Background: Neglected radiocarpal dislocations are rare and may have functional repercussions on the injured limb.
Objective: The aim of this study was to evaluate the functional results of our management of neglected radiocarpal dislocation.
Patient and method: This was a retrospective and descriptive study of five cases of neglected radiocarpal dislocation between January 2011 and December 2020. Patients were collected from various hospitals in Abidjan, Ivory Coast (some private centers and the orthopaedic surgery and trauma department of Cocody University Hospital). The minimum consultation time was 11 weeks. The initial treatment was traditional in 3 cases and failure of hospital treatment in 2 cases. Lesions were classified according to the Dumontier classification. Treatment was surgical in all cases. Functional results were assessed using the Quick DASH score and the modified Green and O'Brien score.
Results: Patients were assessed for function at a minimum follow-up of 24 months. The total Quick DASH score was obtained using the formula: [(Sum) × 1.1] × 5/2. The mean Quick DASH score was 88.55 (extremes: 74.25 and 99). The mean modified Green and O'brien score was 96 (extremes: 80 and 100).
Conclusion: Our functional results were satisfactory overall, as demonstrated by assessments using recognised and reliable tools. Further studies with a larger sample size are needed to confirm the conclusions of our study.
Africa, Functional results, Neglected dislocation, Radiocarpal, Treatment
Radiocarpal dislocation (RCD) is a complete loss of contact between the articular surfaces of the carpus and the articular surfaces of the radius [1]. They occur following high-velocity trauma [1,2]. They can have functional repercussions on the injured limb. Where they exist, associated lesions influence the choice of treatment and the functional prognosis of the wrist.
RCD is said to be neglected or chronic when, whether it is reducible, it remains untreated for up to 6 weeks from the date of the trauma [3,4]. It should be distinguished from irreducible RCD. Neglected RCDs are rare, accounting for 0.2% of all dislocations [5]. There is no consensus on the treatment method for neglected RCDs [6]. In general, treatment consists of precise surgical reduction, possible ligament reconstruction and stable fixation until complete healing [4]. The indications for treatment depend on the type of injury, the patient's professional situation and the surgeon's experience. Alternative techniques such as proximal carpectomy, lunate excision and wrist arthrodesis have been described [7,8].
The aim of this retrospective descriptive study was to evaluate the functional results of surgical reduction of neglected RCDs in black African patients, using recognised and reliable tools.
Between January 2011 and December 2020, five cases of neglected CRL were managed in different hospitals in Abidjan, Ivory Coast (some private centers and the orthopaedic surgery and traumatology department of the Cocody University Hospital). The minimum consultation period was 11 weeks. The patients were all male, manual workers and right-handed. The average age of the patients was 34 years (extremes: 29 and 56). The initial treatment was conventional in 3 cases and failed in-patient treatment in 2 cases. The lesions were all classified as Type 2 in Dumontier's classification [9]. The initial dislocation was anterior with an anterior marginal fracture of the radius in 3 cases. It was posterior with a posterior marginal fracture of the radius (n = 1), and posterior with a fracture of the radial styloid (n = 1) (Figure 1, Figure 2 and Figure 3). Associated injuries were tendon transection (n = 2), scapholunate dislocation (n = 1) and ulnar styloid fracture (n = 3).
 Figure 1: (a and b) Dislocation with fracture of anterior margin.
View Figure 1
Figure 1: (a and b) Dislocation with fracture of anterior margin.
View Figure 1
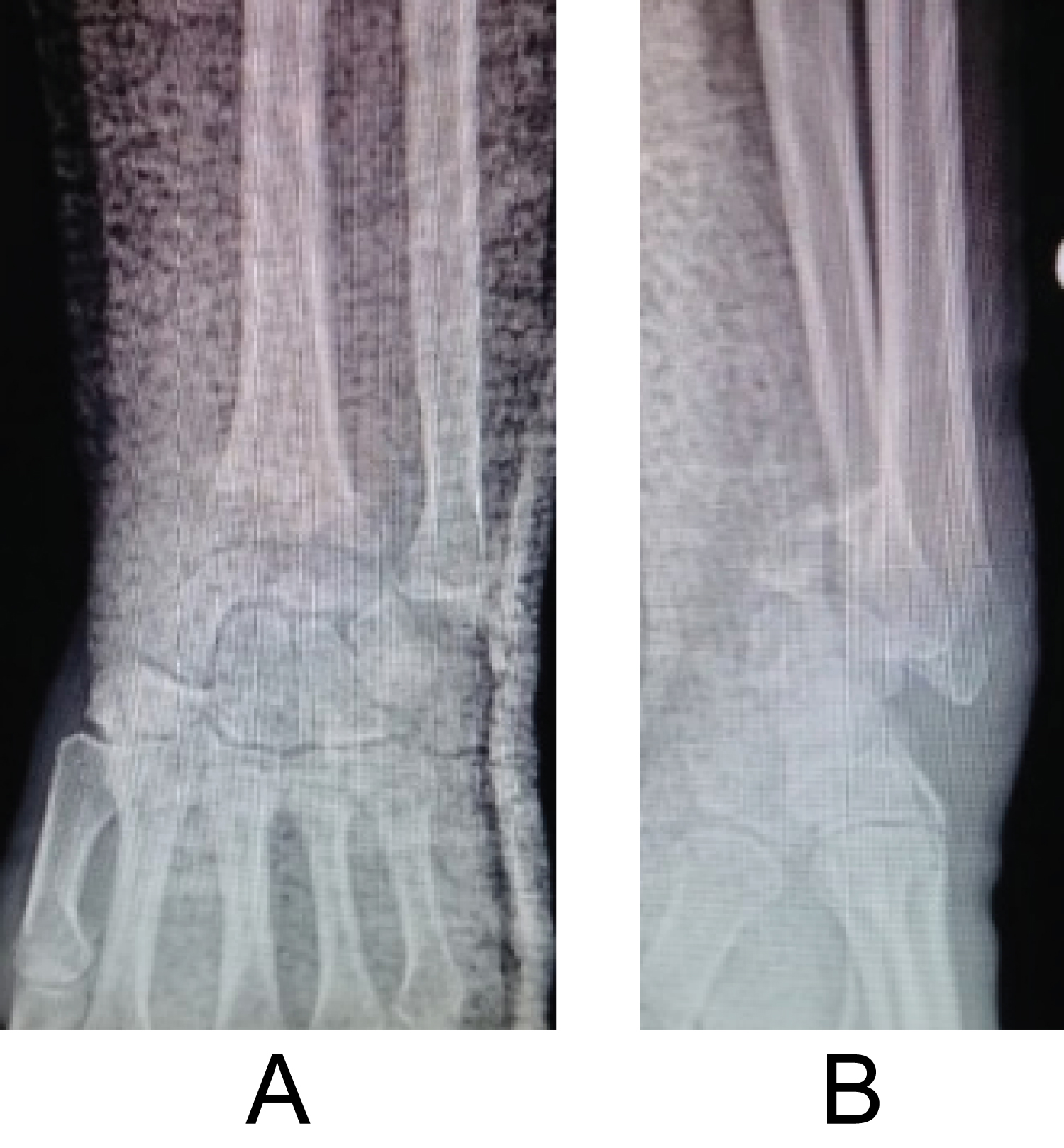 Figure 2: (a and b) Radiograph of an anterior dislocation with fracture of the anterior margin.
View Figure 2
Figure 2: (a and b) Radiograph of an anterior dislocation with fracture of the anterior margin.
View Figure 2
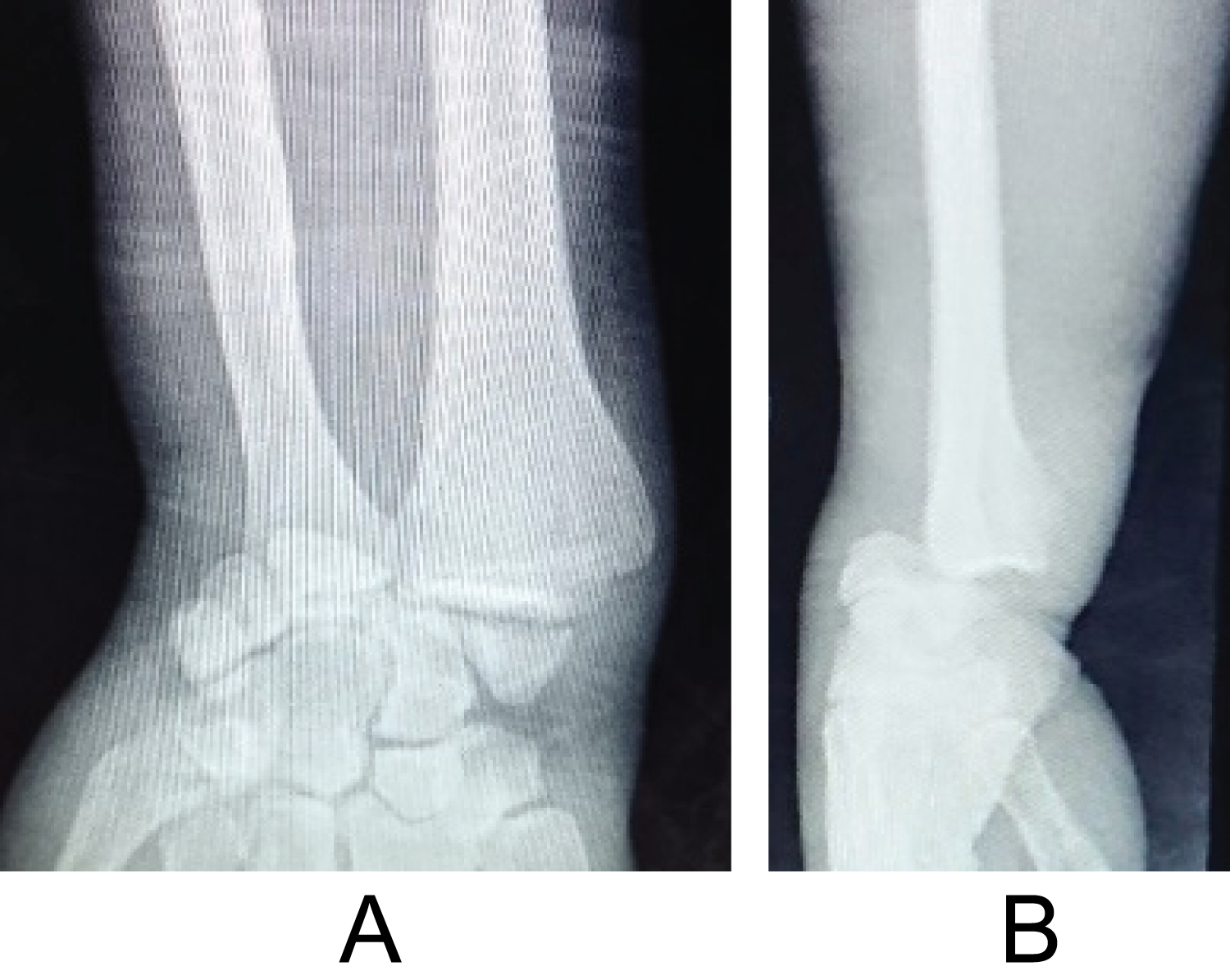 Figure 3: (a and b) Radiograph of posterior dislocation with radial styloid fracture.
View Figure 3
Figure 3: (a and b) Radiograph of posterior dislocation with radial styloid fracture.
View Figure 3
All our patients underwent a minimum of 12 rehabilitation sessions before undergoing surgery. Treatment was surgical in all cases, without ligament suture. The indication for surgery was essentially based on the injury profile. The approach was dorsal in all cases. Two neglected RCDs were surgically reduced and immobilised with an external fixator (Figure 4). The other 3 were also surgically reduced but fixed by screw and K-wire (n = 1), screw plate (n = 1) and simple K-wire (n = 1). In the latter 3 cases, the wrist was immobilised in an anterior plaster cast. The severed extensor tendons were repaired in accordance with standard techniques. The criteria for successful surgical intervention were checked by fluoroscopy: Reconstitution of the bistyloid line and radioulnar index, and absence of distal radioulnar translation.
 Figure 4: (a and b) Control radiograph of reduction osteosynthesis with external fixation.
View Figure 4
Figure 4: (a and b) Control radiograph of reduction osteosynthesis with external fixation.
View Figure 4
Apart from reduced RCDs synthesised with an external fixator, the duration of post-operative immobilisation with an anterior plaster cast varied from 4 to 8 weeks. The external fixator was kept in place for 8 to 12 weeks. Fracture stabilisation and consolidation was achieved after an average of 10 weeks.
After removal of the plaster cast or external fixator, patients were referred to a physiotherapist specialising in upper limb surgery to begin rehabilitation. The rehabilitation sessions were designed to correct residual stiffness, prevent algodystrophy, eliminate pain and restore anatomical wrist joint amplitudes. All patients underwent an average of 30 rehabilitation sessions.
Two patients required repeat surgery. The first was for a recurrence of the dislocation 3 weeks after the first reduction-osteosynthesis using an external fixator (Figure 5). The second was for delayed consolidation with sepsis of a dislocation-fracture four months after the first surgery.
 Figure 5: (a and b) Follow-up radiograph of a reduction-osteosynthesis using an external fixator-whose surgery was repeated with osteosynthesis using a screw plate.
View Figure 5
Figure 5: (a and b) Follow-up radiograph of a reduction-osteosynthesis using an external fixator-whose surgery was repeated with osteosynthesis using a screw plate.
View Figure 5
In the postoperative time, patients were reviewed and re-examined in consultation at 4 weeks, 8 weeks, and 12 weeks and then once a year.
The clinical examination during follow-up consisted of measuring wrist joint amplitude using a goniometer, and bilateral measurement of grip strength. These checks were carried out using passive movements by the examiner. The choice of passive gestures made it possible to obtain real results, as the patient's active gestures, limited by possible pain, can bias the results. Other aspects of the follow-up clinical examination were a review of the possibility of returning to work and patient satisfaction.
Functional assessment consisted of scoring according to the Quick DASH score [10] and the modified Green and O'Brien score [11]. The total Quick DASH score was obtained from the formula [(Sum) × 1.1] × 5/2 [10]. Prior to surgery, all patients had a mean Quick DASH score of 67.1 (extremes: 57.75 and 79.75), (Table 1). The modified Green and O'Brien score [12] was 65 (extremes: 60 and 80), (Figure 2).
Table 1: Quick DASH score assessment data before and after surgery. View Table 1
On initial clinical examination, mean angulation was flexion 41° (extremes: 35° and 45°), extension 35° (extremes: 20° and 45°), ulnar tilt 13° (extremes: 10° and 15°), radial tilt 13° (extremes: 10° and 15°), pronation 50° (extremes: 45° and 60°) and supination 56° (extremes: 45° and 60°).
Patients were assessed at a minimum follow-up of 24 months. Table 1 and Figure 6 show the mean Quick DASH score and the modified Green and O'Brien score, respectively, after surgery and at the follow-up clinical examination. The mean Quick DASH score was 88.55 (extremes: 74.25 and 99) and the mean Green and O'Brien score was 96 (extremes: 80 and 100).
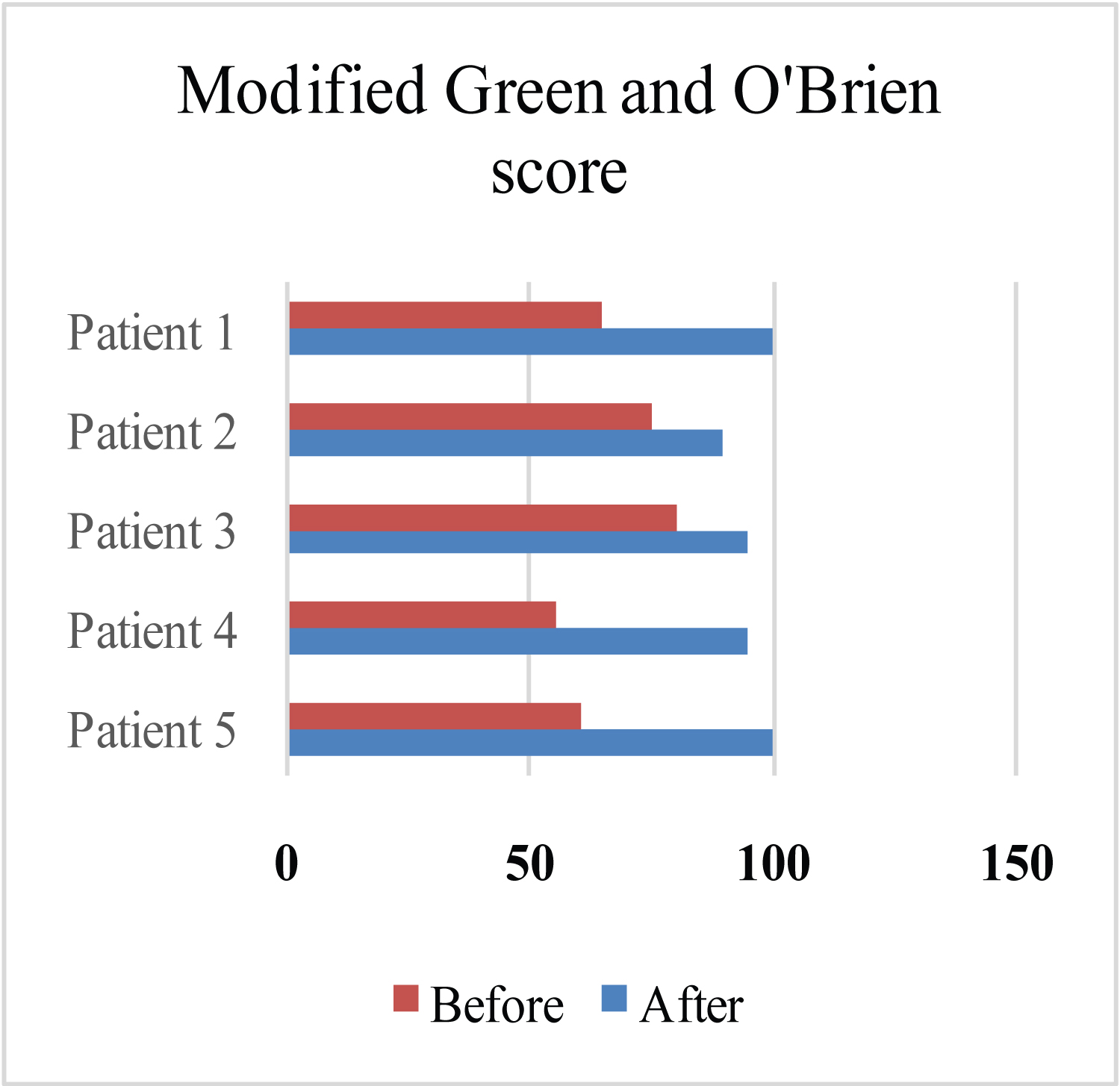 Figure 6: Modified green and O'Brien score evaluation data before and after surgery.
View Figure 6
Figure 6: Modified green and O'Brien score evaluation data before and after surgery.
View Figure 6
Mean flexion was 58° (extremes: 30 and 90), extension 34° (extremes: 20 and 50), ulnar tilt 15° (extremes: 10 and 20), radial tilt 10° (extremes: 5 and 15), pronation 58° (extremes: 20 and 90) and supination 42° (extremes: 20 and 60).
Four of the patients had returned to work, and we noted one occupational reclassification. All patients had resumed a leisure sporting activity after two years.
On clinical examination in hindsight, the mean angulation was palmar flexion 57° (extremes: 50° and 60°), dorsal flexion 52° (extremes: 40° and 60°), ulnar tilt 26° (extremes: 20° and 30°), radial tilt 17° (extremes: 10° and 20°), pronation 74° (extremes: 60° and 80°) and supination 71° (extremes: 65° and 80°). These results were better detailed by the group in Figure 7.
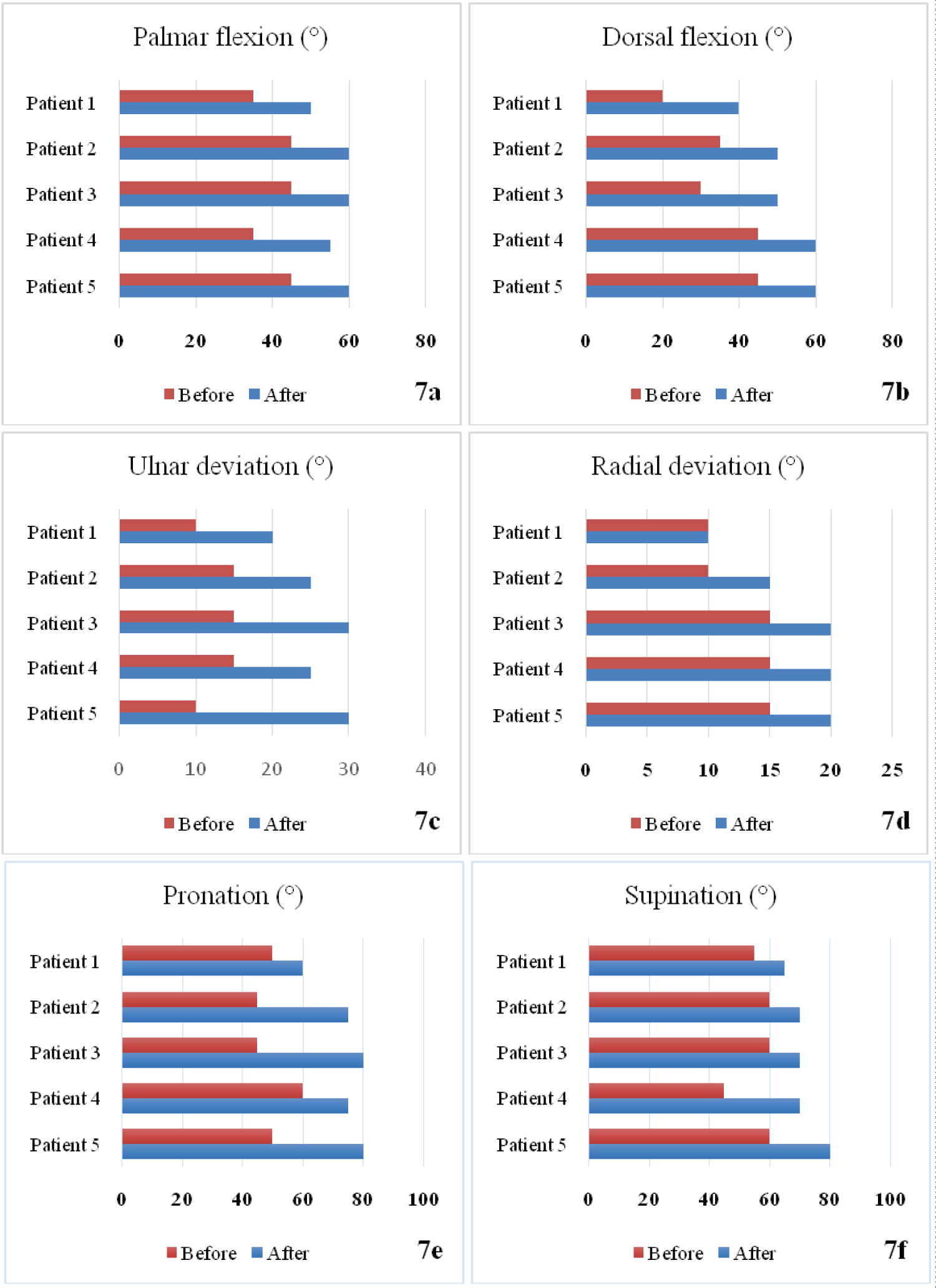 Figure 7: Detailed results of wrist amplitudes before and after surgery.
View Figure 7
Figure 7: Detailed results of wrist amplitudes before and after surgery.
View Figure 7
Post-operative complications included residual wrist stiffness in two patients. We also noted a loss of grip strength in one patient. Arthrosis developed in two cases, one radio-ulnocarpal and one scapholunate with ulnar translation. These osteoarthritic lesions were well tolerated.
Neglected RCD is rare [13]. Our study was relatively descriptive. No statistical analysis was necessary because of the small sample size. Neglected RCDs are exceptional because of the often-unbearable pain, which could lead the patient to consult a specialist. Moreover, in the black African context, trauma patients are used to being treated by bonesetters as a first-line treatment. This is not the case in developed countries. In this study, we treated three cases of RCD that had been neglected following traditional treatment. The problem of belief in traditional treatments and their resurgence remain a real problem for society, with considerable consequences for patients.
Dumontier established a classification of radiocarpal dislocations for therapeutic purposes, into Type 1 (dislocation with less than one third of the radial scaphoid surface torn off, requiring ligament suture) and Type 2 (dislocation with a synthesisable bone fragment) [9]. All our patients were Dumontier , et al. type 2 and had undergone osteosynthesis without ligament suture. The authors are not unanimous as to the methods of management of RCDs, but acknowledge the superiority of ligament suture, because of the great instability of these lesions [14,15].
The question of the need for ligament repair in the treatment of neglected RCD remains controversial [15]. Kailu, et al. believes that ligament repair is necessary to restore the anatomical relationship between the midcarpal bones and avoid late intercarpal instability [6]. Dhillon, et al. believes that it is not useful to repair retracted ligament ends in chronic RCD, due to the extent of fibrosis [4]. If possible, interosseous ligament repair is strongly recommended in neglected RCD [15]. However, ligament repair is almost impossible in most neglected RCDs and, in these cases; ligament reconstruction using tendon plasty is recommended.
Dumontier, et al. believe that failure to reinsert the ligament could lead to a complication such as ulnar translation with residual instability [9]. In all cases, the aim is to restore optimal anatomical congruence between the joint surfaces. The translation observed in our case was due to arthritic epiphyseal collapse rather than radiocarpal instability.
The functional results of our treatment were assessed at a minimum follow-up of 24 months. Two recognised and reliable tools were used for this assessment. The Quick Disabilities of the Arm, Shoulder, and Hand (DASH) score assesses the ability to perform everyday activities [16]. In our study, the mean Quick DASH score was 88.55 (extremes: 74.25 and 99). We observed an improvement in this score at the time of evaluation at follow-up, compared with the values observed before the surgical procedures [17].
The modified Green and O'Brien score assesses pain, mobility, functional status, and grip strength [12]. The results obtained using the modifiedGreen and O'Brien score were also satisfactory (Figure 6). These results corresponded to those found by other authors in the literature [2,18]. These satisfactory results can be explained by the austerity with which our patients were managed, including rehabilitation, which was carried out exclusively by a physiotherapist specialising in upper limb surgery.
The success of our results was because our patients had benefited from a minimum of 12 rehabilitation sessions prior to surgery. This helped to relax the tendinous and ligamentous structures of the wrist to facilitate reduction during surgery. Although this is a very advantageous technique, it has been overlooked by several authors in the literature.
Between 6 and 8 months post-operatively, our patients were already able to return to work and sport, albeit with varying degrees of discomfort. All patients were able to return to work, as in the series by Cornu, et al. [1]. If one patient had to change job, his new job was still manual, or at least not very strenuous.
Associated lesions such as nerve damage were not found in this study, as some authors have done in the literature [2,4]. Lesions of the extensor tendons were found in 2 patients. After surgical repair of these tendon lesions, we noted that they had no significant influence on functional results.
Subluxation, instability, and osteoarthritis are considered long-term complications and have been reported in other series [19]. The two cases of osteoarthritis observed in our study were due, in one case, to radial epiphyseal collapse and, in the other, to radio-ulnocarpal osteochondral lesions and scapholunate instability that had gone unnoticed. These were long-term residual complications following surgery that the patients had tolerated. The patients concerned had resumed their activities with these arthrosic complications. However, we discussed with them the possibility of arthrodesis, radiocarpal prosthesis or first row carpectomy.
Residual stiffness was noted in all our patients from the day after removal of the immobilisation equipment (plaster cast, external fixator). They were corrected by rehabilitation sessions. The rehabilitation sessions in our study were more efficient because our specialist physiotherapist used precise, objective, and gentle techniques. Wrist stiffness following RCD treatment is rare in the literature. Several authors have not reported any cases of wrist stiffness in their series [1,18,20].
A second operation was necessary in two cases. The first was for a recurrence of dislocation three weeks after reduction-osteosynthesis using an external fixator. The external fixator was removed and replaced with a screw plate, and the stability of the construct was enhanced by double ulno-radial pinning. The second operation was indicated because of delayed consolidation with sepsis four months after the first operation. It consisted of osteo-muscular decortication, cancellous grafting and tri-antibiotic treatment following the operation.
In summary, we believe that, given the complexity of the wrist joint, radiocarpal dislocation should be treated early and surgically. Reduction can be manual but must be fixed with a pin and immobilised with a circular cast. Rehabilitation is also of great importance in the management of these injuries.
Radiocarpal fractures and dislocations are rare and serious injuries which are generally managed surgically, requiring optimal lesion description. Functional recovery is often limited, with a risk of stiffness, instability, or osteoarthritis. Complications associated with the treatment are often well tolerated and allow some resumption of manual activity. Even with limited functional recovery and a risk of osteoarthritis and instability, the patient was able to return to work. Overall, our functional results were satisfactory, as demonstrated by follow-up assessments using proven reliability scores. Further studies with a larger sample size are required to confirm the conclusions of our study.
The authors declare no conflict of interest.
The authors declare that all data and materials are authentic and available.
The authors declare that they have received no funding for this study.
UFNY initiated the study. HVF prepared and drafted the manuscript. SGNK corrected the manuscript.