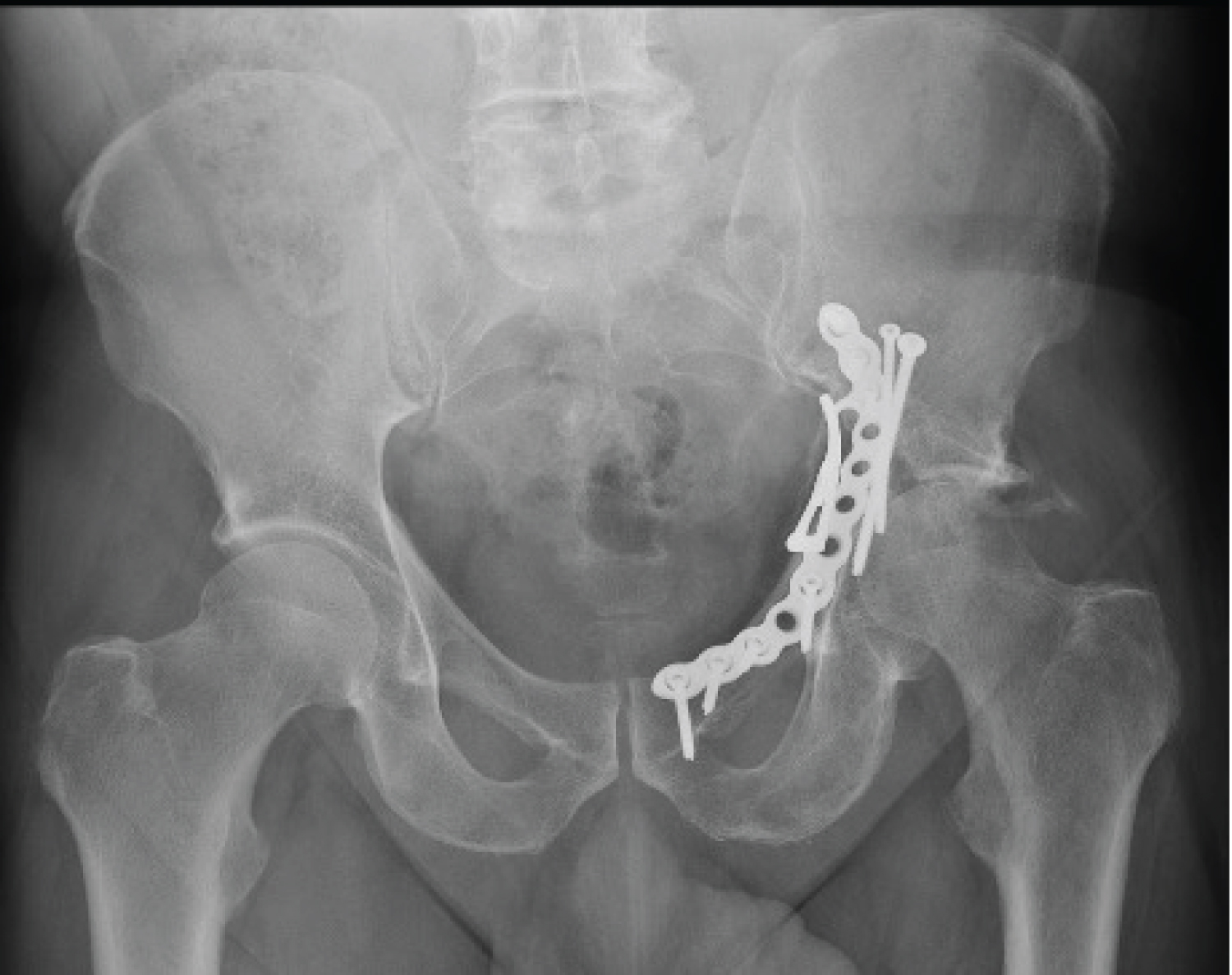 Figure 2: Case 1 post-operative AP pelvis X-ray. View Figure 2
Figure 2: Case 1 post-operative AP pelvis X-ray. View Figure 2
 Figure 3: Case 2 admission AP pelvis X-ray. View Figure 3
Figure 3: Case 2 admission AP pelvis X-ray. View Figure 3
 Figure 4: Case 2 post-operative AP pelvis X-ray. View Figure 4
Figure 4: Case 2 post-operative AP pelvis X-ray. View Figure 4
 Figure 5: Case 3 admission AP pelvis X-ray. View Figure 5
Figure 5: Case 3 admission AP pelvis X-ray. View Figure 5
 Figure 6: Case 3 post-operative AP pelvis X-ray. View Figure 6
Figure 6: Case 3 post-operative AP pelvis X-ray. View Figure 6
 Figure 7: Case 4 admission AP pelvis X-ray. View Figure 7
Figure 7: Case 4 admission AP pelvis X-ray. View Figure 7
 Figure 8: Case 4 post-operative AP pelvis X-ray. View Figure 8
Figure 8: Case 4 post-operative AP pelvis X-ray. View Figure 8
 Figure 9: Case 5 admission AP pelvis X-ray. View Figure 9
Figure 9: Case 5 admission AP pelvis X-ray. View Figure 9
 Figure 10: Case 5 post-operative AP pelvis X-ray. View Figure 10
Figure 10: Case 5 post-operative AP pelvis X-ray. View Figure 10
Table 1: Resume of case information. View Table 1
In our cases the patients with a poor reduction (> 3 mm) in post-operative CT developed early symptomatic osteoarthritis with the need for THA at 1 year follow-up. These two patients also presented the higher magnitude of dislocation of femoral head at initial X-ray and one of them, Case 4, was also the case which waited 36h for closed reduction and skeletal traction, on the other hand Case 1 was the case in which the hip was reduced 2 h 30 m after hospital admission. The Gull sign was present in 3 patients but all 3 had different grades of reduction success. Functional outcomes were good, especially in those with anatomical reduction (< 1 mm).
With an aging population, the prevalence of fragility acetabular fractures is expected to continue to rise. In the elderly, low-energy falls from a standing height account for roughly half of the fractures [1]. Even though associated traumatic injuries are less frequent, due to poor bone quality these falls often result in complex acetabular fractures in patients with poor overall health status but crescent functional demands; a grueling combination the treating surgeon must deal with.
Letournel classification [3] describes acetabular fracture patterns typical of high energy trauma involving patients with normal bone quality: That's why it's not always easy to apply it in this subset of patients, in fact, the study published by Herman, et al. classifies acetabular fractures based on injury mechanism vector, theses fractures would be included in the superomedial displacement vector group [12].
Historically, the nonoperative management of geriatric acetabular fractures has yielded poor results. In the past, reductions were attempted via lateral trochanteric or longitudinal skeletal traction and prolonged bed rest. Nowadays we know the prolonged bed rest has a high morbidity and mortality associated and also the cumulative experience has showed that good to excellent outcome can be achieved with surgical treatment [4]. Therefore, conservative treatment should be reserved for patient with < 2 mm of displacement, an intact roof arc angle of 45°, superior 10 mm of the subchondral ring intact on CT, posterior wall fractures involving < 20% of the posterior wall, hip joint stability and congruity, and an absence of the poor radiographic prognostic factors, which include: Posterior wall comminution, marginal impaction, gull sign, hip dislocation, impaction injuries to the femoral head, femoral head or neck fractures, and preexisting arthritic changes [8,13,14]. Patients who are medically unfit for surgery, functionally incapacitated or present with a both-column fracture pattern that exhibit the so-called secondary congruence in which femoral head acts as a template for the osteochondral fragment to settle which may provide acceptable functional outcomes specially for low-demand patient are also indications for conservative treatment [15].
The purpose of acetabular fracture reduction and fixation is to allow early, pain-free mobility and mitigate the potential for posttraumatic arthritis by anatomically reducing the articular surface. As reported by Matta [9]. Achieving a reduction with < 3 mm of intra-articular incongruity is key to obtaining a good clinical result in all acetabular fractures. This is harder in older patients when compared to young ones, so is mandatory to consider whether an acceptable reduction can be achieved and whether bone quality is sufficient for the implants purchase to sustain articular reduction before deciding on treatment. Factors affecting the survival of the native hip should also be considered when choosing treatment options. In their series of 816 acetabular fractures followed over twenty-two years, Tannast, et al. revealed that an age of greater than forty years, anterior dislocation, posterior wall involvement, femoral head cartilage impaction fractures, marginal impaction, acetabular impaction, and initial articular displacement of > 2 cm were correlated with a future need for total hip arthroplasty [16,17]. In this situation ad minimum surgical aggression to prepare for future arthroplasty is a comprehensible strategy.
The choice of surgical approach is important to allow for good fracture visualization and fixation. Fracture pattern involving the anterior column may be approached via an ilioinguinal or modified Stoppa approaches, while those involving the posterior wall or isolated posterior column are preferably treated using a Kocher-Langenbeck approach. In geriatric population, as stated previously, fractures usually involve the anterior column and displacement of the quadrilateral plate. In this setting the modified Stoppa approach, provides direct access and visualization of these fragments, specially the quadrilateral plate, for reduction and fixation contrary to the ilioinguinal approach [18,19]. The Stoppa approach is also less invasive and associated with less blood loss, as our cases exemplify, the most important limitation in its use being the learning curve and noble structures identified during this approach. Dual approaches may also be needed in cases of complex fractures involving the two columns. In cases of acute total hip arthroplasty (THA) an ilioinguinal or modified Stoppa approach for fracture fixation can be combined with a Kocher-Langenbeck approach for hip repositioning and total hip arthroplasty [14].
Fixation in elderly acetabular fractures is difficult due to poor bone quality, atypical fracture pattern, superomedial roof impaction, bone comminution and quadrilateral plate involvement that characterize acetabular fractures in this age group. The quadrilateral plate forms the medial wall of the acetabulum so the inability to achieve a solid and reliable fixation will eventually lead to loss of reduction and medial subluxation of the femoral head, which is not an uncommon occurrences in these circumstances as stated in the older literature where quadrilateral plate buttress often resulted in late displacement [20].
Regarding this technical problem, recent advances in acetabular fracture surgery aimed to create solutions for the demands posed by an aging osteoporotic patient population. Results have improved mainly due to two factors: Wider use of the modified Stoppa approach and the development of infra and supra-pectineal quadrilateral surface buttress plates which provide a buttress to the quadrilateral surface and prevent medial subluxation of the femoral head and allow for fixation of the anterior column along the pelvic brim and fixation to the medial surface of the posterior column spanning both columns [6]. Biomechanical studies showed that final stiffness after cyclical loading and resistance to medial subluxation with plates that span the columns and provide quadrilateral surface buttressing were comparable to or better than traditional fixation constructs [12,20].
The major limitations of this retrospective case series are: the small case number and heterogeneity between patients. More cases would allow us to study the relation between the initial aggression to the articular surfaces, higher in the dislocations cases, the time to hip reduction and temporary stabilization and the reduction quality - with the development of symptomatic osteoarthrosis and need for THA.
Acetabular fractures in the elderly are becoming increasingly common. In this age they are often the result of standing height fall and are associated with anterior column displacement, quadrilateral plate involvement, medialization of the femoral head, and superomedial roof impaction. Open reduction and internal fixation can provide good outcomes when a concentric, congruent and anatomic joint reduction is obtained. However, there remains a high conversion rate to total hip arthroplasty. The modified Stoppa approach is especially useful in this subset of patients as it is less invasive than the traditional approaches and provides better visualization and direct access to the quadrilateral plate fracture fragments improving their reduction and fixation.
The infra and supra-pectineal quadrilateral surface buttress plates maximize the advantages of the modified Stoppa approach as they allow for fixation of the anterior column along the pelvic brim and fixation to the medial surface of the posterior column spanning both columns which provide a biomechanically strong buttress to the quadrilateral surface and medial subluxation of the femoral head allowing for anatomic reduction and consolidation and preventing protusio acetabuli in cases of poor reduction and delayed total hip arthroplasty.
No funding was received to assist with the preparation of this manuscript.
On behalf of the all authors, the corresponding author states that there is no conflict of interest.