Aspergillosis of the sphenoid sinus is a rare condition. The causative agent is most often Aspergillus fumigatus. We report this case of an immunocompetent 16-year-old woman with no specific medical history who presented with severe chronic headache, retro orbital pain, associated with nasal obstruction. The clinical examination showed a polyp filling the left nasal cavity with a left exophthalmos. The CT scan showed a heterogeneous left sphenoid sinus lesion with calcifications inside it. In magnetic resonance imaging (MRI), this lesion was in T1 isosignal, heterogeneous T2 hypersignal and enhanced heterogeneously by gadolinium. A left sphenoidotomy by endoscopic endonasal approach was performed. Mycological examination revealed aspergillary mycelial filaments. The pathology examination confirmed the diagnosis of aspergillosis. The evolution was favorable with disappearance of the headaches after a decline of one year.
Sphenoid aspergillosis is difficult to diagnose clinically due to its rarity and misleading clinical manifestations. The interest of the CT scan is to orient the diagnosis in the presence of intra-sinus calcifications. Early and adequate treatment is the only guarantee of success.
Sinusitis, Sphenoid sinus, Aspergillosis
Sphenoidal aspergillosis is a rare condition that is difficult to diagnose. The most common pathogen is the Aspergillus fumigatus. The symptomatology is non-specific. We report a case of sphenoidal aspergillosis in a young immunocompetent patient.
A 16-years-old women, with no specific pathological history, more specifically no diabetes or allergy, and no history of prolonged corticosteroid use. She'd been suffering during 4 months before consulting from an intense and recurrent headache associated to retro-orbital pain and a unilateral nasal obstruction (left side), with no other ENT or general signs: No epistaxis nor posterior snuffles nor blurred vision or fever. The patient had a good general condition.
The clinical examination using an nasal endoscopy found a polyp filling the left nasal cavity, it's origin couldn't be individualized. The rest of the clinical examination was clear. The ophthalmological examination found a discrete left exophthalmos with no visual disturbance.
Biological tests were normal, in particular, blood count and sedimentation rate. The facial CT scanshowed a revealed a spontaneously heterogeneous left sphenoidal and ethmoid-nasal lesional process with calcifications inside it, with discrete homolateral exophthalmos (Figure 1). The MRI found a sphenoidal and ethmoid-nasal left polylobed process isosignal in T1, hypersignal in T2 and heterogeneously enhanced by gadolinium (Figure 2).
 Figure 1: Facial CT scan showed left sphenoidal and ethmoido-nasalpolyp with calcifications inside, with homolateral exophthalmos.
View Figure 1
Figure 1: Facial CT scan showed left sphenoidal and ethmoido-nasalpolyp with calcifications inside, with homolateral exophthalmos.
View Figure 1
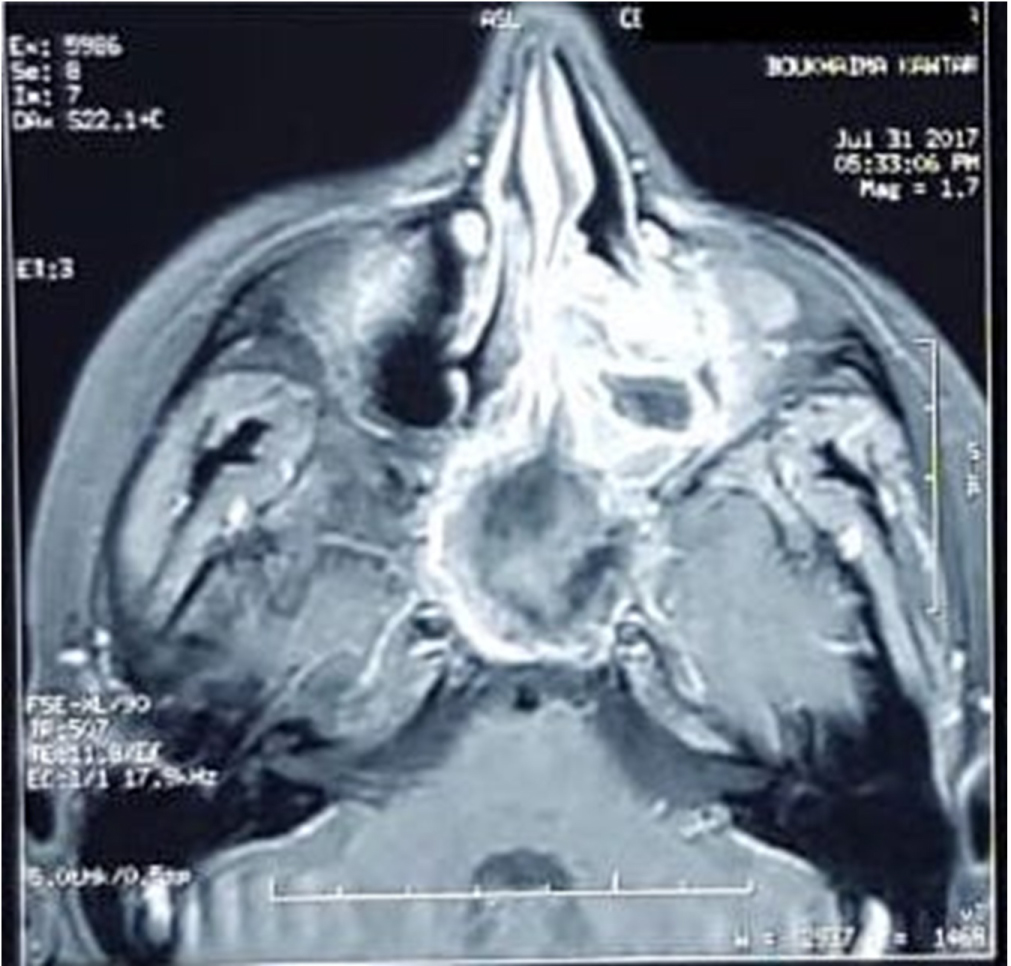 Figure 2: MRI showing sphenoidal polyp isosignal in T1, hypersignal in T2 and heterogeneously enhanced by gadolinium.
View Figure 2
Figure 2: MRI showing sphenoidal polyp isosignal in T1, hypersignal in T2 and heterogeneously enhanced by gadolinium.
View Figure 2
The patient underwent endoscopic endonasal surgery, she underwent a sphenoidotomy with a left ethmoidectomy. The surgical exploration found a polyp emanating from the left sphenoidal sinus which was completely filled with blackish mycotic truffles (Figure 3). A good and careful cleaning of the sphenoid sinus cavity was performed with aspirating of the aspergillar truffles.
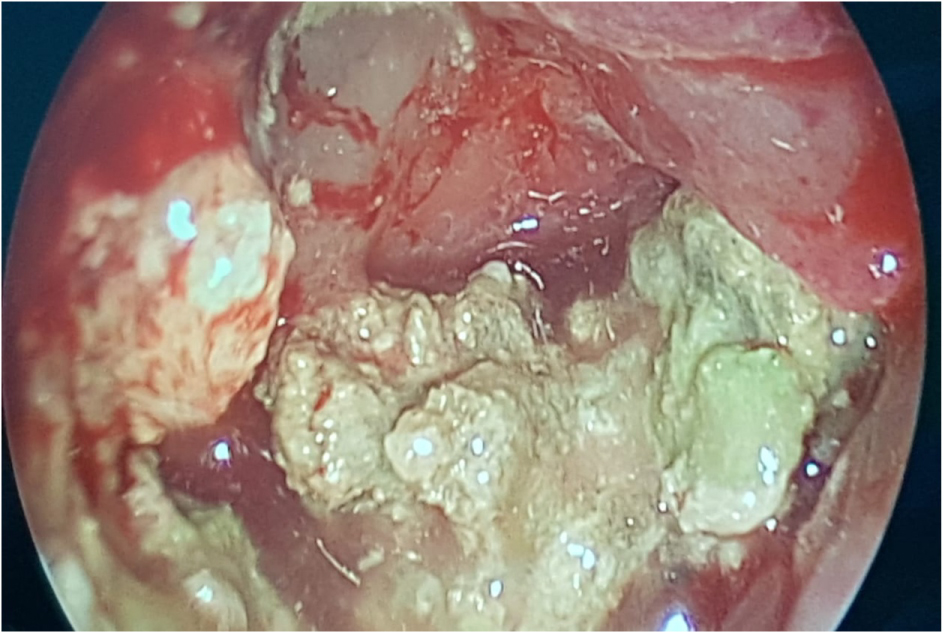 Figure 3: Per-operative view of sphenoid sinus showing polyps which was completely filled with mycotic truffles.
View Figure 3
Figure 3: Per-operative view of sphenoid sinus showing polyps which was completely filled with mycotic truffles.
View Figure 3
Direct mycological examination revealed the presence of mycelial filaments with aspergillar heads. The culture was negative.
Pathological examination confirmed the diagnosis of aspergillosis by showing aspergillar mycelial filaments.
The postoperative sequelae were simple. The evolution was favorable with disappearance of the headaches after one year.
Aspergillosis is caused by a ubiquitous germ of the genus Aspergillus with predominance of the fumigatus and flavus species [1,2]. The sphenoidal location of this infection is exceptional [3]. Indeed, the aspergillar spores usually colonize the proximal para-nasal sinuses.
Clinically, the signs are often fleeting and the presentation is non-specific. The major calling sign is the headache with a predominantly retro-orbital pain [4,5]. Rhinological signs are dominated by purulent rhinorrhea and nasal obstruction. In invasive forms, the clinical presentation is dominated by ophthalmological signs (diplopia, ptosis, exophthalmos, ophthalmoplegia, blindness) caused by the orbital extension and invasion of the cavernous sinus. Neurological and endocrine signs by contiguous invasion of the adjacent neuro-meningeal structures [6].
CT scan shows heterogeneous hyperdense sinus filling, that does not rise after injection of contrast material, with calcifications . The study of the bone window allows the search for localized bone reshaping or bone lysis observed in invasive forms [7].
The MRI shows a heterogeneous lesion in T1 and T2 that is not enhanced after gadolinium injection, with a very hypo-intense area on T1 and T2. It is mostly interesting in the evaluation of possible orbital or meningoencephalic invasion [7,8].
In the absence of diagnosis or effective treatment, functional and sometimes vital complications may occur, such as rupture of the internal carotid artery within the cavity, pan hypopituitarism or damage to the central nervous system [3,5,9].
The treatment of aspergillosis of the sphenoidal sinus is surgical and relies on endoscopic sphenoidotomy. It allows the drainage of a purulent greenish liquid in which the characteristic aspergillar masses are located. In case of immunosuppression, it must be combined with systemic antifungal treatment [5,8,10].
In the non-invasive forms, the evolution is favorable with no recurrence if the exeresis has been complete. On the other hand, in the invasive forms with an immunocompromised background, the prognosis is serious [5,11,12].
Sphenoidal aspergillosis is difficult to diagnose clinically because of its rarity and clinical manifestations. The interest of the scanner is to orient the diagnosis in the presence of intra-sinusal calcifications. Early and adequate management is the only guarantee of success.
The authors declared that there is no conflict of interests.
M Elbouderkaoui, Y Lakhdar: Diagnosed the patient; A Raji, H Nouri, Y Rochdi: Treated the patient; S Rochd: Obtained consent.
M Elbouderkaoui, Y Lakhdar: Wrote the majority of the manuscript; SRochd: Contributed to case report writing and iconography; A Raji, H Nouri: Critically reviewed the manuscript.
Informed consent was obtained from the patient for publication of this case report and accompanying images.
None.