Globus pharyngeus is a common benign condition. Patients with this condition are commonly investigated to exclude the risk of upper aero-digestive malignancies. One of the investigations carried out is barium swallow. However, there is great debate regarding the role of barium swallow in the diagnosis of head and neck cancers. Therefore, the aim of this study is to review the validity of barium swallow in diagnosing malignancies. All patients diagnosed with head and neck cancer between January 2010 and December 2014 in North Wales were included in the study (708 patients). Results showed that 35 patients had barium swallow before the diagnosis of cancer. Barium swallow suspected malignancy in only 5 patients and missed the cancer diagnosis in 30 patients. Therefore, the study confirms that that barium swallow has a very limited sensitivity and specificity in diagnosing head and neck cancer. In conclusion, barium swallow should not be requested routinely as part of the investigation of cases suspected to have head and neck cancer. This approach will reduce the cost and radiation effect of unnecessary investigations.
Globus pharyngeus is a common condition which represents 3-4% of new referrals to the ENT outpatient clinic [1-3]. It is defined as a feeling of a 'lump' in the throat. The exact aetiology and management of the condition remains unclear [4]. Furthermore, there is a lack of consensus about the role of any investigation in its management [2]. The main aim of investigating patients with globus is usually to eliminate upper aero-digestive malignancies.
Barium swallow is the most commonly used non-invasive method of investigation. However,most of these contrast investigations usually fail to demonstrate any serious pathology. Therefore, the aim of this study is to review the barium swallow reports carried out for patients diagnosed with head and neck cancer before the date of diagnosis.
The study includes all patients diagnosed with head and neck cancer in Betsi Cadwaladr University Health Board between January 2010 and December 2014. This data has been retrieved from the Head and Neck service in Ysbyty Gwynedd in Wales, UK.
Table 1 illustrates all 708 head and neck cancer patients included in the study. From these patients, 262 (37%) were females and 546 (77%) were males. Thyroid cancer is more common in females (68%).
Table 1: Head and neck cancer categories (2010-2014). View Table 1
Table 2, highlights the number of head and neck cancer patients diagnosed in each hospital within the trust respectively. The three main hospitals in the trust are Ysbyty Glan Clawd, Wrexham Hospital and Ysbyty Gwynedd.
Table 2: Head and neck cancer patients diagnosed in each hospital (2010-2014). View Table 2
In order to ensure that the barium swallow was carried out before the date of diagnosis, all 708 head and neck cancer cases were revised through the PACS synapse radiology system. Therefore, any case which had barium swallow after diagnosis of head and neck cancer or as part of the follow up of surgery or complication of treatment had been excluded from thestudy.
From these 708 patients, a total of 35 had a barium swallow prior to the date of diagnosis of head and neck cancer. Out of the 35 patients, 30 were deemed to not have any head and neck cancer and it was only later picked up by other sensitive investigations; Computed Tomography (CT) and Magnetic Resonance Imaging (MRI). As a result of this false reassuring reports, the diagnosis of cancer had been delayed. In the remaining 5 cases, the barium swallow report recommended further investigations and rose suspicion of cancer. Three of these 5 patients had previous throat cancer. One patient had fungating filling defect in the hypopharynx and upper oesophagus. The last one had thyroid mass pressing on the pharynx.
Our data shows that the sensitivity of barium swallow in diagnosis of head and neck cancer is 15%. Barium swallow has very high false negative results (Figure 1).
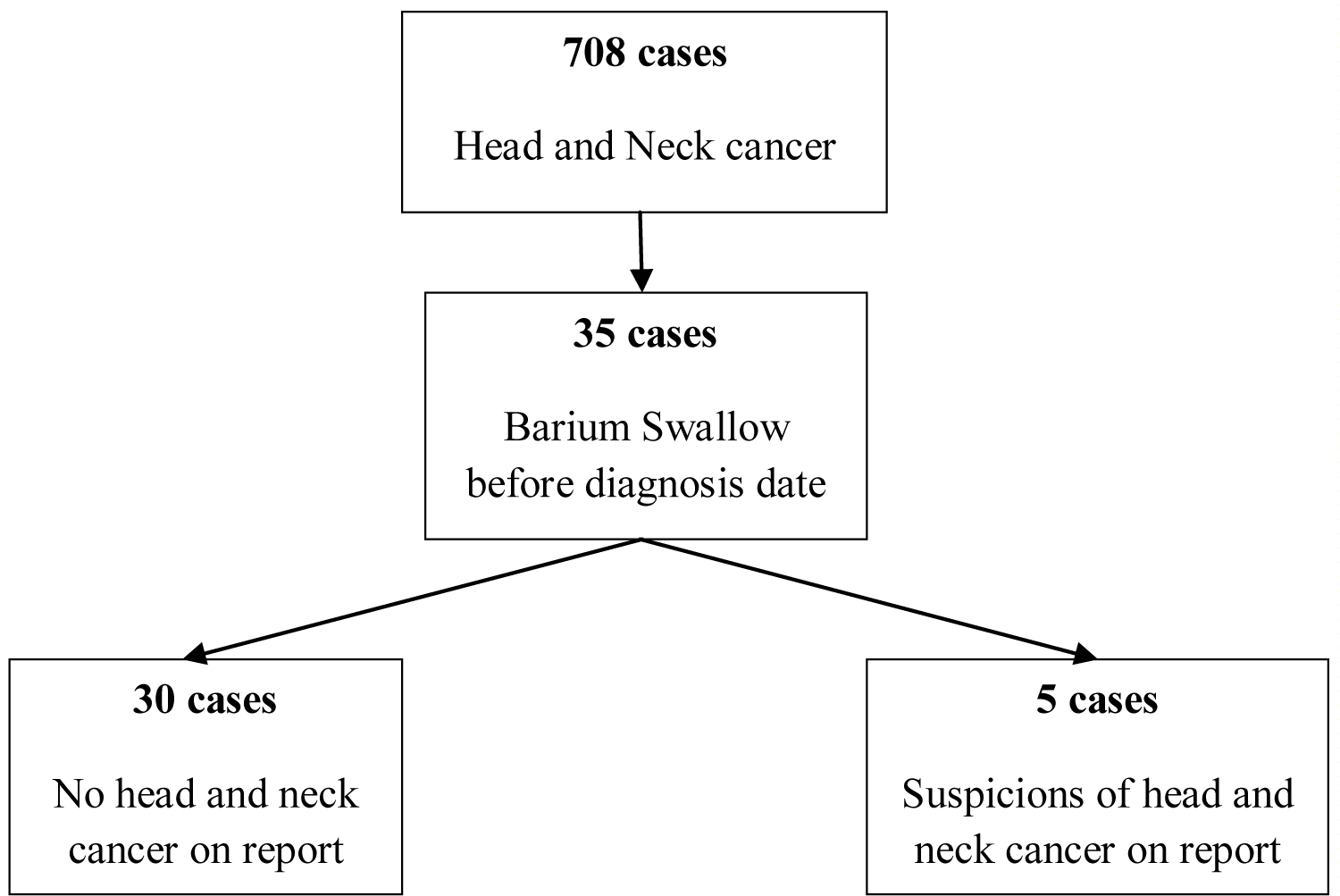 Figure 1: Summary of head and neck cancer diagnosis based on barium swallow reports.
View Figure 1
Figure 1: Summary of head and neck cancer diagnosis based on barium swallow reports.
View Figure 1
Globus pharyngeus is a common problem of uncertain aetiology and of controversial management. Patients with this condition are commonly investigated to exclude the risk of upper aero-digestive malignancies. Around 45% of the general population experience globus sensation at some point in their lifetime [5,6]. Several factors are thought to be responsible including; cricopharyngeal spasm, lingual tonsil, granular pharyngitis, cervical osteophytosis, Gastroesophageal Reflux Disease (GORD), hiatus hernia, sinusitis, postnasal drip, goitre and finally psychiatric causes [6]. The clinical examination is almost always unremarkable. The relationship between GORD and globus is very controversial.While some studies identify a strong association, others deny such a relation. The reported association varied from 11% [7] to 55% [8]. The association of both hiatus hernia and reflux with globus is estimated to be 2-3% [9]. In another study of 116 barium swallow, cervical osteophytosis was found in about one third of the patients [10].
Barium swallows are usually requested to exclude pharyngeal and upper oesophageal neoplasia in patients with globus [7]. This is mainly to reassure patients and to eliminate serious pathology [10]. The sensitivity of barium swallow to diagnose small upper digestive tumours is low and it is reported that it may fail to detect 50% of the hypopharyngeal carcinoma [4]. In a study of 2,011 barium swallow of patients with globus, no serious pathology was detected. Furthermore, no patients were diagnosed with cancer following 2 to 7 years of follow-up [9]. Extensive review of literature failed to identify any patient with globus diagnosed with upper aero-digestive malignancies [2,3,7]. Therefore, the indication of barium swallow in typical globus pharyngeus patients is very doubtful due to the investigations low sensitivity to detect small tumours. The investigation has both a radiation risk and cost implications. The radiation amount of one barium swallow study is equivalent to 75 chestX-rays [2]. The cost of each barium swallow is about £200. Therefore, this investigation is not considered cost-effective.
The management of globus is unclear as it is considered to be predominantly a clinical diagnosis requiring no investigation the majority of the time [2]. Current guidance suggests that in the presence of globus without any risk factors and normal clinical examination, there is no indication for further investigation unless the symptoms persist [7]. Despite this, a questionnaire study about the management ofpatients with typical symptomsof globus pharyngeus showed that 14% of the UK consultants perform no investigation. The remaining consultants suggest carrying out the following investigations; rigid endoscopy (61%), barium swallow (56%) or a combination (14%) [4]. A study suggested that Globus should be managed with a 1-month course of antacid to patients with typical globus followed by investigation if the symptoms persist [5].
Small post-cricoid carcinoma can be missed by barium swallow and only rigid endoscopy can confirm the final diagnosis [4]. Comparing rigid endoscopy, flexible endoscopy and barium swallow, the first is considered the most sensitive diagnostic test for the upper aero-digestive tract malignancies [11-13]. Flexible oesophagoscopy may miss hypopharyngeal tumours and the rigid endoscopy is essential in these cases [14].
Patients with upper aero-digestive tumours typically divided into two groups based on tumour size. The first group includes patients with large tumours and the diagnosis is usually obvious on clinical examinationand fiberoptic examination. In our study, the only 2 primary cancer cases diagnosed with barium swallow could have been diagnosed by complete clinical examination with fiberoptic examination without the need for barium swallow. The second group includes patients with small tumours and negative clinical signs. Barium swallow usually will fail to diagnoses these small lesions. For this group, more sensitive investigations; MRI scan and CT scan should berequested.
The study confirms reduced validity of barium swallow in globus pharngeus and head and neck cancer patients. For example, a patient diagnosed with a T4a cancer tongue base was missed by barium swallow. In another case, barium swallow suspected a lesion on the right side whereas the MRI scan confirmed a large mass on the left side.
Our study is clearly showing that barium swallow is not helpful investigation for patients presented with symptoms suspicious for cancer.
The role of barium swallow in the management of globus pharyngeus is controversial. Barium swallow is usually prescribed to exclude the presence of upper aero-digestive malignancies. It has low sensitivity to diagnose small pharyngeal and oesophageal tumours while larger tumours are usually obvious on clinical examination.