Introduction: Globally, musculoskeletal disorders (MSDs) combined account for more than a fifth of the total years lived with disability. This condition affects workers alone and people across the life-course in all regions of the world. Despite this long-standing awareness, MSDs continue to be the main reason associated with people with a work-related illness. The aim of this study is to explore the prevalence of work-related musculoskeletal disorders among workers in sugar factories in Jinja-Uganda.
Methodology: This study implored a cross-sectional study design among the sugar factory workers considering their baseline data. A structured, standardized questionnaire Nordic Musculoskeletal Disorders Questionnaire (NMQ) was used to capture the data. A sample size of 402 was divided equally among two sugar factories, A and B. Ethical approvals were sought from the relevant bodies before conducting the study.
Results: The quantitative data were analyzed using IBM SPSS Version 26, a descriptive statistic such as mean, standard deviation, percentages, and frequencies was conducted. A higher prevalence of 77.1% was reported among Factory A and 28.4% in Factory B in 12 months. The respondents were the lower back region, 63.7%, and the upper back region, 46.3%, was the most affected body region. An independent t-test showed statistical differences between the following variables in both factories; age (p = 0.000), BMI (p = 0.000), duration of work in the field per day (p = 0.033), systolic (p = 0.000), and diastolic rate (p = 0.000).
Conclusion: This study revealed a very high prevalence among the sugar factory workers due to high ergonomic risk exposure during respondents' work activities. Due to the recorded high prevalence, an ergonomic intervention among the workers to enhance their wellness by addressing SDGs goal number 3 was recommended. This will reduces the socioeconomic burden of work-related absenteeism and ultimately increases the productivity among the sugar factory workers.
Prevalence, Work-related musculoskeletal disorders, Sugar factory, Workers
One of the highest global leading causes of years lived with disability are musculoskeletal disorders (MSDs) [1]. It is also a complex and multifactorial phenomenon that includes psychological, biological, psychological, and social factors and represents a significant burden for the individual and society. Globally, all MSDs combined account for more than a fifth of the total years lived with disability [1]. This condition of musculoskeletal disorders affects not only workers but people across the lifecourse in all regions of the world. Musculoskeletal disorders conditions based on the reports from the WHO was known as one of the leading causes of disabilities in four out of the six World Health Organization countries/regions in 2017, it was ranked second in the East Mediterranean Region and third in the African Region) [2]. There is an association between the prevalence of musculoskeletal disorders, which increases with the age of an individual; younger people are also affected, often during their peak income-earning years [2].
The largest leading producer of sugarcane worldwide is Brazil, followed by India, China, Thailand, Pakistan, and Mexico [3]. The sugar cane factory is one of the most important agricultural sectors in Uganda and worldwide, which directly contributes to creating employment, income, and social developments in the rural areas of the country. Both skilled with a certain level of education and unskilled workers with low or no formal education from rural areas are engaged in this sector. Most sugar factories have poor occupational health and safety measures; there are sometimes inadequate policies and infrastructure to meet the health hazards. Hence, the workers are exposed to workplace accidents, repetitive strain injury (RSI), and musculoskeletal disorders (MSDs) in the neck, upper back, lower back, and arms due to continuous movements [4]. The sugar factory is one of the fastest-growing agro-allied/agro-processed agricultural products in Uganda and East Africa. Non-availability of information on MSDs may deprive policy makers on accurate estimation that will assist in making well-informed decisions related to resource allocations and subsequent management of those with MSDs. It is also incumbent on the sugar factory to reduce the cost of treating MSDs among workers, which might have been because of the work exposure. This shows a considerable gap in knowledge that the health of workers in the agriculture sector, mainly subsistence, is the dominant economic activity, representing 72 percent of Uganda's workforce. Sixty-seven (67%) percent female (rural women), and 65 percent males. The sector also accounts for 52 percent of the country's total exports [5].
In Uganda, studies on MSDs have been conducted among schoolchildren by Mwaka, et al. [6], and Healthcare workers by Abdulmujeeb [7], but an extensive review of the literature did not reveal any studies on the prevalence and risk of MSDs among farmers most especially on the sugar factories workers in the country. Sugar factory workers need to perform detailed tasks that consistently require them to assume prolonged and static working postures, perform fine muscular work in unnatural postures, and use high-frequency vibration tools, which have been reported to result in the development of MSDs [8]. The majority of available sparse literature on MSDs in African countries was not focused on Agricultural settings, especially sugar factories. Therefore, it is on this adding to existing knowledge that this paper aimed to explore the prevalence of work-related musculoskeletal disorders among sugar factory workers.
This study was a multiple cross-sectional study to capture baseline data from the two sugar factories. A cross-sectional survey was used to study a phenomenon at a given time or to gather data from multiple groups at the same time [9]. This study design was selected as it has been used in previous studies on musculoskeletal disorders (MSDs) among dentists, steelworkers, nurses, and office workers [10].
The study was conducted in Jinja and Buikwe, municipal Uganda; Jinja municipal comprised of Agro-allied industries where most of the sugar factories are located. The study was in two different factories located in Jinja, Uganda.
Since the target population in the sugar factory, all the workers in all units were considered. The sample size determinations have the following assumptions in calculating the minimum sample size for the two study sites. The two sugar factories comprise approximately 10,000 workers. The sample was calculated using the formula by Schulz and Grimes [11].
The formula above clearly shows the minimum number of subject cases required to identify a true relative risk or an experimental event rate with the power and two-sided type I error probability α (alpha). 5% is mostly the usual choice for α. Typical values for the power (The probability of detecting a real effect of a sample) are 80%, 85%, and 90%, respectively.
β = 1 - power,
nc is the sample size corrected for continuity,
m is the number of control subjects per experimental subject,
p0 is the chances (Probability) of the event in controls occurring,
p1 is the chances (Probability) of the event in an experimental subject will occur,
Zpi is designated as the normal standard deviation for the probability p [12].
By inserting in the formula n = 366
Having 10% of no response as an assumption, the final sample was 366 + 36.6 = 402
This sample size was then divided equally for the two companies;
Factory A (n = 201), Factory B (n = 201).
Workers in all the units were randomly selected, and based on their willingness to join the baseline survey, only a total of 201 were included in the study based on the calculated sample size for each factories.
Inclusive criteria
To participate in this study, the following criteria was set:
1. The participant with symptoms of MSD in the last three weeks
2. Age 18 and above
3. The participant with more than six months of working experience.
4. Participants who are willing to join the study
Exclusive criteria
The exclusion criteria for participants in this study were if they did not meet all the above inclusion criteria.
1. The participant with an accident on any of this MSD region within the past 12 months
2. The participant with limb surgery within the past 12 months
3. Females participant who is pregnant
4. Participants who are critically ill and those with comorbid diseases such as TB
This study adopted Nordic Musculoskeletal Questionnaire (NMQ) because it is suitable for its applicability in workplaces and a large number of workers because it is very quick and cheap [13]. This Nordic Musculoskeletal Questionnaire (NMQ) includes the nine anatomical body areas: the neck, the shoulders, the back, the elbows, the wrist/hands, the thighs, the knees, and the ankles. The most useful measuring instrument that is always used to evaluate work-related musculoskeletal disorders among workers of different sectors worldwide is the Nordic Musculoskeletal Questionnaire (NMQ). The NMQ has several advantages over other measuring instruments. Some of them are standardized questions, worldwide recognition, and its free. It also provides a basis for self-evaluation among workers and even fast in quick identification of primary symptoms of Musculoskeletal disorders among workers [14].
The study toots was tested for realiability and a reliability of 0.70 or higher was considered acceptable for this study. The NMQ has been translated into various languages and tested for its validity and reliability (Wang, et al. 2017). The Validity index of 0.903 and 0.98 was ascertained, which is greater than the Standard Value of 0.7, indicating that the items were extremely relevant and therefore considered acceptable for this study.
Data analyses were done using IBM statistical packages for social science (SPSS) version 26 [15]. The prevalence of MSDs for each anatomical region was calculated during the last 12 months for the baseline data.
This study was conducted according to the research guidelines of the authors' institutions MKU/ERC/1644, accordance with the Declaration of Helsinki and approved by the ethical review board in Uganda CIUREC/0234.
The following guideline in accordance with the Declaration of Helsinki was used to address the ethical issues in the field during the research.
i. The purpose of the study was explained to participants using an information sheet.
ii. The participants were assured of strict confidentiality of any information they provided.
iii. Each participant was required to fill out an informed, written consent letter.
iv. Anonymity was assured to the participant using codes for identification instead of their names.
Table 1 below shows the demographic information of Factory A and B respondents involved in the baseline survey respectively, where it can be observed that two-thirds of Factory A respondents were between the ages of 20-29 while the majority of the respondents from Factory B were between the age of 30-39. Similarly, 8 out of every 10 respondents in both factories were found out to be male, and where relatively half of both factories were married in both groups. Regarding the highest level of education, the majority of the 201 respondents 94/201 (46.8%) and 83/201 (41.3%), respectively had certificates/diplomas. The mean BMI of both respondents was 22.97 and 24.52; both groups of respondents displayed an average of 122/131 systolic blood pressure and 77/81 diastolic blood pressures approximately. More than one-third of the respondents involved in both groups were fieldworkers, and relatively half of them (101/201 (50.2%) and 84/201 (41.8%) majority of the worker in both factories were from the manufacturing department 101/201 (50.2%). More than 70-85% of the respondents do not smoke simultaneously, more than three-quarters of both groups do not drink.
Table 1: Sociodemographic characteristics of the study participants. View Table 1
Regarding the work experience across the two groups, Factory A had more workers with less than 5 years of work experience. In contrast, Factory B had the majority of workers with working experience of 10 years. Regarding the working hours per week and per day, more than half of the respondents in both Factories worked for 40-60 hours per week, for 5 and more hours per day respectively among the respondents (see Table 1).
Table 2 below shows the characteristics of the musculoskeletal disorders by body parts among the respondents at the baseline. It shows the body regional MSDs prevalence based on 12 months, prevalence based on 7 days, and how workers are prevented from doing normal activities (at work, home or Leisure) because of the trouble as a result of MSDs. The following prevalence was recorded from baseline data of the respondent (n = 201) at 12 months and 7-days for Factory A and Factory B with lower back pain having the highest prevalence (A = 63.7% & B = 40.8%), and (A = 62.2% & B = 39.8%), upper back pain (A = 46.3% & 26.4%) and (A = 44.3% & B = 25.9%), wrist/hands (A = 24.3% & B = 13.9%), and (A = 23.4% & B = 13.9%), shoulder (A = 17.9% & B = 16.4%) and (A = 17.9% & 17.4%), elbow (A = 16.4% & 10.0% and (A = 14.4% & B = 9.5%), Neck (A = 14.9% & B = 10.4%) and (A = 11.9% & B = 10.9%), hips/thigh (A = 14.4% & B = 16.9%) and (A = 11.9% & B = 14.4%), Knee (A = 12.9% & B = 20.4%) and (A = 10.9% & B = 21.9%), with the ankle/Feet with the lowest prevalence at (A = 8.0% & 13.9%) and (A = 6.0% & 14.4%). During the last 12 months respondent were prevented or hindered from doing their normal activities (at work, home or Leisure) because of the trouble in the respective anatomical regions, this was also represented in the Figure 1, Figure 2 and Figure 3. The highest prevalence of such hindrance was on lower back pain having prevalence of (A = 34.8% & B = 38.8%), upper back pain (A = 22.4% & B = 27.9%), wrist/hands (A = 10.9% & B = 14.9), shoulder (A = 10.0% & B = 14.9%), elbow (A = 9.0% & B = 10.9%), Neck (A = 7.5% & B = 13.4%), hips/thigh (A = 7.5% & B = 14.4%), Knee (A = 6.5% & B = 23.9%), with the ankle/feet with the lowest prevalence (A = 5.0% & B = 13.9%).
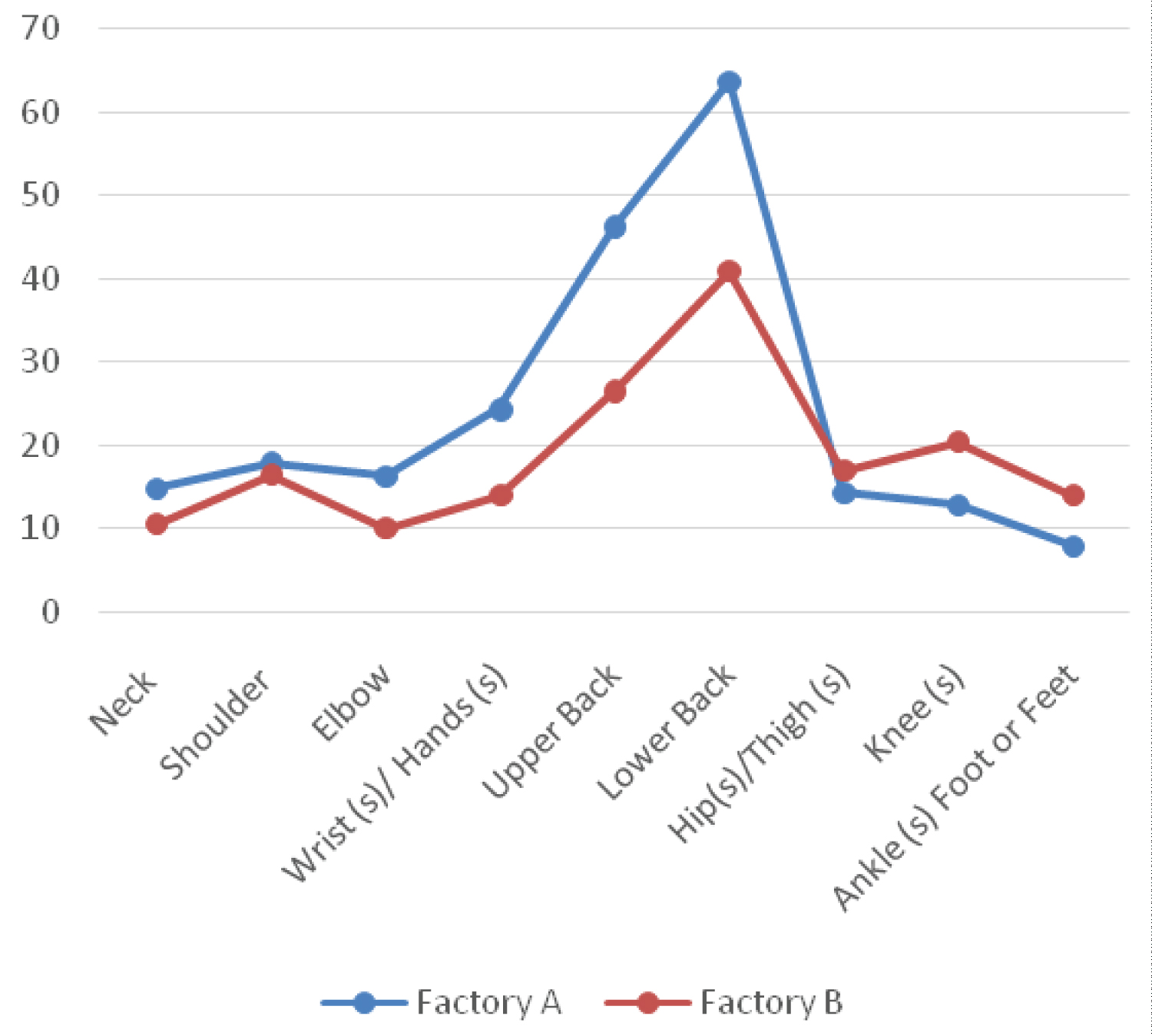 Figure 1: Showing prevalence for last 12 months of MSDs.
View Figure 1
Figure 1: Showing prevalence for last 12 months of MSDs.
View Figure 1
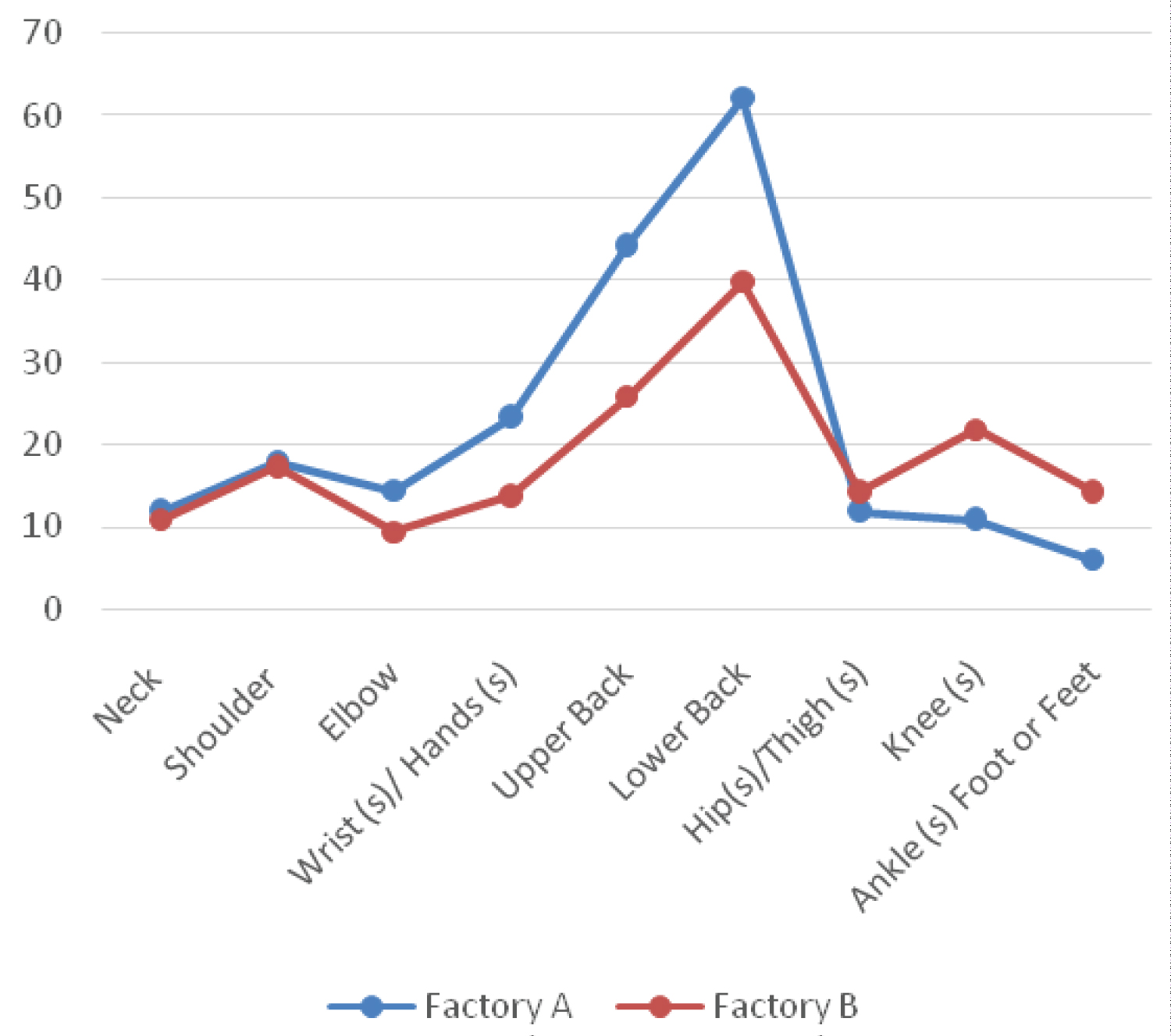 Figure 2: Showing prevalence for last 7 days MSDs.
View Figure 2
Figure 2: Showing prevalence for last 7 days MSDs.
View Figure 2
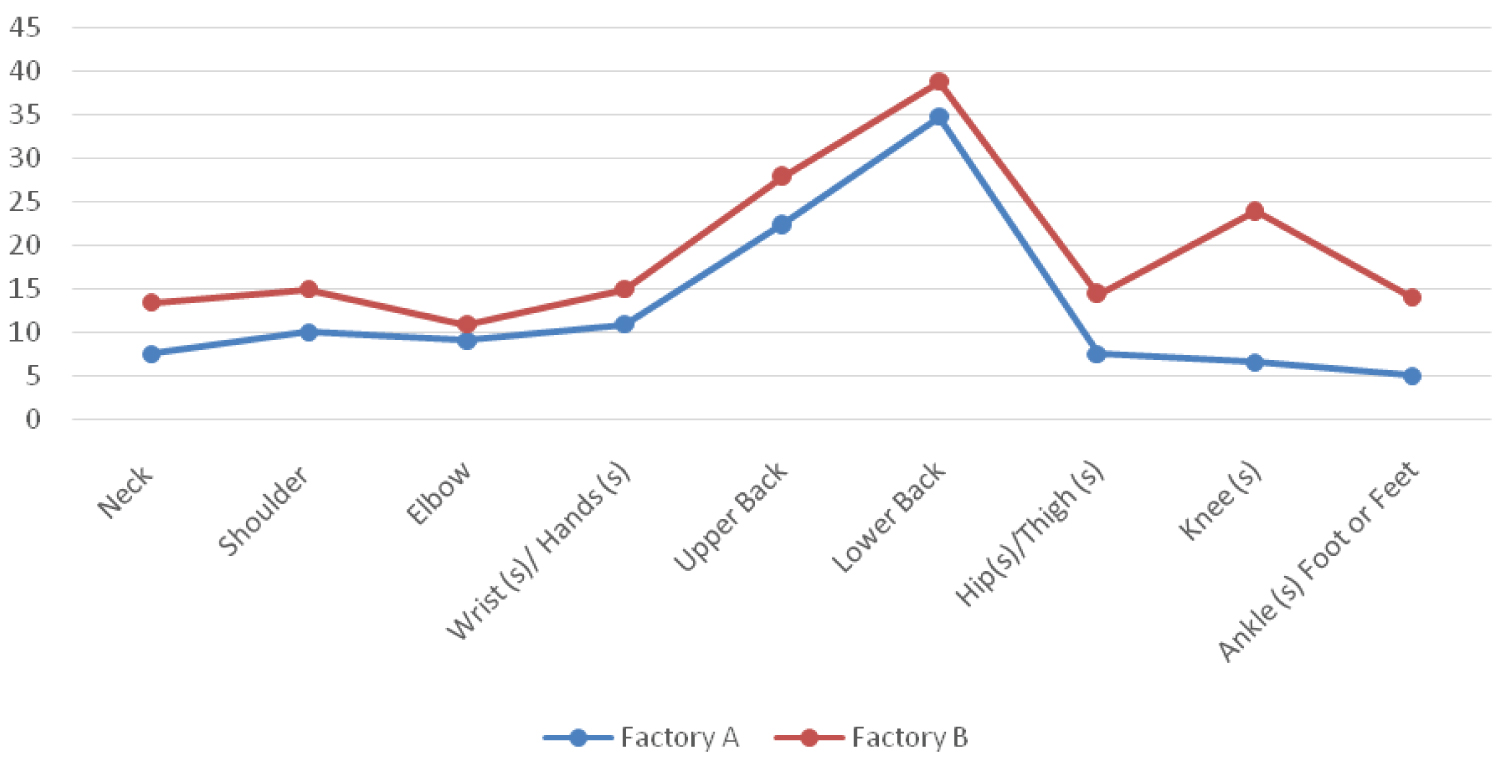 Figure 3: Showing prevalence of last 12 month prevented from doing normal activities.
View Figure 3
Figure 3: Showing prevalence of last 12 month prevented from doing normal activities.
View Figure 3
Table 2: Characteristics of WRMSDs of the study participants (n = 402). View Table 2
An independent t-test was run to see statistical differences between variables at baseline for the two factories, as shown in Table 3 above. Variables such as; Age of the respondent (P = 0.000), BMI (P = 0.000), Duration of work in the field per day (P = 0.033), systolic (P = 0.000), and Diastolic (P = 0.000) were all significantly different between the two factories.
Table 3: Independent t-test for baseline characteristics of the study participants. View Table 3
This study aimed at exploring the prevalence of work-related musculoskeletal disorders among sugar factory workers in Uganda. This study reported the prevalence of WRMSDs during the last 12 months in both factories as 77.1% and 28.4% for Factory A and Factory B. The high prevalence in Factory A resulted from manual work activities, which are less mechanized than the control group, the manual work predisposed workers to musculoskeletal disorders. Workers are constantly exposed to occupational hazards during their occupational activities, which predisposes them to have difficulties in carrying out their duty which translates into musculoskeletal disorder among the workers. This pain has remained one of the most common signs, and symptoms of work-related musculoskeletal disorders is excruciating pain among the workers affected by the WRMSDs regions during their working time [16]. Several studies conducted in various occupational settings with similar work situations were explored to discuss this study. The extremely high prevalence recorded in this study was comparable to multiple studies conducted by Phajan, et al. [17], who reported a very high prevalence of 82.96% and 88.70 for 12-months and 7-days among sugarcane farmers on work-related musculoskeletal disorders in North-eastern Thailand. In their study lower back region had the highest prevalence of 58.7% t region on the anatomical region among the respondents which was similar to findings from this study. A very high WRMSD prevalence of 96.6% during the last 12 months was also reported by Mousavibaghi, et al., among Technicians of Surgery who reported pain and discomfort in at least one of the anatomical regions. They also reported lower back region having a prevalence of 71.5%, and the least on the anatomical region was ankles with 16.2%, similar to findings from this study [18]. A similar study by Udom, et al., in a rubber plantation in Pakistan, also revealed that the prevalence of WRMSDs in the last year was 87.7% and the last week to the study was 65.11% [19]. A Nigeria study by Okeuze O, et al., on work-related musculoskeletal disorders among office workers in Higher Education institutions also reported a very similar prevalence to this current study of 71.9% [20]. In their research, considering different anatomical regions, the study showed a higher WRMSD prevalence on the lower back region of 58.1% and the lowest to be 20.7% ankle/feet, similar to the same result from this current study among factories workers. Another comparable prevalence rate from two studies among Turkish office workers by Celik, et al., and Ardham H, reported a similar prevalence of 68.1% and 69.7%, with both studies showing severe WRMSDs symptoms, which triggers difficulties among workers during their work schedule and physical discomfort [21,22]. Lagerstrom, et al., conducted an interventional study on professional loggers on Active surveillance on WRMSDs symptoms in the development of safety intervention reported a year prevalence of 60% among the conventional harvester and 50% among mechanized harvesters [23]. They further attribute this varying in prevalence between the two factories due to the machine used among mechanized harvesters, which reduces their chance of being exposed to ergonomic hazards as compared to the conventional harvester. Also, the one-year prevalence of lower back was 24.8% in conventional and 22.7% in mechanized harvesters.
The Factory B of this current study also revealed a very similar prevalence (of (40.8% & 46.3%)) for the lower back region, upper back region (21.7% & 26%), and elbow having the lowest prevalence of (10.4% & 21.1%). The increase in the prevalence rates accounts that workers are continuously being exposed to ergonomic hazards that predisposed the respondents to develop WRMSDs among the workers. Despite the mechanized organization of Factory B, workers are still prone to the development of WRMSDs since ergonomic hazards control are not adequately in place as recommended. Gourab, et al., conducted similar work on work-related musculoskeletal disorders among male sugar factory workers who deal mainly with molasses in Nadia district of West Bengal, India, with an extreme prevalence of 76% for the lower back region. They also reported Ankle/feet 3.5%, which was precisely similar to the report of this current study in Uganda [24]. Different studies conducted in different occupational regions supported this very high prevalence. A similar cross-sectional survey conducted by Smita, YV & Deepak (2016) also revealed a very high prevalence of WMSD's among sugarcane workers [25,26]. From their results, they reported that prevalence was more in the lower back (50%), knee (29%), neck (19%), hip (13%), ankle (10%), upper back (13%), shoulders (13%), elbows (10%) and wrists (14%). A Malaysian study on establishing a relationship between work-related musculoskeletal disorders and certain risk factors like psychosocial factors was conducted in research conducted among healthcare workers in a public hospital in Malaysia. They reported prevalence rate for different body parts was the upper lumbar (back) (40.69%) with a slightly higher prevalence as compared to the lower back region, with lower prevalence having the prevalent to be (35.28%) though slightly different from the prevalence reported in this current study [27]. Similarly, Arsalani, et al. [28], in their research conducted among nursing staff personnel in Tehran, Iran. They reported that 88.0% of the nursing staff have complained and experienced musculoskeletal disorders in one of the anatomical regions for Musculoskeletal disorders in the last year, with the lower back having the highest prevalence rate at (65.3%) similar to findings from the experimental group prevalence at baseline.
Findings from this study reveal the magnitude of MSDs among the sugar factory workers, which has been one of the neglected areas of research in Agricultural industries. Work-related musculoskeletal disorders are relatively common among sugar factory workers in Uganda, although the etiology of WRMSDs among the sugar factory workers was multifactorial. This current study revealed a comparative prevalence between two sugar factories. The prevalence of MSDs was so alarming and high among the factory workers, which predisposes the workers to the prognosis of MSDs in both factories. Lower back pain was the most reported anatomical region for MSDs among the workers in almost all the units of the sugar factories. Although the reason for this high prevalence was due to Factory A working condition was not as mechanized as in Factory B. Majority of the workers in Factory A cane yards unit always offload the sugar cane manually from the truck, this exposes the workers to a lot of occupational hazards such as award bending, prolong twisting and repetitive movements. Factory B uses more of an engineering control hierarchy, so most of the work in the factory was done by the machine, including offloading sugar cane from the truck and loading sugar into the truck, so workers face few hazards compared to Factory A. It is evident from the study findings that workers in mechanized factory were also prone to the development of MSDs but to a lesser extent than workers in non-mechanized factory. Therefore, incorporating ergonomic-based intervention on-the-job training initiatives for old and new workers and with continuous improvement in workplace conditions may reduce workplace accidents or injuries and work absenteeism among workers and overall increase work productivity.
To achieve goal 3 by 2030: Ensuring healthy lives and promoting well-being for all ages, findings from this baseline data will be used to formulate ergonomic-based intervention among the various factory workers.
1. In addition to routine occupational health and safety training to employees as speculated and required by the Uganda Health and safety Act 2005 legislation, it is also recommended that factories should be focused more on educational and promotional activities aimed at improving occupational and safety awareness and to also create a safety culture within the Factory. The outcomes of this occupational training should be documented, monitored, and reported by regular inspections to the top management.
2. A low-cost solution is recommended for them to alleviate the risk and burden of WRMSDs; this should include a work-rest cycle and sitting chair with backrest and hand rest or position during work.
3. The Labor Union in Uganda should ensure workers in this occupational setting work within the confines of the country's occupational health and safety guidelines to reduce the prevalence of MSDs among workers.
1. The physical symptoms of musculoskeletal disorders and the pain mechanism were not being investigated.
2. This study relied on self-reported data; the respondents might not have reported all incidences of musculoskeletal disorders, or some level of bias might have set in during the filling of the questionnaire.
1. The economic burden of musculoskeletal disorders should be thoroughly explored because, so far, in African settings no documented evidence on the Regional burden of WRMSDs.
2. Epidemiological surveillance systems should be further studied to ease the proper diagnosis of WRMSDs among the workers.
3. Linking the disease's co-morbidity to the prognosis of WRMSDs should also be explored.
The study was conducted in accordance with the Declaration of Helsinki, according to the research guidelines of the authors' institutions MKU/ERC/1644 and approved by the ethical review board in Uganda CIUREC/0234. All the subjects were consented to through the informed consent letter before the research was conducted and all ethical principles were applied during and after data collection.
Not applicable.
Some or all data, or codes that support the findings of this study are available from the corresponding author upon reasonable request.
The authors declare no conflict of interest.
No grant was obtained for this research.
AAB: Generated the concept of this research paper, wrote up of the research proposal, analyzed the data, involved in presentation and interpretation process of results and discussion, reviewed and finalized the manuscript document, and corresponding author. AOO: Generated the concept of this research paper, wrote up of the research proposal, analyzed the data, involved in presentation and interpretation process of results and discussions and draft the manuscript. JJ: Involved in wrote up of the research proposal, analyzed the data, involved in presentation and interpretation process of results and discussions, and reviewed the draft manuscript document. MAS: Involved in wrote up of the research proposal, involved in presentation and interpretation process of results and discussions, and reviewed the draft manuscript document. All the authors read and approved the final manuscript.
The authors would like to thank the management and workers of the two factories, Uganda farmer's crops limited and Sugar Corporation of Uganda Limited for their cooperation through the data collection process.