Congenital giant cervical lymphatic malformation are rare tumors. Recent advances in prenatal diagnosis and delivery by ex utero intrapartum treatment (EXIT) have improved prenatal outcome.
An otherwise healthy 35-year-old woman, gravida 5, para 4, was referred to our institution at 25 weeks' gestation with a diagnosis large neck mass in the fetus. Prenatal ultrasound and magnetic resonance imaging (MRI) findings suggested airway obstruction in the fetus. The EXIT procedure attempt to deliver the baby was successful.
Despite prenatal detection and diagnosis of airway compromise in a fetus with a huge cervical lymphatic malformation, securing the fetal airway can be challenging. Large mass can completely distort normal tissue and anatomy.
Cervical lymphatic malformation is a benign congenital malformation with an excessive growth of the lymphatic system that has its genesis in the lack of development of communication between the lymphatic and venous systems. It may be unilocular or multilocular and variable size. The incidence of cervical lymphatic malformation is rare, it is approximately 1/6000 live births [1]. Most common location of cervical lymphatic malformation occur in the neck (70-80%), usually in the posterior cervical triangle [2]. The remainder 20-30% occurs in the axilla, superior mediastinum, chest wall, mesentery, retro-peritoneal region, pelvis and lower limbs [3]. It is known to appear at birth in about 50% of the affected newborns and 90% appear by the age of 2 years. Airway complications, dysphagia, and speech difficulties may develop [4].
A healthy 35-year-old woman, gravida 5, para 4, delivered a 3.03 kg, female infant with a huge right neck mass. Suspicious of fetal right neck teratoma by transabdominal ultrasound during antenatal checkup, patient then proceed for MRI of the fetus at 25 weeks (Figure 1). MRI shows lymphatic malformation with the size of 14 cm × 9 cm × 15 cm. At 37 weeks 3 days, baby delivered via elective ex-utero intrapartum treatment (EXIT) procedure due to the suspicion of compression of the airway. Prior to the EXIT procedure, obstetrics and gynecology aspirated 90 ml of fluid from the mass interpartumly by ultrasound guidance. During the procedure, once obstetrics and gynecology team able to secure the head, pediatric ENT team called for bronchoscope and to secure the airway, the patient intubated using endotracheal tube (ETT) size 3. After the airway secured, umbilical cord clamped then cut. Infant fully delivered.
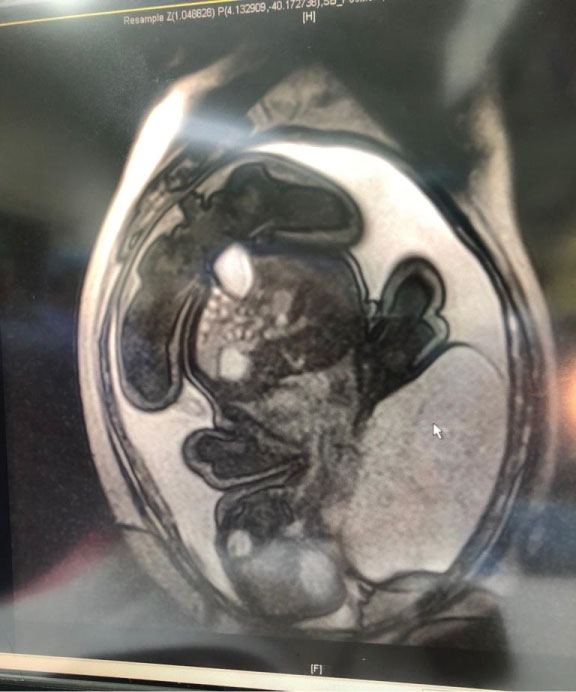 Figure 1: MRI of the fetus at 25 weeks shows lymphatic malformation with the size of 8 cm [AP] × 9 cm [W] × 9 cm [I]. View Figure 1
Figure 1: MRI of the fetus at 25 weeks shows lymphatic malformation with the size of 8 cm [AP] × 9 cm [W] × 9 cm [I]. View Figure 1
Patient kept in the pediatric intensive care unit (PICU) for monitoring. On examination (Figure 2), the mass over right side of the neck, measuring 10 cm [AP] × 14 cm [W] × 14 cm [I]. Day 2 post-partum, patient proceeded for MRI neck (Figure 3). MRI findings shows that there is a huge cystic mass arising from right side of the neck measuring 10 cm [AP] × 14 cm [W] × 13.8 cm [I]. It consists of mainly macrocystic component with few intervening septae. No hemorrhagic component. Occasional enhancing vessels post gadolinium (Gd) series likely represent externa jugular veins and its tributaries. The mass has a broad base and major part of the mass protruding outward. The base is at the right posterior triangle of the neck, spanning from pinna to the supraclavicular area and shoulder.
 Figure 2: Mass over right side of the neck, measuring 10 cm [AP] × 14 cm [W] × 14 cm [I]. View Figure 2
Figure 2: Mass over right side of the neck, measuring 10 cm [AP] × 14 cm [W] × 14 cm [I]. View Figure 2
 Figure 3: Day 2 post-partum MRI neck shows that there is a huge cystic mass arising from right side of the neck measuring 10 cm [AP] × 14 cm [W] × 14 [I] cm. View Figure 3
Figure 3: Day 2 post-partum MRI neck shows that there is a huge cystic mass arising from right side of the neck measuring 10 cm [AP] × 14 cm [W] × 14 [I] cm. View Figure 3
It displaces the right pinna anterosuperiorly, ipsilateral parotid gland, right thyroid lobe and carotid sheath is compressed and displaced medially, otherwise the IJV and carotid artery are patent.
Trachea fairly central. It is abutting the superior aspect of thymus. No extension to the mediastinum or pleura. It also extends posteriorly till midline of posterior neck. Head and neck are tilted to left due to mass effect. The impression from MRI neck is large exophytic lymphatic malformation over the right side of neck, macrocystic type.
Patient then planned for operation on day 8 of life. Otolaryngologist decided to approach the mass via cervical incision. The operation was uneventful. Intraoperative finding: Multilobulated, thin wall cyst measuring about 15 cm × 10 cm at right lateral neck from post auricular extended down to the supraclavicular fossa. Contains straw colored fluid from the cyst. Medially cyst insinuated the carotid artery, jugular vein and vagus nerve. The sternocleidomastoid muscle was stretched and thin out. Histopathological examination (HPE) come back as cystic lymphangioma, patient keep in PICU for 3 days for observation and IV antibiotic, then discharged home. During follow up, the wound properly healed.
Cervical lymphatic malformation are believed to occur as a result of the failure to establish an appropriate connection to the lymphatic channels. They are usually encountered at birth or in early infancy [5]. Neonates diagnosed with a large cervical teratoma are best managed by C-section delivery with EXIT procedure, a specialized surgical procedure that allows the neonate to stay on placental support while their airway is secured. It was first described by Drs Adzick and Harrison in the 1990s as a method for delivering neonates with airway compression [6,7].
In order to successfully perform the EXIT procedure, the participation of multidisciplinary groups, including the specialties of obstetrics, neonatology, anesthesia and head and neck surgery is fundamental [8]. The EXIT procedure was successfully used in cases in which it is possible to anticipate the difficulties related to the access to the neonate's airways [9]. After uterine incision, only the fetal head is delivered. Uterine volume and fetoplacental circulation are maintained, securing oxygenation during access to the airways [10]. Lymphangiomas are divided histologically into two major groups based on the depth and the size of abnormal lymph vessels. The superficial ones are called lymphangioma circumscriptum. The more deep-seated ones are cavernous lymphangioma or cystic hygroma [11].
It is usually multiloculate and contains clear lymph fluid; the wall of the sac is lined by a single layer of flattened epithelium. The cysts are able to intercommunicate with each other and can insinuate between muscle planes, this can lead to compression to other structures. Large lesions can compress many vital structures in the neck like, the sympathetic chain, contents of the carotid sheath and branches of hypoglossal, lingual, and the facial nerves [12].
The possible differential diagnosis of cervical masses are lymphadenitis (caused by mycobacteria tuberculosis, other bacterial and viral infections), inclusion cyst of cervical region including submandibular gland, branchial cleft cyst, laryngocele, haemangioma, lymphoma and congenital vascular malformations [13]. The incidence of lymphangiomas has been reported to range from 1.2 to 2.8 per 1000 newborns [14].
Lymphangiomas may be diagnosed by ultrasound (US) during the intrauterine period. Magnetic resonance (MR) imaging may be useful for a differential diagnosis and evaluation of the mass extent at this time [15]. Although mediastinal extension of cervical masses could be shown with US on neonates, a CT scan is superior to US on the determination of the extent within the thoracic cavity and deep structures of the neck [16]. On a CT scan, they are visualized as cystic masses with a characteristic feature such as an 'enveloping effect' around the trachea, esophagus, great vessels, and even the heart [17]. While cysts frequently have low attenuation values, these values may be variable depending on the nature of the cystic content. MRI are more sensitive than CT scanning and US for the delineation of a lesion's nature and its extension. The relationship with adjacent vessels and muscles may also be able to visualize clearly. Upon MRI, lymphangiomas have typically heterogeneous low signal intensity similar to those of muscles on T1-weighted images and a higher signal intensity than fat on T2-weighted images. However, they may show variable signal intensities due to variable protein content or hemorrhage on T1- and T2-weighted images [16].
Management of giant cystic lymphangiomas which involve head, neck, tongue and oral cavity is always done by surgical excisions [18]. As lymphangiomas are benign lesions, the vital structures should not be sacrificed during their surgical resections [18]. Many times, it may not be possible to completely excise the lymphangiomas in a single sitting and it may require more additional operations [18]. Recurrences are also reported to occur in 5-15% of the cases and additional operations may be required for the excisions of the recurrent lymphangiomatous cysts [18].
Other treatment of choice for the management of cervical lymphatic malformation is sclerotherapy. Previously, sclerotherapy was carried out with sclerosant agents, such as boiling water, quinine, sodium morrhuate, urethane, iodine tenture, doxycycline and nitromin [19]. However, some sclerotherapy agents has been associated with low success rates and frequent complications. Sclerotherapy with intra-lesional bleomycin, as a primary treatment modality, for cervical lymphatic malformation, has been tried. Various case reports and original studies have documented good response to the therapy [20].
The other techniques recently introduced in the management of lymphangiomas are radio-frequency ablation and laser excision of the lymphangiomas. In present time, laser has been increasingly used especially for management of laryngeal lymphangiomas. It causes point destruction of the lesion, at the same time avoiding damage to the adjacent vital structures [21].
Observation is recommended for small, nonexpanding lesions. Surgical resection with complete removal is recommended for lesions that persist, enlarge, or produce obstructive symptoms.
Careful surgical planning is very important to avoid injury to any adjacent tissues and structures, a multidisciplinary approach is warranted.
A team of experienced physicians from varying fields including otolaryngology, pediatric surgery and anesthesia will help to ensure a successful surgical outcome.
We have no conflict of interest to declare.