Intratonsillar abscess (ITA) is a rarely reported clinical entity in both children and adults. Despite its rarity ITA should be considered in the differential diagnosis of Peritonsillar abscess and Tonsillitis. CT scan is useful to confirm the presence of an ITA. The following case series summarizes three cases of intratonsillar abscess that presented to our centre and their management. The primary treatment modality in our cases involved needle aspiration with post-procedural antibiotics.
Intratonsillar abscess, Needle aspiration, Tonsillectomy
ITA: Intratonsillar Abscess; WBC: White Blood Cell Count
Tonsillitis is a common pharyngeal infection in children and young adults, however intratonsillar abscess is a rare complication associated with it. Intratonsillar abscess is characterized by formation of abscess in the parenchyma of the tonsil. The literature reports only about 29 cases of intratonsillar abscess [1]. The clinical features may resemble tonsillitis or peritonsillar abscess, and radiological imaging may be required to confirm the diagnosis. Treatment modalities may vary from IV antibiotics, needle aspiration, incision and drainage to tonsillectomy. In our study we emphasize that needle aspiration under antibiotic cover would suffice as primary treatment with consideration of surgical intervention in cases of recurrence.
The following are the cases encountered in our setup and a brief discussion of this entity.
A 35-year-old woman presented to our ENT Out Patient Department with complaints of recurrent episodes of swelling and pain in the right tonsillar region and odynophagia for a duration of 1 month. On examination: the patient was afebrile (96.7 °F) with pulse rate of 92 beats per minute and blood pressure of 116/76 mmHg. A complete ENT examination revealed a pale yellow swelling seen in the substance of right tonsil 4*5 cm, medially extending up to the midline, it had a soft, cystic consistency and was tender on palpation as in Figure 1a and Figure 1b. Rest of the oropharyngeal examination was normal. Neck examination showed palpable, jugulodigastric lymph node 2*1 cm, mobile tender, soft.
 Figure 1a: Showing a pale yellow swelling seen in the substance of right tonsil.
View Figure 1a
Figure 1a: Showing a pale yellow swelling seen in the substance of right tonsil.
View Figure 1a
 Figure 1b: Follow up status on day 7.
View Figure 1b
Figure 1b: Follow up status on day 7.
View Figure 1b
Patient's complete haemogram showed WBC of 13,800 cells/mm3 with normocytic normochromic blood picture while the C-reactive protein was negative. The diagnosis was then confirmed by CT scan of Head and Neck which showed a ring enhancement in the right tonsil. Subsequently the patient was treated with needle aspiration of the abscess and IV antibiotics (Inj. Amoxycillin 1g + clavulinic acid 200 mg 12th hourly & Inj. Metronidazole 100 ml 8th hourly) for 7 days. The aspirate was sent for culture sensitivity which did not grow any organism; we attributed it to the most likely fact that the patient had been treated with 2 courses of antibiotics in the preceding 20 days. Following this the patient has been on for regular follow up with no further episodes.
A 34-years-old male patient came with fever of 3 days duration and right sided throat pain and odynophagia since 1 week. His vitals were within normal limits. On examination, right sided tonsillar swelling measuring 1*1 cm with hyperemia of unilateral oropharyngeal structures was seen as depicted in Figure 2a and Figure 2b. No palpable neck nodes were found. Investigations showed WBC count of 14,300 cells/mm3 with peripheral neutrophilia. Patient was subjected to needle aspiration and pus retrieved was sent for culture sensitivity which reported the growth of staphylococcus aureus. Sensitivities showed the efficacy of ceftazidime, amoxicillin & clavulinic acid. Tab Cefpodoxime 200 mg + Clavulinic acid 125 mg bid with analgesics were prescribed was given. Patient was free of symptoms in 7 days with no complications.
 Figure 2a: Showing the intratonsillar abscess in the right tonsillar region.
View Figure 2a
Figure 2a: Showing the intratonsillar abscess in the right tonsillar region.
View Figure 2a
 Figure 2b: Patient came to us for follow up on day 7.
View Figure 2b
Figure 2b: Patient came to us for follow up on day 7.
View Figure 2b
A 30-year-old female patient, presented to us with throat pain, odynophagia and difficulty in opening mouth progressively over 10 days. On Clinical examination patient was afebrile (95.3 °F) with pulse rate of 86 beats per minute. On ENT examination had grade 1 trismus grade 1 with congested oropharynx and right tonsil showing 2*2 cm swelling as shown in Figure 3a and Figure 3b. Neck examination revealed a 1.5*2 cm soft in consistency, mobile tender level II lymph node. Blood investigations revealed leucocytosis (WBC count- 14,400 cells/mm3) with peripheral neutrophilia and negative C-reactive protein. On clinical suspicion, swelling was subjected to needle aspiration. Thick 1 cm3 of purulent fluid was aspirated and culture sensitivity done. The culture yielded growth of enterococcus species which were sensitive to amoxicillin & clavulinic acid, augmentin, vancomycin, linezolid, amikacin. Patient was then started on IV Amoxycillin 1g + clavulinic acid 200 mg 12th hourly with supportive fluid and analgesic treatment for 7 days with good clinical response. There were no complications during her hospital stay. Patient was on regular follow up with no signs of recurrence.
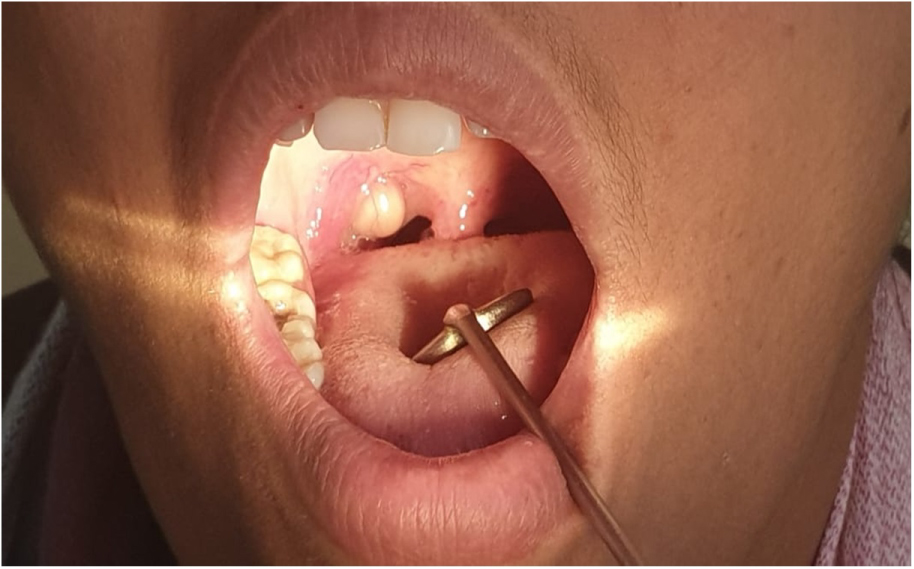 Figure 3a: Localised, yellowish, smooth swelling over the medial aspect of right tonsil with congestion of surrounding tonsillar tissue.
View Figure 3a
Figure 3a: Localised, yellowish, smooth swelling over the medial aspect of right tonsil with congestion of surrounding tonsillar tissue.
View Figure 3a
 Figure 3b: Post-procedural status on day 7 follow up.
View Figure 3b
Figure 3b: Post-procedural status on day 7 follow up.
View Figure 3b
The palatine tonsils are situated at the lateral portions of the oropharynx, each bound by the Anterior (formed by the palatoglossus) and Posterior (formed by the palatopharyngeus) tonsillar pillars. The palatine tonsils are covered by a fibrous sheath of connective tissue laterally and non-keratinized squamous epithelium medially. The medial surface of the tonsil is made up of multiple tonsillar crypts varying from 8-20 in number [2,3].
Intratonsillar abscess formation commonly develops as a sequel of acute follicular tonsillitis. The exact etiology of intratonsillar abscess is obscure. Two major mechanisms postulated in previous studies are extension of a crypt abscess directly into the tonsillar tissue & bacterial seeding into the tonsil through lymphatic or blood borne spread [4].
Michaels and Hellquist suggested that suppurative focus may penetrate inwards potentially leading to the formation of an intratonsillar abscess [5]. Failure of the tonsillopharyngeus muscle to clear debris/food and further localized inflammation are also implicated in some studies [4,6]. In the bacteriology of tonsils, Staphylococcus aureus is the most common pathogen cultured in adults and children; Enterobacter and Escherichia coli in adults; and Streptococcus pyogenes is more prevalent in children [3].
Rapid lymphatic transport from palatine tonsils and the absence of lymphatic valves prior to the capsule may not allow aggregation of bacteria within the tonsillar parenchyma [7]. This may account for the low incidence of ITA and more peritonsillar abscess. Therefore factors which compromise the lymphatic flow may be predisposing factors for ITA, such as dehydration, inflammatory swelling of follicles and previous history of peritonsillar abscess. The incidence of intratonsillar abscess is seen to be about 5% in patients with peritonsillar abscess [4].
Regardless of the mechanisms at play, parenchymal cellulitis in the tonsil is the final result and degree of sepsis and associated factors, as listed above, would probably determine the size and frequency of its occurrence.
This rare entity was first reported in literature by Childs, et al. in 1991, but all the cases had coexisting peritonsillar abscess which is also the case among many other studies [7]. Prevalence of isolated ITA as in our cases is rare and its occurrence, may in fact be higher than reported, as the clinical features are very similar to peritonsillar abscess/peritonsillitis.
Clinically, intratonsillar abscess exhibit palpable tonsillar enlargement, but patients with peritonsillitis/peritonsillar abscess show swollen surrounding tissue, deviated uvula, and have muffled voice [4,8]. In all our cases, clear clinical indication of intratonsillar abscess were seen along with absence of clinical signs such as muffled voice or deviation of uvula or exudates in tonsil and hence a diagnostic CT was not always indicated. CT clinches the diagnosis in times of unclear inference, where ITA in CT scan shows low density ring enhancement within the tonsillar capsule, as depicted in Figure 4, unlike in peritonsillar abscess which shows peritonsillar space involvement [6-8]. Misdiagnosis of intratonsillar abscess may lead to inappropriate treatment and undue complications for eg. if misdiagnosed as peritonsillar abscess, the incision and drainage under antibiotic cover may be excessive and may not facilitate drainage of the intratonsillar abscess.
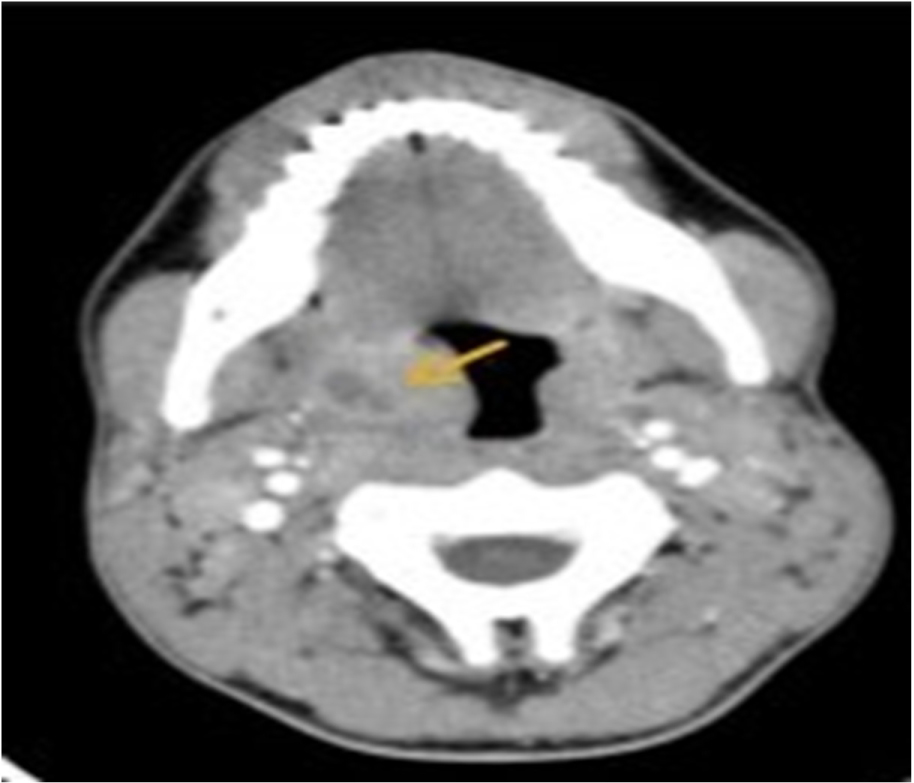 Figure 4: Axial CT imaging demonstrating right intratonsillar abscess.
View Figure 4
Figure 4: Axial CT imaging demonstrating right intratonsillar abscess.
View Figure 4
A recent case series on the cited subject, in children, by Ulualp, et al. has highlighted the role of antibiotics in treatment of ITA with no surgical intervention at all [9]. Clinical response to IV Antibiotic treatment may be determined using the following clinical signs and symptoms: Restitution of general wellbeing, improvement of appetite, improved swallowing, absence of fever, and decline in tonsil size, symmetrical peritonsillar regions with no fullness, normal appearing oropharynx, and decreased trismus. If no clinical improvement is seen after 48-72 hours, surgical intervention could be considered [9].
In our case series however, our first patient came with a month long history during which, she underwent 2 courses of antibiotics as a primary intervention with no improvement in her symptoms and hence we decided on primary incision & drainage followed by antibiotic cover.
Many authors, support needle aspiration under antibiotic cover [10,11]. In our set up we used a wide bore 18 G needle aspiration with post-procedural antibiotic therapy as a primary treatment modality since the procedure was easy, cost effective, and less invasive, avoids the need for a general anaesthesia, and a less painful method while the wide bore needle aids in thorough pus drainage. In children, as standard operating procedure similar to foreign body removal we would prefer to do it under short general anesthesia or sedation followed by post-procedural antibiotics but in this case series all the patients that presented with ITA were adults and hence that was an option we didn't explore since their compliance for the procedure was excellent.
Post-procedural bleeding is a potential complication of this procedure. However in all our cases, post-procedural bleeding was minimal and subsided spontaneously. Too deep an insertion for drainage can puncture large vessels causing increased bleeding and must be done with utmost care [12-14]. Following the drainage, the pus should be always sent for microscopy, culture, and sensitivity analysis thus antibiotic choice can be directed by the microbes cultured and their sensitivity.
If needle aspiration fails, Yaakov, et al. advocated subsequent incision and drainage using general anesthesia if absolutely necessary in conditions such as airway compromise or combination of intratonsillar abscess and peritonsillar abscess [9].
Some authors report children with ITA having undergone tonsillectomy after initial antibiotic therapy [4]. However, we could find no evidence based medicine in favor of tonsillectomy for ITA as a primary modality. In this context, it would be imperative to note that even in peritonsillar abscess; tonsillectomy is no longer regarded as an absolute indication and is recommended for recurrent abscesses only [11].
This case series merits mention on account of the rarity of ITA, its probable underreporting in the medical literature and the need for appropriate management. Although uncommon, Intratonsillar Abscess should be considered and differentiated from clinically similar entities such as peritonsillar abscess or peritonsillitis. A CT scan is not always indicated, although it can be used in times of unclear inference to clinch the diagnosis. Aspiration and drainage under antibiotic cover should be considered as primary modality of treatment and the needle should be placed in the tonsillar parenchyma carefully and not the peritonsillar space. The antibiotic choice can be directed by the microbes cultured and their sensitivity. Abscess Tonsillectomy may be considered in case of failure of treatment or recurrent abscesses only.
None.
None.
None.