Leg length discrepancy (LLD) and pelvic obliquity have often been associated with scoliosis in the literature, and neuromuscular contributions have been mentioned as being possibly involved. It is herein hypothesized that a craniocervical junction (CCJ) misalignment (CCJM) may induce a neuromuscular imbalance leading to functional leg length discrepancy, and that re-establishing a proper alignment can result in some LLD disappearance.
A total of n = 40 consecutive scoliotic children aged 7-16 years, 15-50 Cobb angle, were followed for a mean period of 16 months. Children presenting signs and symptoms of CCJM were evaluated with specific radiographs. Patients for whom the misalignment was confirmed received a CCJ adjustment for their realignment.
All patients presented at first LLD and CCJM. From a mean LLD of 11.0 mm at first presentation (Pre), there was a mean 90% reduction of LLD at the first follow-up visit (1.1 mm) after the realignment (mean 15 days Post), and the mean LLD during the complete follow-up period (2.0 mm) was 82% less than that of the mean Pre-LLD, with a mean yearly 1.2 CCJM recurrences and treatments per patient.
The results suggest an association between LLD and CCJM among scoliotic children, and LLD may be reversed by means of a CCJ realignment which can be sustained. Occasional CCJM recurrences were typically due to falls or hits. The LLD were measured in a horizontal position. It is likely that in a vertical gravitational position, forcing the feet even on the ground, these neuromuscular imbalance forces responsible for this LLD would not disappear but translate into other pelvic and spinal compensatory deviations that may possibly contribute to the development of scoliosis.
Anisomelia, Pelvic tilt, Upper cervical, Atlas, Posture
Leg length discrepancy (LLD) is considered a common sign of craniocervical junction (CCJ) misalignment (CCJM) or malalignment among upper cervical (UC) practitioner community which believe that a CCJM can result in some compensatory neuromuscular imbalance affecting the musculoskeletal structures of the whole body, including the spine, pelvis and legs. The presence of LLD along with different other clinical signs and symptoms described below may suggest the presence of CCJM, also called upper cervical misalignment (UCM) or occipito-atlanto-axial misalignment, defined as a subtle relative displacement of the components of this complex (i.e. occipital base, atlas and axis, or C0-C1-C2). The presence of CCJM can be confirmed with specific radiographs obtained at an incidence optimizing the visualization of the craniocervical articulations. It is herein hypothesized that CCJM may induce a neuromuscular imbalance leading to functional LLD, and that re-establishing a proper CCJ alignment can result in some disappearance of this LLD. The primary objective of this article is to evaluate the co-occurrence of LLD and CCJM among pediatric scoliotic patients, and the second objective is to evaluate the effect upon functional LLD of re-establishing a proper CCJ alignment.
Leg length discrepancy, difference, disparity or inequality, also called anisomelia, limb length discrepancy or apparent leg length difference, can be divided in two categories, either structural (also called true or anatomic) or functional. Structural LLD (SLLD) can be defined as a bilateral difference of the osseous length of the legs (femoral + tibial lengths), whereas functional leg length discrepancy (FLLD) can be defined as the overall observed LLD, but excluding the structural LLD contribution. Regardless of whether the LLD is structural or functional, the mechanical effects on the kinetic chain are potentially the same for either [1].
LLD has often been associated with pelvic tilt, also called pelvic list or obliquity, which may lead to pronounced compensatory spinal deviations and scoliosis [2-6] that with time may become structural [6,7]. Innominate rotation inevitably brings about a tilted sacrum, and an uneven sacral base results in a compensatory lateral curve of the spine [8]. Pelvic obliquity and rotation are the most common methods of compensating for LLD [9-12]. LLD is also often compensated by external rotation and pronation of the foot on the side of the long leg, and supination and/or plantar flexion on the contralateral side [4,13,14]. Although pelvic tilt may be compensatory from LLD, the rotation of the pelvis due to suprapelvic muscular abnormal tonicity can generate functional LLD [15]. LLD and pelvic tilt may have a two-way cause to effect association.
Either structural or functional, LLD affects hip joints, joints posture and weight bearing, and is associated with pelvic tilt and rotation [7,8,16,17]. LLD is also favorable to chronic hip and low-back pain [7,16], headache and dizziness [8], stress fracture [4,7,18], muscle spasm, asymmetrical activation and tonus, fatigue and pain [4,7,16]. LLD may result in sciatica and paresis by means of the entrapment of the sciatic nerve [17] that can be caused by the protrusion of the asymmetrically loaded vertebral disc from the intervertebral space and impinge on the sciatic nerve [19]. LLD may also hamper the normal gait and energy consumption, and subjects the lumbar segments to constantly repeated asymmetrical bending, torsion and axial rotation known to be the most damaging load to the disc [7,20,21].
The examination for LLD in an unloaded position is commonly used as a sign of neuromuscular dysfunction [15,22,23]. The patient stands up on a horizontal step that is fixed to a vertical mat table to which the patient sticks and holds the two side handles. The device is equipped with an electro-hydraulic system that allows for the mat table, step and the standing still patient to pivot slowly from the vertical gravitational position to an unloaded horizontal position, therefore standardizing the positioning of the patient. The step slowly withdraws gradually during the mat table rotation procedure. The still patient is not touched or forced anyhow during and after his rotation process with the mat table until the LLD is measured, not to interfere with the natural positioning of the patient and measurements. Once the patient is in the horizontal position, the legs are stable and difficult to move in their longitudinal axis, as the displacement of the legs would require some displacement of the hips and trunk mass.
The LLD is measured as the distance between the two heels along the leg longitudinal axis in either a prone or supine unloaded position, providing consistency of the method used.
This LLD value does incorporate both SLLD and FLLD contributions and has the advantage of being simple, involves no radiation, does not depend on the perception of the pelvis level, is at low cost and does not require any specific anatomical landmark identification, therefore minimizing the error.
Although the FLLD and SLLD contributions may be difficult to separate from the overall LLD, the difference of the overall LLD before and after an UC realignment (UCR) of the CCJ is clearly entirely functional. The efficacy of the UCR treatment can be appreciated in the difference of LLD before and just after the treatment.
The objective of this paper is not to validate the precise upper cervical adjustment (PUCA) as a realignment treatment, but to utilize it to demonstrate that UCM may involve some neuromuscular imbalance leading to an asymmetrical contraction of muscles involved in the posture and FLLD, and that it can be reversible.
The description of the UC technique (UCT) is beyond the scope of this article, however, a summary of the UCT, the PUCA treatment and its background, along with the different approaches and branches of the UCT, can be found in the literature [22]. A more extended and complete review of the UC complex and its misalignment, called subluxation among UC practitioners, has also been previously presented [23].
Briefly, the UCT and its PUCA treatment are based on the B.J. Palmer (1881-1961) principles in which a CCJM is responsible for some neurological disturbance leading to compensatory neuromuscular imbalance that can affect the posture of the whole body [10,22,23]. The realignment is performed by means of a soft and short (milliseconds) manual adjustment (not a manipulation) of the lying down patient's misaligned UC vertebrae.
The adjustment of the UCT truly differentiates from standard chiropractic manipulation, knowledge and principles in that it does entail neither bone articular cavitation (cracking) nor neck rotation/torsion (twisting), and softly interacts only with the CCJ to reverse the neuromuscular imbalance instead of interacting where the pain or deviations are, considering that the postural anomalies elsewhere in the body are compensatory to the culprit CCJM.
A total of n = 40 consecutive pediatric patients, including 8 males (20%) and 32 females (80%), aged 7 to 16 years, presenting at the clinic with scoliosis from 15 to 50 Cobb angle, were evaluated for their LLD along with signs and symptoms of UCM, and followed for a period of at least 2 months including a minimum of 5 follow-up (FU) visits. The presence of syndrome was an exclusion criterion. All data of the patients were included up to the writing of this article, or until the end of their FU period defined as a complete lack of FU visit for a period of at least 4 consecutive months.
This article contains some preliminary sub data on LLD obtained from an ongoing study about juvenile and adolescent idiopathic scoliosis occipito-atlanto-axial neuro-biomechanics (JAISON) that investigates the effect on pediatric idiopathic scoliosis arising from UCR treatment, and which received the approval of the Ethic Board of the McGill University Faculty of Medicine. However, the relation between scoliosis deformations and UCR is beyond the scope of this article. The radiology of the CCJ was acquired at the first visit for patients presenting signs and symptoms suggesting the presence of an UCM. Patients diagnosed with UCM received a PUCA treatment on a horizontal drop piece adjustment table (Zenith-Palmer-Thomson Specific Headpiece Mfg, IL USA) to re-establish a proper alignment (realignment) of their UC complex (UCR treatment).
Complete examination for signs and symptoms of UCM was performed at each FU visit, namely including the assessment of LLD in an unloaded prone position with a rotative mat table (Zenith Hi Lo, Williams Mfg, IL USA), bilateral thermography differential of the full spine (Titronics, Tytron C-5000, IA USA) and bilateral mastoid fossa temperature differential (Braun Thermoscan Irt-6520, MA USA), pelvic obliquity, and neck and shoulders obliquity (LLOYD table company IO USA). Transparent leg check shoes measuring device were placed (strapped) under each foot, and a scale printed on them allowed for the measurement of their bilateral offset (i.e. LLD) in the leg longitudinal axis. The LLD values were originally measured with devices using the imperial system (inch, abbreviated by the quotation mark) with a 1/8" (0.13" = 3.2 mm) increment. All values were rounded to the nearest increment and converted in millimeters (1" = 25.4 mm).
Children presenting at first with UCM received a PUCA treatment. This UCR was performed one time at the beginning (t = 0) of their FU period. A subsequent UCR was however repeated if ever the child presented evidence of an UCM recurrence along the FU period, in which case the child and family were asked if they could associate the UCM recurrence to any specific causative reason and its date, like a fall, an impact, or an unusual activity or event. The LLD were systematically measured before and just after any UCR to appreciate the effectiveness of the treatment.
Variables are presented as mean ± standard deviation, along with the 95% confidence interval (CI) for the mean. Measures of LLD collected before and after treatment were compared using paired t-test, while mean LLD at follow-up (1st FU and overall FU) were compared to the threshold of 3.2 mm (1/8") using a Student's t-test. Normality and assumptions were verified. Two-tailed p values of < 0.05 were considered statistically significant. Statistical analyses were performed using SAS version 9.4 software (SAS Institute Inc., Cary, North Carolina).
The mean FU period was 16 months (475 days ± 282) and involved 818 visits during which 66 recurrences of UCM and treatments were performed, and the mean lapse of time between two FU visits was three weeks (23 days).
The first observation from the results is that all pediatric scoliotic patients presented at first (Pre) some level of LLD, ranging from 6.4 to 15.9 mm. The mean Pre-LLD was 11.0 mm with a standard deviation (STD) of ± 2.8 mm (95% CI: (10.2, 11.9 mm)).
The second observation is that all patients also presented at first with pelvic tilt and bilateral temperature differential of the full spine (including cervical) and at the level of the mastoid fossa, along with a combination of other aforementioned signs and symptoms associated with UCM. Proper UC radiographs confirmed the diagnosis of UCM for all patients. Therefore, all patients of the cohort presented at first with some level of UCM and received a PUCA treatment for their UCR.
The third observation is that all patients demonstrated some decrease, and in most cases a complete disappearance, of their LLD just after their first UCR. From a mean Pre-LLD of 11.0 mm ± 2.8 mm, the mean LLD at the first FU visit (mean 15 days after the original UCR) was 1.1 mm ± 2.5 mm (95% CI: (0.3, 2.0 mm)), which represents a mean overall 90% ± 25% LLD reduction (95% CI: (81, 97%)) as compared to the mean Pre-LLD (p < 0.0001 for the comparison of mean Pre-LLD versus mean first FU LLD). The mean LLD at the first FU visit is significantly lesser than the threshold of 3.2 mm (p < 0.0001).
The fourth observation is that the LLD reduction was generally sustained during the FU period despite some occasional recurrence of UCM that were typically associated with small punctual traumatic events. From a mean Pre-LLD of 11.0 mm ± 2.8 mm, the overall mean LLD for all patients during their full FU period was 2.0 mm ± 1.8 mm (95% CI: (1.5, 2.5 mm)), which represents a mean LLD reduction of 82% ± 18% (95% CI: (75, 87%)) as compared to the mean Pre-LLD (p < 0.0001 for the comparison of mean Pre-LLD versus mean full FU LLD). The mean LLD for the full FU is significantly lesser than the threshold of 3.2 mm (p = 0.0004).
All patients presented at first (Pre) with LLD, with a mean value of 11.0 mm (mean 3/8", 1/4" to 5/8"). Therefore, there was an association between scoliosis and LLD, in accordance with a compelling body of literature [2-6,24]. All patients were diagnosed with UCM and received a PUCA treatment for their UCR. Therefore, the condition of these scoliotic children was associated with UCM. All patients but one (n = 39 over 40) demonstrated some decrease if not a complete disappearance of their LLD at the first FU visit (mean 15 days after) with a mean 90% LLD reduction. Therefore, UCR was associated with a regression of FLLD. Also is worth mentioning that the mean 90% LLD reduction at the first FU visit suggests that functional LLD was predominant over structural LLD, as previously reported [2]. There was an overall mean LLD reduction of 82% as compared to the mean Pre-LLD along the course of the FU period (mean 16 months FU), therefore suggesting that the LLD reduction from an UCR may be sustained, although some UCM recurrence and consequent LLD may happen.
Also, a point of interest is that at the first FU visit, 75% of all patients had a zero LLD (i.e.100% LLD reduction), and 20% of all patients had only 3.2 mm (1/8") LLD. Therefore, 95% of all patients had a LLD of either zero or 3.2 mm at the first FU visit as compared to a mean Pre-LLD of 11.0 mm. To be noted that a LLD value of 3.2 mm (one increment value, i.e. 1/8") was clinically considered as an absence of LLD sign. The authors believe that this arbitrary threshold corresponds to a value under which there is no considerable consequence, is frequently observed, may happen without the presence of significant CCJM, does not justify any intervention and is near the precision of the measurements. LLD over this threshold value may however cause distinct gait and posture disorders [3].
From the remaining 5% of the patients (i.e. 2 patients), one patient had an increase from a Pre-LLD of 9.5 mm (3/8th inch) to a LLD of 12.7 mm (1/2") at the first FU visit, due to slipping on the wet floor and falling on the hips when getting out of the pool the day before that first FU visit. This LLD thereafter decreased to 3.2 mm (1/8") at the second FU visit. The second patient that did not reach a LLD of either zero or 3.2 mm (1/8") at the first FU visit had a reduction from a Pre-LLD of 12.7 mm (1/2") to a LLD of 6.4 mm (1/4") at the first FU visit, and then reached a LLD of 3.2 mm (1/8") at the second FU visit. Therefore, again from a mean Pre-LLD of 11.0 mm (3/8"), 100% of all patients reached a LLD of zero or 3.2 mm (1/8") either at the first or second FU visit and were clinically considered as having no sign of LLD.
The following Figure 1 illustrates the mean LLD of all patients at first presentation, first FU visit, and whole FU period. The mean LLD along the FU period is slightly higher than the mean LLD at the first FU visit (2.0 mm vs. 1.1 mm) because a patient is more likely to have an UCM recurrence along his whole FU period (mean 16 months) than between the original UCR and the first FU visit (mean 15 days).
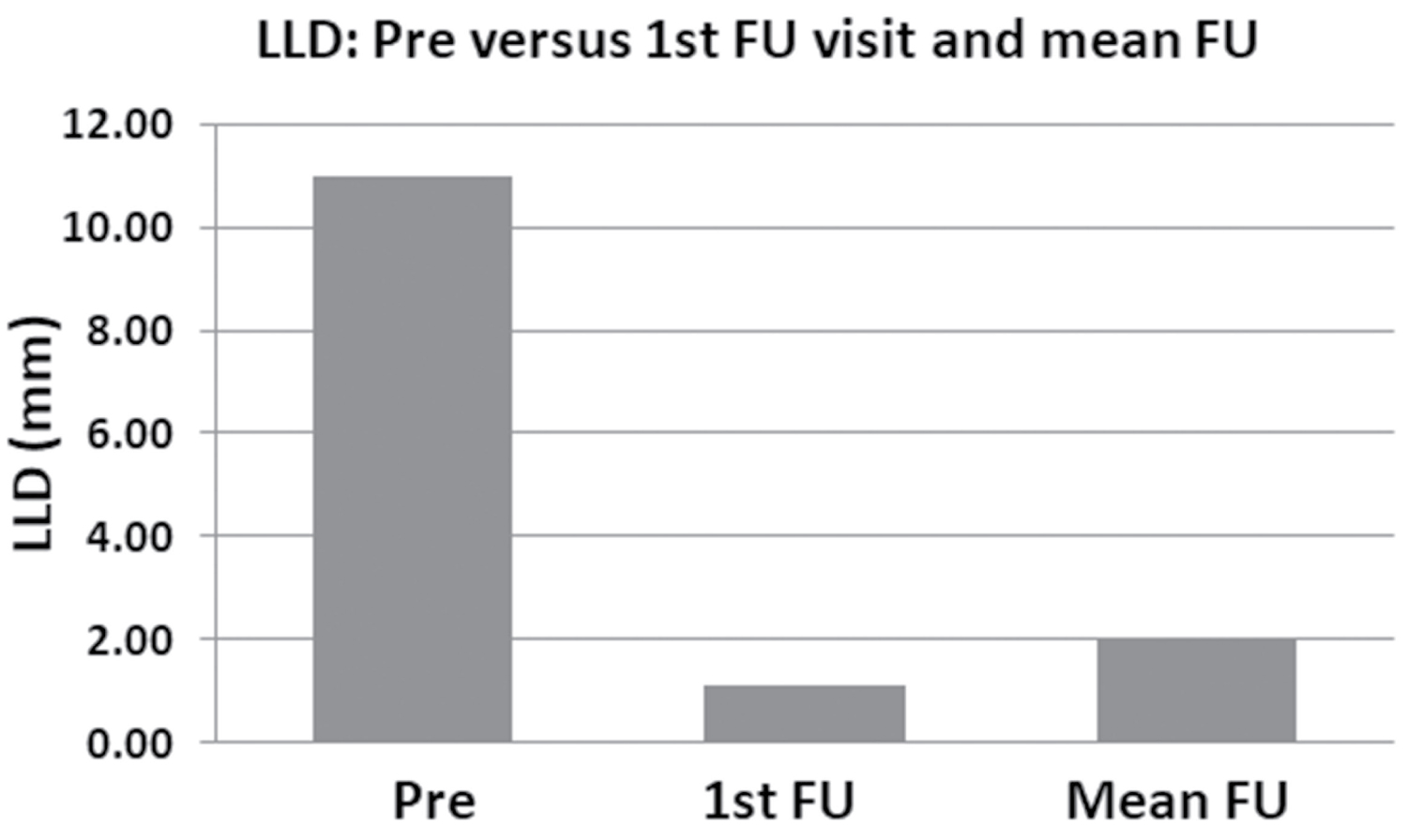 Figure 1: Left bar: Illustration of the mean LLD upon first presentation of all patients just before the original UCR treatment (Pre). Center bar: Mean LLD of all patients at the first follow-up (FU) visit (mean 15 days after the original UCR). Right bar: Mean LLD of all patients during the whole FU period (mean FU of 16 months).
View Figure 1
Figure 1: Left bar: Illustration of the mean LLD upon first presentation of all patients just before the original UCR treatment (Pre). Center bar: Mean LLD of all patients at the first follow-up (FU) visit (mean 15 days after the original UCR). Right bar: Mean LLD of all patients during the whole FU period (mean FU of 16 months).
View Figure 1
Although the UCR performed at the beginning of the FU period can be sustained, the UCM may re-appear for some reason, in which case a realignment procedure was performed (UCR). During the FU visits, the presence of LLD over 3.2 mm (1/8") must be accompanied namely with pelvic obliquity, along with bilateral temperature differential of the full spine and mastoid fossa to justify an UCR. Cervical radiographs were acquired only when a child presented for the first time with signs and symptoms of a UCM. During the follow-up (FU) period, the presence namely of the above-mentioned signs and symptoms of an UCM recurrence was considered sufficient to justify an UCR, without additional cervical radiographs to minimize the radiation dose absorption, in accordance with the ALARA (As Low As Reasonably Achievable) ionizing radiation protection principles and Ethics.
The number of UCM recurrences (i.e. excluding the first UCR) was counted for each patient and normalized to obtain an equivalent mean value of recurrence per one full year of FU period. The mean number of UCM recurrence/year for the cohort was 1.2 (± 1.6) UCR/year, meaning an average UCM recurrence and treatment per patient every 10 months. Interestingly, 43% of the patients did not experience any UCM recurrence at all during their whole FU period (mean 16 months). Also, 25% of the patients had only one UCM (and UCR) recurrence along their whole FU period. Therefore, the 2/3rd (68%) of all patients had either no or a single UCM (and UCR) recurrence during their whole FU period, which suggests that the UCR can be sustained. On the other hand, 10% of the patients (i.e. 4 patients) contributed to 40% of all UCM (and UCR) recurrences.
The recurrence of UCM may be caused typically by static or dynamic forces, bad movement or position, that may be of a large amplitude and occur once (punctual event), or of a smaller amplitude but repetitive. The recurrence of UCM can also be favored by some level of intrinsic ligamentous laxity, as in patients with Marfan syndrome for instance [24], or anatomic anomalies resulting in some instability of the CCJ, or simply being more recurrent among children that are more active, practice sports or activities at risk of weight bearing, jump, fall, shake and hit, or that are simply more "daredevil".
Roughly, for one half of the UCM recurrences, no cause was elicited from the information provided from the family. However, for the other half, the first three causes reported were a fall (38%), especially on the buttocks and the hips, followed by gymnastic/physical-education (21%) and a hit (20%). They were frequently accompanied with pain and sometime with fractures (elbow, ankle or wrist).
The reported culprit fall, hit or shake responsible for an UCM recurrence would, namely, be caused by sports (hockey, soccer, roller skate, ice skating, ski, and ball games), gymnastic (all kind of gymnastic at large including physical education courses at school, cheerleader dancing, long jump, trampoline and circus gym), accidental fall (in the stairs, from a treadmill exerciser, slip on the ice or on the wet floor by the pool, and fall from a tree branch or a hammock), leisure activities (water slide, dancing, jumping, snow sled and roller coaster ride), a hit (direct or indirect hit on the head, neck or shoulders, pushed by someone, pushed on a post, a tree or a wall, and hit from a ball or an object), or an impact (car collision and dodgem bumper car).
The Figure 2 represents examples of the effect on LLD from UCM recurrence following some of the above-mentioned causes. Interestingly, although the FLLD may disappear rapidly after an UCR, one patient maintained an equal and constant small LLD of 3.2 mm (1/8") along her FU period, as illustrated in Figure 2d, suggesting the presence of a SLLD (anatomic). She maintained this residual LLD at 16 FU visits over a total of 20 visits during a 13½ months (413 days) FU period and never reached a zero LLD.
 Figure 2: All bar values in this Figure 2 were shifted of + 0.5 mm (1/50th inch), otherwise zero values would have shown no bar. All LLD between zero and 3.2 mm (1/8") inclusively (i.e. here 3.7 mm with the shift, dotted line), were clinically considered as an absence of LLD sign. The abscissa indicates the number of follow-up days including the Pre visit (before UCR), and the ordinate indicates the LLD (maximum at 18.0 mm (0.7" ≃ 3/4") (a) Effect on LLD of a fall on the buttocks during a treadmill session; (b) Effect on LLD of a fall on the buttocks in the stairs. Two UCR were necessary (4 days interval) to reverse the 12.7 mm (1/2") LLD; (c) Effect on LLD of a hit on the hips during a hockey game; (d) Equal and constant small residual LLD of 3.2 mm (1/8") along the FU period, suggesting the presence of an anatomic LLD. Also of interest is the 12.7 mm (1/2") LLD caused by hitting a wall during physical education at school (left arrow), and falling on the buttocks while roller skating (right arrow).
View Figure 2
Figure 2: All bar values in this Figure 2 were shifted of + 0.5 mm (1/50th inch), otherwise zero values would have shown no bar. All LLD between zero and 3.2 mm (1/8") inclusively (i.e. here 3.7 mm with the shift, dotted line), were clinically considered as an absence of LLD sign. The abscissa indicates the number of follow-up days including the Pre visit (before UCR), and the ordinate indicates the LLD (maximum at 18.0 mm (0.7" ≃ 3/4") (a) Effect on LLD of a fall on the buttocks during a treadmill session; (b) Effect on LLD of a fall on the buttocks in the stairs. Two UCR were necessary (4 days interval) to reverse the 12.7 mm (1/2") LLD; (c) Effect on LLD of a hit on the hips during a hockey game; (d) Equal and constant small residual LLD of 3.2 mm (1/8") along the FU period, suggesting the presence of an anatomic LLD. Also of interest is the 12.7 mm (1/2") LLD caused by hitting a wall during physical education at school (left arrow), and falling on the buttocks while roller skating (right arrow).
View Figure 2
LLD was measured just before and one hour after the UCR. Typically, the LLD would disappear completely within one hour after the UCR, and the pelvis would return to level in standing position. This suggests that there is a quite rapid neuromuscular response following the craniocervical realignment procedure that translates into some disappearance of LLD. The following Figure 3 illustrates the loss of 19.1 mm (3/4") of FLLD measured just before and one hour after the UCR.
 Figure 3: Illustration of a 19.1 mm (3/4") LLD complete disappearance, measured just before and one hour after the UCR.
View Figure 3
Figure 3: Illustration of a 19.1 mm (3/4") LLD complete disappearance, measured just before and one hour after the UCR.
View Figure 3
The results herein presented suggest that an UCM may lead to some neuromuscular imbalance that manifests as FLLD. LLD is associated with pelvic tilt, either cause or effect, which may result in compensatory lateral curve of the spine [8]. Yet there is evidence that even a small amount of pelvic tilt can result in changes of a true structural scoliosis if the tilt has been present for a long time, especially if present during the adolescence growth spurt [6,7,20].
The combination of an initial stage in which a small curve develops due to a small defect in the neuromuscular control system or paravertebral muscles [25-30], pelvic tilt/rotation, compensatory functional spinal deviations [7], aggravating biomechanical factors, asymmetrical bone growth of the vertebrae [28] and wedging [31], and further spinal degenerative changes [9] might explain the cascade of events responsible for the initiation, development and progression of idiopathic scoliosis.
This article suggests that an UCM may result into neuromuscular FLLD, it however does not demonstrate the mechanism by which the neuromuscular function can be affected, possibly involving the central nervous system. Although the neuromuscular contribution has not been proven (by electromyography for instance), and that this work is not a randomized double blinded study, the authors opine however that, in the light of the results herein presented, there is some level of evidence-based medicine supporting that UCM may somehow be involved in FLLD among pediatric scoliotic patients, and that UCR can help to reduce this FLLD. Therefore, this article could be seen as a precursor systematic investigation of 40 consecutive scoliotic patients, presenting novel scientific data, concepts and hypothesis, and that opens the door for further research.
Although all patients were scoliotic, the consideration of Cobb angles in regards with LLD and UCR, and consequent longitudinal full spine radiology and quantification, was beyond the scope of this article that focuses on the association between LLD and UCM.
The scoliotic children of the cohort presented with concomitant functional leg length discrepancy and upper cervical misalignment. The discrepancy resulting from compensatory neuromuscular imbalance caused by the craniocervical junction misalignment can be reversed by means of a realignment. The leg length discrepancy herein observed is measured in an unloaded horizontal position. It is likely that by forcing the feet to be even on the ground in a vertical gravitational position, these neuromuscular imbalance forces would not disappear but rather translate into other pelvic and spinal compensatory deviations that could possibly contribute, if not be causative, to the initiation of scoliosis and its development.
We would like to thank Dr. DH Eidelman and Dr. JP Farmer from the McGill University Faculty of Medicine for their kind support.
There are no conflicts of interest.
All the authors equally contributed to this study.
This research was not supported by any funding source.