Gradenigo's syndrome is a characteristic triad of suppurative otitis media, pain in distribution of trigeminal nerve and abducens nerve palsy. Early diagnosis and management of Gradenigo's syndrome is important as it can give rise to fatal complications. Careful clinical history and physical examination, neuroimaging are needed for a differential diagnosis.
We present a case report of unusual presentation and eitiological cause of Gradenigo's syndrome and its effective management. Patient was managed with prolong antibiotic followed by cortical mastoidectomy for histopathology. The patient responded to prolong antibiotic treatment for 3 weeks after which the lateral rectus palsy completely recovered.
Tuberculosis petrositis has similar presentation like Gradenigo's syndrome and it can be effectively managed with medical line of management avoiding major surgery. Surgery is only required for histopathology for establishing the diagnosis and in resistant and extensive cases where disease clearance is needed.
Gradenigo syndrome, Abducens nerve diseases, Otitis media, Tuberculosis, Petrositis
The syndrome was first by Guiseppe Gradenigo in year 1907 [1]. Before the discovery of antibiotics, it was an uncommon complication, seen due to acute otitis media (AOM) and mastoiditis. The sixth cranial nerve and the trigeminal ganglion are in closely separated by the dura mater at the petrous apex of the temporal bone. The infection spreads to this area and gives rise to the characteristic triad of symptoms. Extradural inflammation secondary to apical petrositis can affect the sixth nerve by inflammation as it passes through the Dorello's canal under the petroclinoid ligament. The infection can spread further giving rise to further complications like meningitis, intracranial abscess, spread to skull base and involvement of IX, X, XI cranial nerves (Vernet's syndrome), prevertebral/parapharyngeal abscess or spread to sympathetic plexus around carotid sheath [2].
We present a case report of unusual presentation and eitiological cause of Gradenigo's syndrome and its effective management.
A 57-year-old male presented with diplopia on left lateral gaze (Figure 1) along with left sided hemicranial headache and reduced sensation on left half of face, since 1 month. There was past history of left ear infection 1 year back which resolved with medications. On ENT examination bilateral tympanic membrane was intact. There was no mastoid tenderness, tunning fork tests: Rinnes was positive on both sides and Weber was centralized. There was restriction of movement of the left eye laterally which was suggestive of left abducens nerve palsy. Rest ENT examination was also normal. Rest of cranial nerve examination was normal. On ophthalmic assessment vision was good and fundoscopy was normal. HRCT Temporal bone was suggestive of complete erosion of left mastoid aircells suggestive of left otomastoiditis, with erosion of dural and sinus plate with extradural intracranial extension (Figure 2). MRI Brain, MR Venogram and MRI orbit were normal. Pure tone audiometry was suggestive of mild conductive hearing loss on the left side while right was normal.
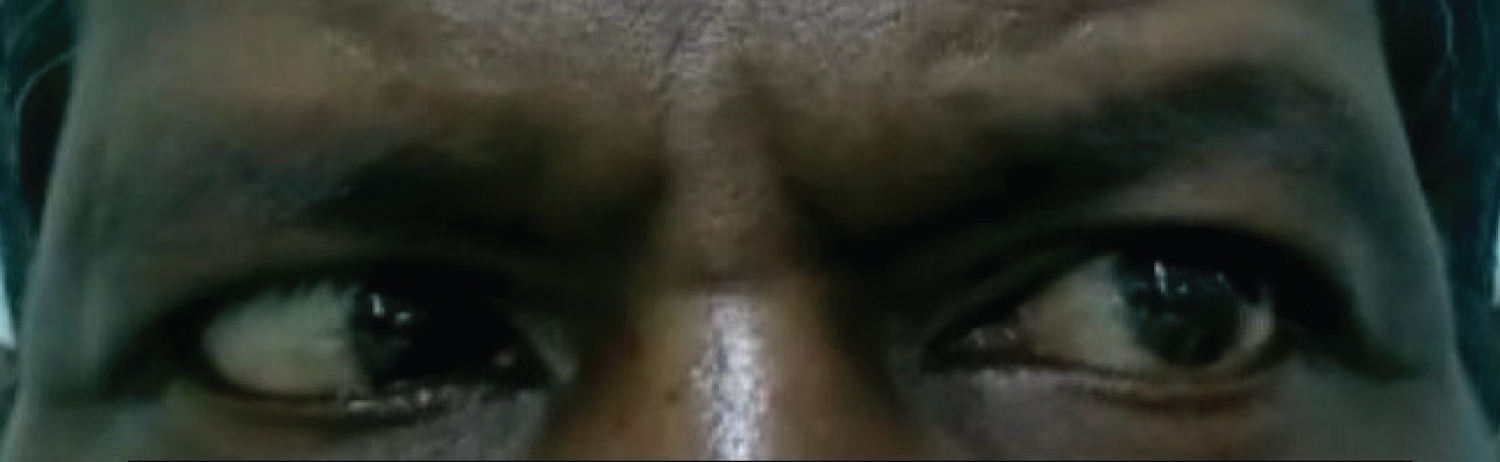 Figure 1: Pretreatment photo showing left lateral rectus palsy.
View Figure 1
Figure 1: Pretreatment photo showing left lateral rectus palsy.
View Figure 1
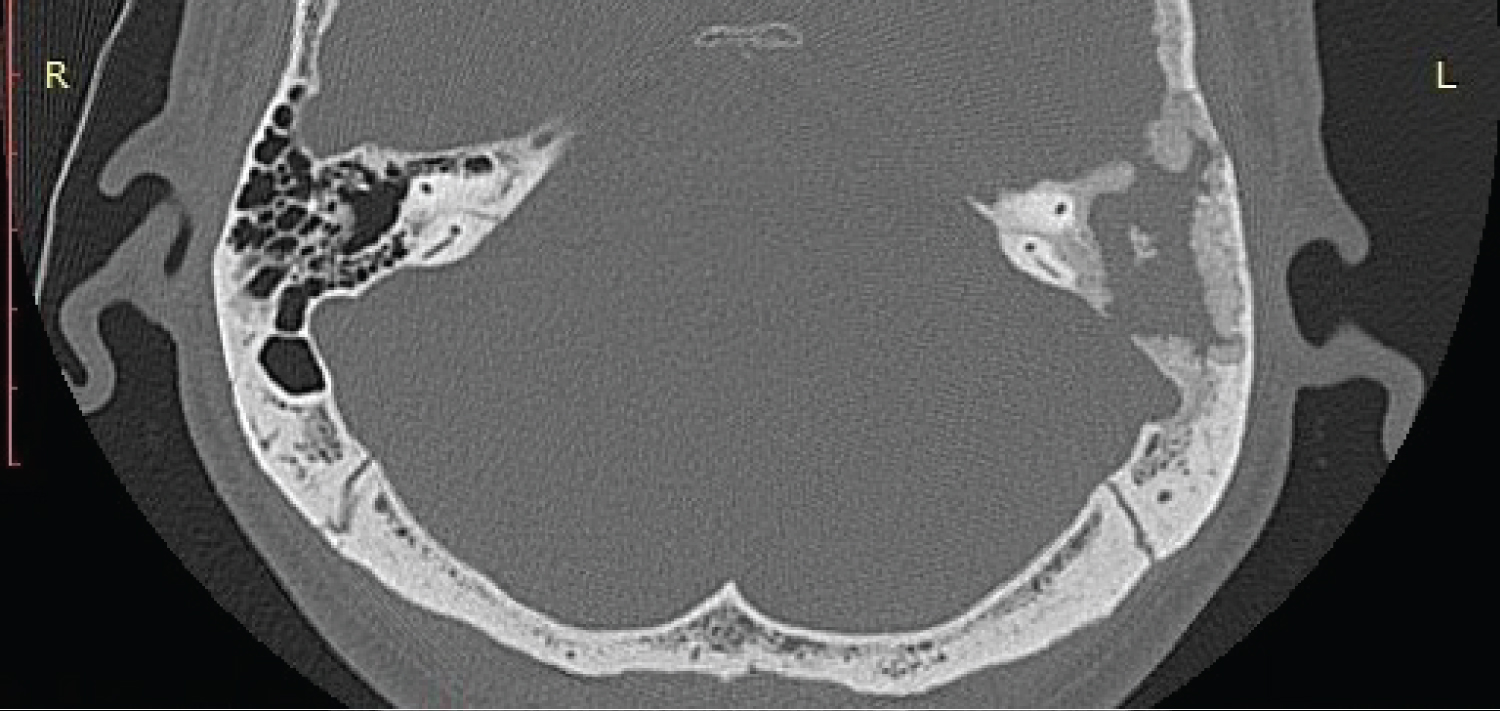 Figure 2: HRCT temporal bone showing complete haziness of left mastoid air cells with destruction of sinus and dural plate and extension upto petrous apex.
View Figure 2
Figure 2: HRCT temporal bone showing complete haziness of left mastoid air cells with destruction of sinus and dural plate and extension upto petrous apex.
View Figure 2
Clinically it was diagnosed as Gradenigo's syndrome and patient was worked up for left mastoidectomy. All blood investigations including ESR were normal. Empirically tablet ciprofloxacin was started for the patient as tuberculous otitis media is one of the differential for Gradenigo's syndrome. Patient partly responded to ciprofloxacin and there was partial improvement in left abducens palsy. Patient was taken up for surgery and on cortical mastoidectomy pale, dense, avascular granulations were present in the mastoid and middle ear cleft along with partial destruction of the posterior superior wall of external auditory canal with intact tympanic membrane (Figure 3). The granulations were cleared and sent for histopathology and Genexpert. The defect in the external auditory canal wall was closed with a cartilage. Histopathology was suggestive of chronic inflammatory granulations and Genexpert was negative for tuberculosis. Since clinically pale, avascular granulations are a feature of tuberculosis and patient had responded to Tab. Ciprofloxacin, empirical treatment with ciprofloxacin was continued for 3 weeks after which the lateral rectus palsy completely recovered (Figure 4).
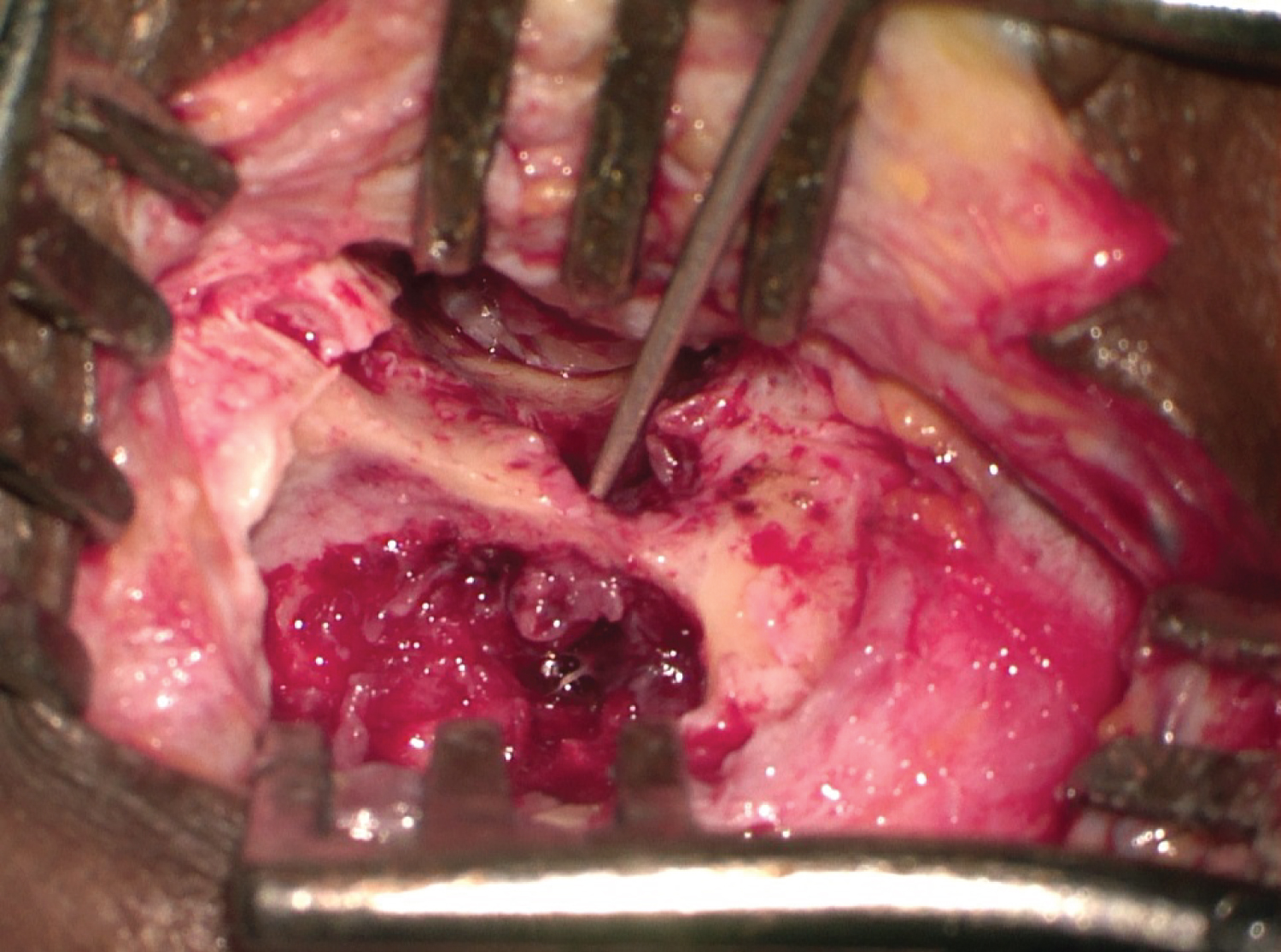 Figure 3: Intraoperative picture of left mastoid showing a ball point passing through the defect in posterior superior bony wall of external auditory canal and dense pale granulations in the mastoid.
View Figure 3
Figure 3: Intraoperative picture of left mastoid showing a ball point passing through the defect in posterior superior bony wall of external auditory canal and dense pale granulations in the mastoid.
View Figure 3
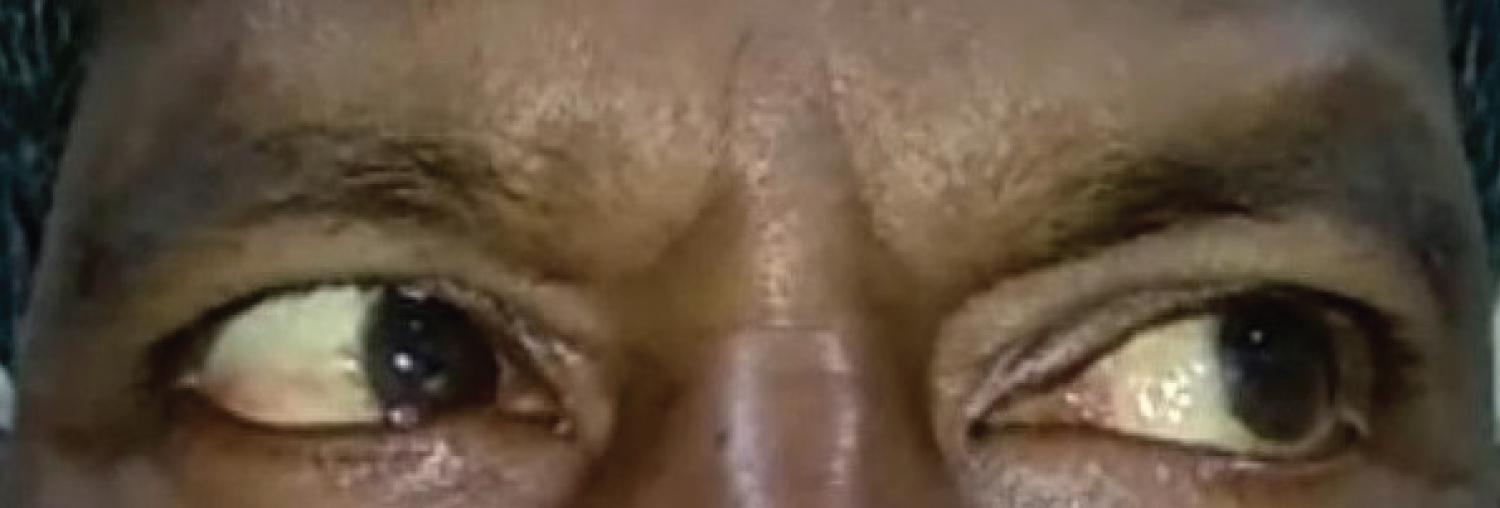 Figure 4: Post-treatment photo showing complete recovery in left lateral rectus palsy.
View Figure 4
Figure 4: Post-treatment photo showing complete recovery in left lateral rectus palsy.
View Figure 4
This case highlights some important points:
First, clinical features in Gradenigo Syndrome are variable. In Gradenigo's original series of 57 patients, less than 50% presented with the complete triad. In other case series, involvements of the seventh and eighth cranial nerves were described [3]. The pneumatisation of the mastoid cells of the temporal bone is universal world over but it varies at the petrous apex. Only one third of adult population show petrous apex pneumatisation. In such cases it can provide a pathway for AOM to spread medially causing apical petrositis [4]. In addition, this can also result by direct extension of the infection through bony destruction or hematologically through venous channels. This can cause true osteomyelitis in the non-pneumatized areas of the petrous bone [5]. Due to the central location of the petrous apex, apical petrositis may rapidly develop into severe and life threatening complications.
Second, literature review shows that it is most commonly caused by aerobic bacteria, but anaerobic bacteria may also be found and that it why both aerobic and anaerobic coverage should be considered when determining the antibiotic treatment [6].
Thirdly, there are various etiology for Gradenigo's syndrome, most common being apical petrositis secondary to suppurative otitis media and extradural inflammation at petrous apex involving: Trigeminal ganglion and abducens nerve [2]. There are reported cases of petrositis caused by cholesteatomas and chronic osteomyelitis of the petrous bone [3]. Some tumors like nasopharyngeal carcinoma have shown similar presentation like Gradenigo syndrome [7]. In 1989 Norwood and Haller reported a lymphoma mimicking Gradenigo's syndrome which is a rare condition [8]. Primary tuberculosis of petrous apex is rare entity and petrositis complication of tuberculous otitis media is even more rarer, and there are very few such cases reported in the medical literature. Also, very few of these patients present with lateral rectus palsy [9]. Infectious petrositis can have afebrile clinical presentation without otological complaints which can delay antibiotic treatment as can be misdiagnosed as a tumor [10]. Similar scenerio was seen in our case where patient had only involvement of trigeminal and abducens nerve without any otorrhoea or signs and symptoms suggestive of tuberculosis. Tuberculosis being endemic in our country, empirical antibiotic treatment with tablet ciprofloxacin was started for this patient to which the patient responded. Intraoperative findings were also in favor of tuberculosis, hence tablet ciprofloxacin was continued in the postoperative period for 3 weeks to which patient responded completely. It was stopped only after the Genexpert and histopathology report came negative for tuberculosis.
Gradenigo's syndrome is a rare and life-threatening complication. It is seen that the full triad of symptoms may not always be present. The etiological cause for it must be found by proper imaging and accordingly it must be effectively treated with long duration antibiotic coverage. Tuberculosis petrositis has similar presentation and it can be effectively managed with medical line of management avoiding major surgery. Surgery is only required for histopathology for establishing the diagnosis and in resistant and extensive cases where disease clearance is needed.
None.
None.
None.
None.
Written and Informed consent was taken from the patient for the surgery and for using the clinical photographs.