Current surgical treatment for chronic rhinosinusitis and nasal polyps is functional endoscopic sinus surgery (FESS). Coblation-assisted Functional endoscopic sinus surgery (CAFESS) will probably replace of FESS with more effective result. Our aim was to explore the safety and efficacy of CAFESS for the patients with chronic rhinosinusitis and nasal polyps comparing to traditional FESS firstly by observing clinical data.
The 40-cases in our department with chronic rhinosinusitis with or without nasal polyps were selected randomly from June to September in 2010, and FESS and CAFESS were operated respectively in the experiment group and control group. The patient's subjective symptoms, objective efficacy and the local morphological changes were observed preoperatively and postoperatively for 6-9 months. Statistical analysis was performed using SPSS software.
The symptoms such as nasal stuff, headache and facial pain, pus snot, postnasal drip were relived in both groups. However, blood loss of intraoperative patients in CAFESS group and FESS group were statistically different (P < 0.05), SNOT-20 score and Lund-Kennedy score of postoperative patient in both groups were not statistically different (P > 0.05). The VAS pain score of postoperative patients in CAFESS group and FESS group was statistically different (P < 0.05).
CAFESS is effectively a new surgical technique following functional endoscopic sinus surgery (FESS) for the treatment of chronic rhinosinusitis and nasal polyps, which has a better applied prospect in clinical medicine because of postoperative clinical efficacy superior to FESS.
Controlled-temperature ablation, Chronic rhinosinusitis, Nasal polyp, Functional endoscopic sinus surgery, Coblation-assisted Functional endoscopic sinus surgery
Chronic rhinosinusitis and nasal polyps are the common diseases of otolaryngology that seriously influence the quality of patients' life. So chronic rhinosinusitis and nasal polyps have become one of the focus research in otolaryngology for many years. The cause of chronic rhinosinusitis and nasal polyps is unclear, but most studies believed that may be involved by many factors, and the infection and allergy were the most important factor for the diseases by pathogenic microorganisms [1-4]. From nasal endoscopic surgery (NES) proposed by Messerklinger to functional endoscopic sinus surgery (FESS) proposed by Kennedy, FESS has become the main surgical method for the treatment of chronic rhinosinusitis and nasal polyps. In recent years, controlled-temperature ablation has been used for pharyngeal operation and laryngeal operation successfully in otolaryngology and head and neck surgery [5-8]. However, this technique has not been used for functional endoscopic sinus surgery. In this study, we firstly proposed a novel surgical method which applied controlled-temperature ablation to FESS in clinical cases with chronic rhinosinusitis and nasal polyps, comparing with the traditional FESS surgery. The novel surgery named CAFESS (coblation-assisted FESS). It is aimed to explore the security, reliability and feasibility of novel CAFESS in clinical application, which will provide a novel theory and reliable clinical data that controlled-temperature ablation used in the FESS surgery.
The patients were randomly selected from the department of otolaryngology in Dalian municipal central hospital between June and September in 2010. The study for collecting human tissue samples was approved by the ethical committee of Dalian municipal central hospital, China. The number appointed to the study: YN201400401. A written informed consent was obtained by all patients. The Clinical cases collected and excluded were following the standard [9].
40 patients were selected as the experimental group applied with CAFESS, and another 40 patients were selected as the control group applied with FESS. The selected patients had the different degree symptoms such as nasal congestion, runny nose, headache and hyposmia. All the patients were examined by nasal endoscopy and coronal CT in sinus, and clinical classification and stage were based on FESS-97 [10] (Table 1). From Table 1, it is obviously clear that we have exclude the interference of age and gender, and all the surgery for the patients were completed by the same skilful and qualified surgeon.
Table 1: The details of the patients in the two groups. View Table 1
The patients in CAFESS group were mainly applied with Messerklinger surgical procedures [11]. After patients were anesthetized generally through oral intubation, the cotton sheets with 1% tetracaine and epinephrine were used for local infiltration and shrinking nasal mucosa under nasal endoscopy. Based on nasal imaging endoscopic imaging system (Germany STORZ Corporation) and different clinical classification and stage, nasal polyps were removed by EIC 8872 (Arthrocare Coblator Ⅱ, US) with controlled-temperature ablation. If the lesions invaded the patients' maxillary sinus, all or part of the uncinate was removed along the front edge of uncinate and corresponding sinus lesions was opened at the end of uncinate, and then sinus lesions were removed and reversible inflammatory mucosal lesions were retained under 30° or 70° endoscopy; if the lesions only invaded the ethmoid without invading the maxillary sinus, the corresponding sinus lesions was directly opened without removing the uncinate. All the patients were packed with a small amount of gelatin sponge in the middle meatus, and no nasal cavity was packed. The patients in FESS group were also applied with Messerklinger procedure, and all the patients were filled with swelling sponge in surgical cavity after surgery.
The patients in the CAFESS group were started to clear the nasal cavity on postoperative 24 h for retaining nasal ventilation. Roxithromycin and prednisone were given orally from postoperative 24 h~48 h for 6 days. The nasal cavity was cleaned again on the 8th day after surgery, and all the cases were started nasal spray with Budesonide aerosol for three months. All the patients after endoscopic examination were checked once a week in the first month after surgery, and then once every two weeks in the second month and once a month after the third months until nasal mucosa recovered normally. The patients were seen at a 6~9 month post-operative visit. The patients in the FESS group were dealed with the same method as the CAFESS group except that the packs were removed in surgical cavity after post-operative 24 h~48 h [12,13].
The assessment indexes of postoperative efficacy included subjective efficacy evaluation and objective efficacy evaluation.
About the subjective efficacy evaluation, we selected the SNOT-20 (Sino-Nasal Outcome Test) as local scale survey of specific disease from clinical outcome of laboratory tests by Washington University School of Medicine [14]. All the patients were scored through SNOT-20 scale item in the preoperation and postoperation for 6 months; and we selected the visual analogue scale (VAS) as the evaluation of postoperative pain [15].
About the objective efficacy evaluation, the amount of bleeding in two groups was compared with using gravimetric technique by the hydrometer. The calculating formula was: Blood loss or blood water content (ml) = The total amount of bloody water × (proportion of bloody water - proportion of normal saline)/(proportion of the patient's blood - proportion of normal saline). Because Lund-Kennedy score was commonly the most useful method on evaluating the size of nasal polyps and sinusitis, especially for the changes of postoperative surgical cavity, so we selected Lund-Kennedy score standard as the assessment of nasal diseases changes with nasal endoscopy preoperatively and postoperatively [16,17]. To evaluate the local histological recovery after surgery, we observed the electron microscopic slices of sinonasal mucosa on the 16th week postoperatively both in the patients of two groups.
Additionally, the standard of postoperative efficacy based on three aspects [10]. If the patients' symptoms disappeared with better nasal sinus opening, sinonasal mucosa epithelization and no purulent secretions under nasal endoscopy, we called "cure". If the patients' symptoms reduced significantly with local edema of sinonasal mucosa, formation of hypertrophy or granulation tissue and a small amount of purulent secretions, we called "improved". If the patients' symptoms didn't improve with adhesion of surgical cavity, sinus stenosis or atresia, formation of nasal polyp and purulent secretions, we called "invalid".
The data were analyzed by ANOVA using SPSS software. Results are reported as mean ± standard deviation, and p < 0.05 was set as statistical significance.
From Table 2, total effective rate in both two groups was 100%. It was obviously that CAFESS and FESS were equally effective for the treatment of chronic rhinosinusitis and nasal polyps.
Table 2: Comparison of postoperative efficacy evaluation. View Table 2
It can be seen from Table 3, the comparison of SNOT-20 between the two groups was not statistically significant, but the difference of SNOT-20 was statistically more significant between preoperative value and postoperative value among each group (p < 0.05). These data showed both CAFESS and FESS were more effective for the treatment of chronic rhinosinusitis and nasal polyps, moreover, the patients' clinical symptoms with chronic rhinosinusitis and nasal polyps were relieved obviously after postoperation for 6 months.
Table 3: The comparison of the patients' subjective and objective indexes preoperatively and postoperatively between two groups (x ± s). View Table 3
From the analysis of VAS Score, the comparison of VAS between the two groups was more significant (p < 0.01). So CAFESS was more effective than FESS in relieving the patients' pain, and the patients would like to accept the CAFESS comfortably because there was no nasal packing after surgery.
From the analysis of blood loss, the comparison of blood loss between the two groups was more significant between the two groups (p < 0.01). So CAFESS was more effective obviously than FESS in reducing the patients' blood loss.
It can be also seen from Table 3, the comparison of Lund-Kennedy Score between the two groups was not statistically significant, but the difference of Lund-Kennedy Score was statistically more significant between preoperation and postoperation among each group (p < 0.05). These data showed both CAFESS and FESS were more effective for the treatment of chronic rhinosinusitis and nasal polyps. The condition of patients' recovery was observed with nasal endoscopy in the course of followed up after surgery in CAFESS group (Figure 1).
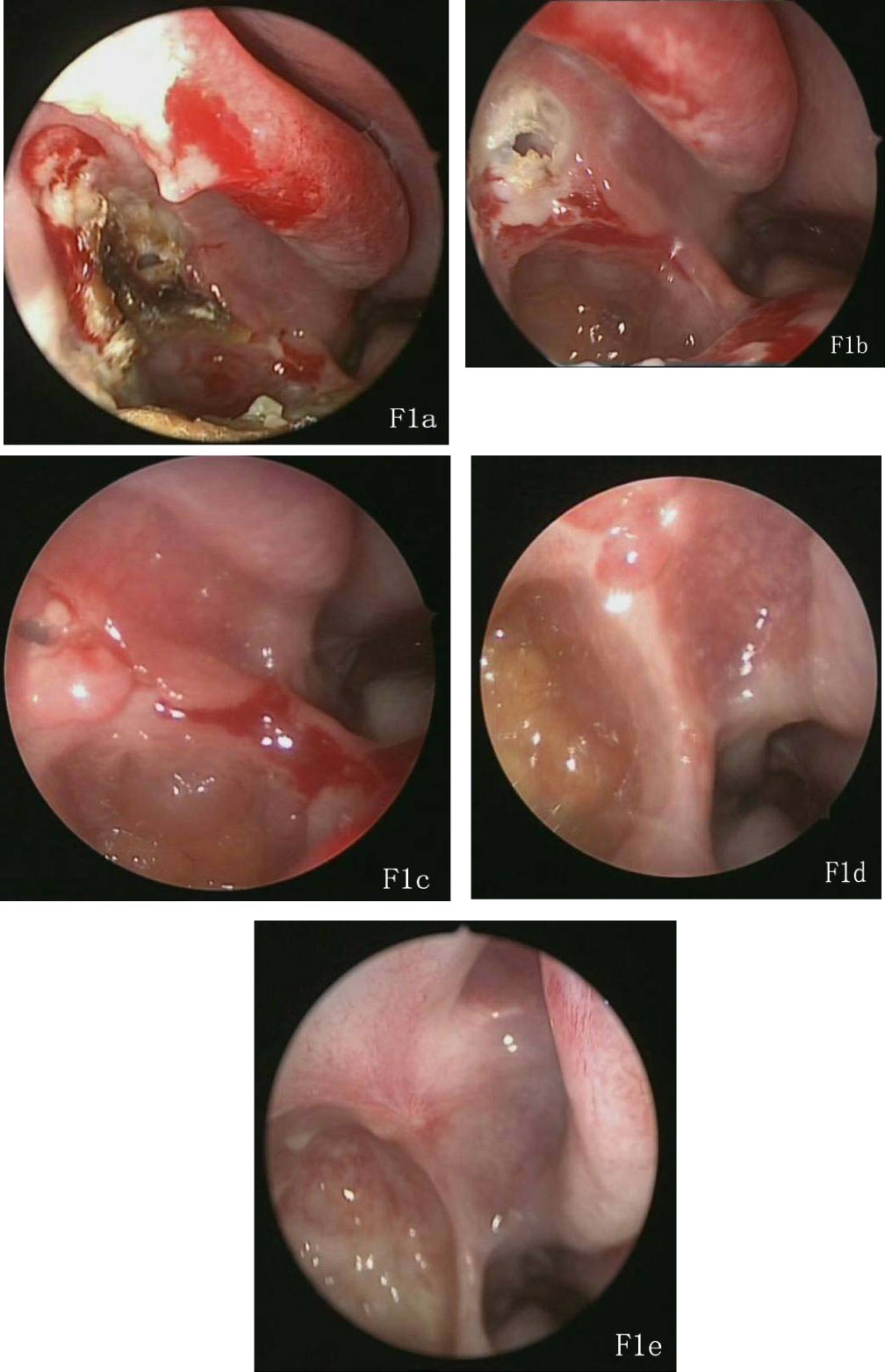 Figure 1: The changes of postoperative recovery in CAFESS group.
Figure 1: The changes of postoperative recovery in CAFESS group.
a) The formation of dry scab and pseudomembrane after postoperative 2 weeks; b) Dry scab obviously reduced after postoperative 4 weeks; c) The formation of follicular with sinus mucosal edema after postoperative 6 weeks; d) Follicular obviously reduced still with mucosal edema after postoperative 8 weeks; e) Surgical cavity has been completely epithelialized after surgery than 12 weeks. View Figure 1
Comparison of Local histological observation
From the Local histological observation with transmission electron microscopy after surgery for 16 weeks, neat and regular cilia formation can be seen obviously on the surface of epithelial cells and the mucosal epithelium arranged regularly. Additionally the nucleus and organelles could be also seen clearly in the CAFESS group (Figure 2a). In the FESS Group, lots of cilia covered on the epithelial cells and arranged in order, moreover nucleus and organelles could be also seen clearly (Figure 2b). There is no significant difference in the nasal mucosa recovery after surgery between the two groups.
Figure 2: The comparision of postoperative recovery in nasal mucosa between the two groups.
a) Neat and regular cilia formation can be seen obviously on the surface of epithelial cells and the mucosal epithelium arranged regularly. Additionally the nucleus and organelles could be also seen clearly after surgery for 16 weeks in the CAFESS group; b) Lots of cilia covered on the epithelial cells and arranged in order, moreover nucleus and organelles could be also seen clearly after surgery for 16 weeks in the FESS group. View Figure 2
Chronic rhinosinusitis and nasal polyps have been treated through surgery for more than 120 years. However, surgical cavity is narrow and surgical vision is limited because the anatomical location of the sinuses is in the deep parts of the craniofacial region, which have brought lots of difficulties on nasal surgical treatment. Sinus surgery has entered into a new stage of development since nasal endoscopy were produced by Germany Wolf company in 1971, which made nasal endoscopic sinus surgery replace the traditional sinus surgery. Kennedy proposed a new concept of functional endoscopic sinus surgery (FESS) for chromic sinusitis and nasal polyp in 1980s, which promotes minimally invasive surgery apply to the nasal sinus surgery with endoscopy wildly and rapidly [18,19]. After decades of development, functional endoscopic sinus surgery (FESS) technology and theory have bring to a new stage development of nasal science on researching clinical sinus surgery and basic nose science.
Controlled-temperature ablation was a new minimally invasive surgery widely applied on otolaryngology over the past decade. The application of controlled-temperature ablation in FESS surgery was a inevitable combination between minimally invasive approach and minimally invasive concept. Coblation-assisted FESS (CAFESS) was the application of controlled-temperature ablation under nasal endoscopy and followed the connotation of FESS technology in order to achieve the purpose of healing, which cleared the lesions, reserved reversible inflammatory mucosal lesions, improved and rebuilt the ventilation and drainage channels of nasal cavity and paranasal sinuses with keeping the basic structure of nasal cavity and paranasal sinuses possibly.
In this study, the cure rate was 95% in CAFESS group, while the cure rate was 92.5% in FESS group, and total effective rate in both two groups was 100%. The result was is consistent with the report that the cure rate was 80%-90% in the western countries [20]. Although SNOT-20 scores and Lund-Kennedy score had no significant difference preoperatively and postoperatively between the two groups, the significant difference within the group showed the treatment with CAFESS was as effective as treatment with FESS. The major clinic symptoms were significantly improved, and blood loss of the patients in CAFESS group was obviously less than that in FESS group.
We consider that controlled-temperature ablation operated at low temperature with flushing a large number of normal saline, which can avoid damage to other normal tissues in the nasal cavity and reduce bleeding. And less blood loss in the operation made the surgical views clearly and operated accurately, which could shorten the operation time and reduce the difficulty and risks of surgery [21]. In our study, less blood loss of patients without any complications in CAFESS group fully proved minimally invasion of CAFESS was safe and more feasible for application in clinical medicine. The difference of postoperative VAS score between two groups reflects CAFESS could reduce the patients' pain without any postoperative nasal packing, and it was easy for patients to accept [21]. In local histological observation, the result showed both CAFESS and FESS for the treatment of nasal sinusitis and nasal polyps were effective, because no obvious difference was found on the pathological changes of the local tissue between two groups.
Thus, CAFESS is a viable new surgical method following FESS for the treatment of chronic rhinosinusitis and nasal polyps. The Arthrocare Coblator Ⅱ surgery system used in CAFESS could reach the position and angle which common cutting systems can't reach, and based on the advantages of FESS surgery and combined with the advantages of controlled-temperature ablation, CAFESS represent the future development of minimally invasive surgical techniques. Especially patients with Ⅰ type (1, 2 stage) and Ⅱ type (1, 2 stage) were more suitable for CAFESS application because of better result in our study. However, the limited clinical cases and the short follow-up time in our study require that we still need continue further study which should enlarge the clinical samples and observe the long-term consequent for the application of CAFESS.
Conceived and designed the experiments: NNZ MTZ QFZ
Performed the experiments: NNZ DLL CPS MTZ WS QFZ
Analyzed the data: NNZ MTZ QFZ
Wrote the paper: NNZ MTZ QFZ.