We present a series of three clinical videos of retrograde air flow through the lacrimal system with Valsalva maneuver that illustrate the hypothesized dysfunctions at various points within the lacrimal valvular system.
Under normal physiologic conditions, the lacrimal excretory system has a series of valves that prevent retrograde flow of fluid and air. Therefore, while performing the Valsalva maneuver, increased intranasal pressure is not transmitted to the nasolacrimal system; however, trauma, lacrimal surgery, and positive airway pressure can disrupt the normal valve system and allow air to enter the lacrimal system.
A 35-year-old patient presented with complaint of tear duct expansion. Additionally, a 42-year-old patient and his son, a 9-year-old patient, presented with sensation of air near the ocular region upon performing Valsalva maneuver.
There was air regurgitation from the lacrimal excretory system in the absence of known predisposing factors. These possibly represent variations in the lacrimal valvular system with characteristic physical exam findings that can best be appreciated through videos.
A small population of patients without predisposing factors may have retrograde air regurgitation due to unknown etiologies.
Valsalva, Nasolacrimal, Lacrimal valve, Regurgitation
NLD: Nasolacrimal Duct; DCR: Dacryocystorhinostomy
The following information was collected and evaluated after obtaining informed consent from the patients in order to comply to HIPAA. The report also adheres to guidelines as outlined by the Declaration of Helsinki.
A 35-year-old man presented with a complaint of "tear duct expands". He denied tearing, infection, or trauma. On examination, when he compressed his nostrils externally and induced a Valsalva maneuver, there was expansion of the lacrimal sac with deflation of the sac upon release of Valsalva (Figure 1A and Video 1). His tear lakes were normal and irrigation of the lacrimal system was normal with no stenosis or regurgitation bilaterally. CT scan revealed that the right lacrimal sac was distended by air (Figure 1B). There was no evidence of disease or fracture. We hypothesize dysfunctional valve of Hasner allowing pneumatocele formation via retrograde airflow with increased nasal airway pressure. The patient was otherwise asymptomatic, and the decision was made to not intervene surgically.
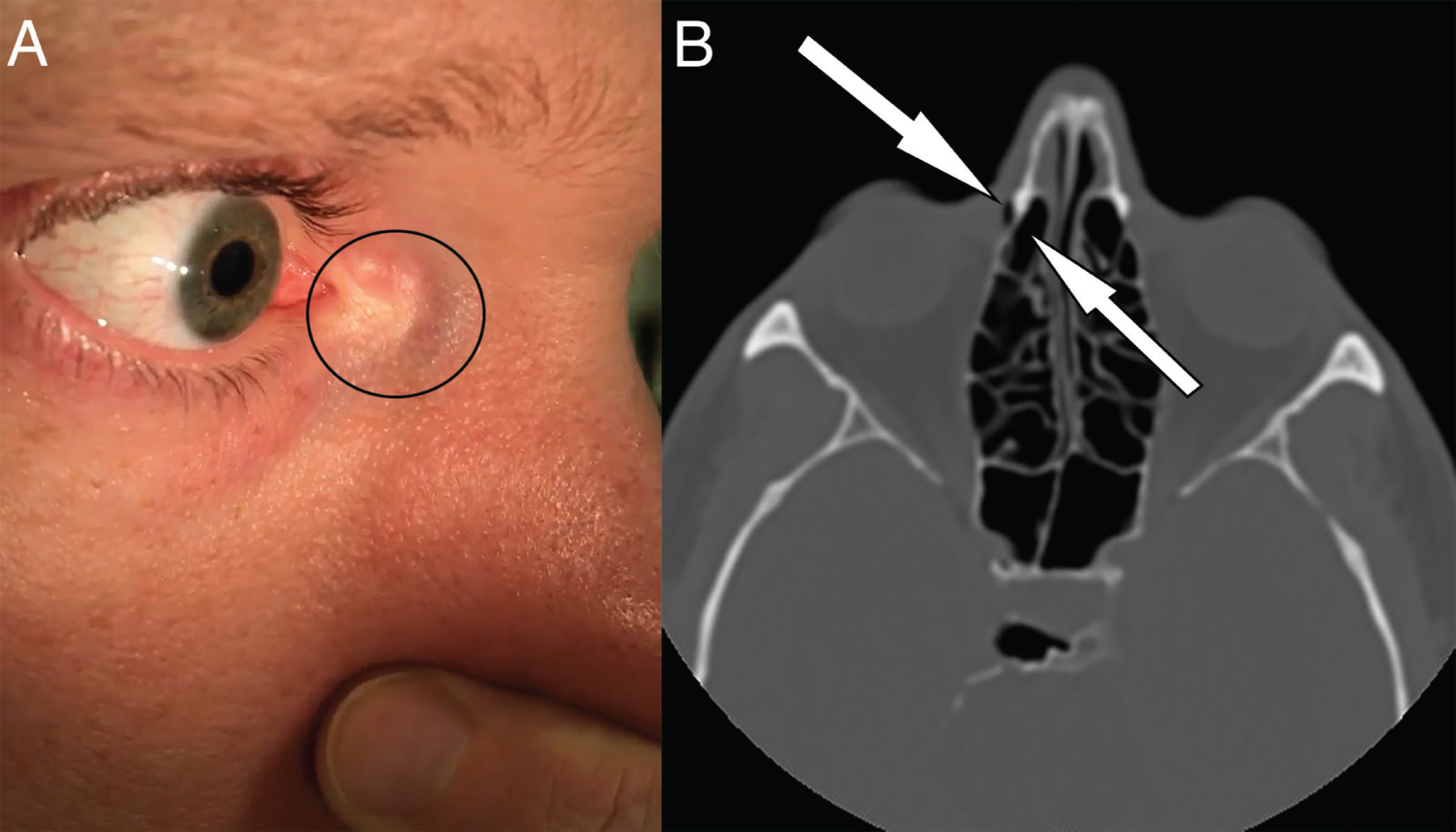 Figure 1: (A) The right lacrimal sac expands with Valsalva maneuver as the intranasal pressure is transmitted to the sac; (B) CT scan confirms pneumatocele in the right lacrimal sac.
View Figure 1
Figure 1: (A) The right lacrimal sac expands with Valsalva maneuver as the intranasal pressure is transmitted to the sac; (B) CT scan confirms pneumatocele in the right lacrimal sac.
View Figure 1
Video 1: Valsalva Maneuver. View Video 1
A 42-year-old man and his 9-year-old son both presented with a sensation of air on the ocular surface with forced expiration while closing the nose. Upon examination of both patients, a Valsalva maneuver resulted in air and a small amount of tears exiting the puncta, creating a high-pitched sound. These sounds were likely produced by turbulent airflow in a small diameter canal at high pressure. Both the patients had no tearing symptoms with normal tear lakes as well as normal irrigation testing. We hypothesize compromised valve function along the entire lacrimal excretory system, beginning with valve of Hasner, but also including the valves within the duct, the valve of Rosenmuller, and the punctal valves. Both patients were asymptomatic under physiologic conditions, and observation was recommended.
A number of named lacrimal valves have been described in detail, including the valves of Hasner at the inferior tip of the NLD, Taillefer within the NLD, Krause near the sac-duct junction, Rosenmuller at the sac-common canaliculus junction, as well as the valves of Bochdalek and Foltz at the superior and inferior puncta, respectively. Under normal physiologic conditions, these one-way valves function to prevent retrograde airflow from the nasal cavity into the lacrimal sac.
In patients who have undergone successful external or endoscopic DCR, negative pressure is detected with forced blinking and positive pressure during Valsalva maneuver [1]. Clinically, it is not uncommon for these patients to describe a sensation of air exiting their puncta with maneuvers that increase intranasal pressure such as blowing their nose. However, this is rarely clinically significant, because in most patients, the remaining valves are competent, the sac is widely opened (preventing pressure build up), and the pressure generated in a wide cavity such as the intranasal space, may be different than that in a smaller space, such as the lacrimal sac. Other causes of pneumatocele include trauma as illustrated by a recent case in which blunt nasal trauma resulted in fracture of medial wall of the NLD and sac-NLD junction, in which Valsalva-augmented CT-dacryocystography revealed a hypodense filling defect within a distended sac [2]. Other causes of lacrimal pneumatocele include congenital mucocele, persistent positive airway pressure, sleep apnea, and punctal plug insertion [3-6].
The prevalence of Valsalva-induced air regurgitation in patients with no predisposing factors is unknown, though many clinicians may have anecdotal experience with such patients. Our cases illustrate variations in clinical presentation that match presumed variations in valvular dysfunction. In addition to routine lacrimal evaluation by clinical exam and irrigation, CT scan or dacryocystography can be useful. While most patients can be simply monitored, DCR is an option for those patients who are symptomatic.
No financial support was received. No conflict relationship exists for any author. No assistance was received from medical writing experts.
All authors have contributed to this manuscript.