To determine the efficacy and incidence of complications in tumors and in other diseases involving the tongue base treated by transoral surgery with the assistance of endoscopes.
Patients treated for pathologies that compromised the tongue base using a transoral approach with the assistance of endoscopes in the head and neck section of the Otorhinolaryngology service of the Hospital Italiano de Buenos Aires between March 2005 and April 2019 were selected.
Central glossectomies and hemiglosectomies were performed with this technique, and through a ventral approach to the tongue, epidermal cysts that compromised the entire extension of the tongue were removed.
Three malignant tumors, one lingual thyroid, two epidermal cysts and a central resection of the tongue in a Down patient with severe sleep apnea were performed.
In malignant tumors the resections were complete with free margins, and in the others the region could be exposed very well and the pathologies resolved.
The use of endoscopes to perform transoral resections of tumors and other pathologies that compromised the tongue base allowed a good exposure of the posterior region of the tongue to the lingual aspect of the epiglottis and made it possible to perform complete resections or perform surgery according to preoperative planning without complications.
Tongue base, Transoral surgery, Endoscopes
The use of endocameras and endoscopes to see with magnification and angle is common in otorhinolaryngological surgeries.
Better vision facilitates exposure and proper surgical treatment.
The use of endoscopes in surgeries of the tongue base allows exposing this sector and visualizing posteriorly and inferiorly up to the lingual aspect of the epiglottis and valleculae, making it possible to perform complete resections even in malignant tumors.
Surgeries performed transorally with the assistance of endoscopes reduce morbidity by avoiding tracheostomies and the indication of prolonged enteral feeding, as occurs in external surgical approaches, and decreases hospitalization time and cost of the procedure.
To determine the efficacy and incidence of complications in tumors and in other diseases involving the base of the tongue treated by transoral surgery with the assistance of endoscopes.
Descriptive and retrospective.
Patients treated for pathologies involving the tongue base using a transoral approach with the assistance of endoscopes in the head and neck section of the Otorhinolaryngology department of the Hospital Italiano in Buenos Aires between March 2011 and April 2019 were selected.
Those who had superficial lesions at the base of the tongue such as vallecula cysts, tonsils lingual hypertrophy and other pathologies that involved the lingual mucosa without affecting the deep muscular plane were excluded.
The surgeries were performed under general anesthesia with orotracheal intubation.
4 mm, 0° and 30° endoscopes similar to those used in rhinosinusal endoscopic surgery, and the Storz tower with a full HD endocamera were used in all cases.
Jennings-type mouth gag was used, and the tissue was cut and coagulated with a cautery or ultrasonic scalpel.
The surgical technique consisted of placing a transfixing point in the anterior sector of the oral tongue to better pull and expose the tongue base.
In hemiglosectomies of the tongue base for malignant tumors, a horizontal incision was first made anterior to the tumor (= or > 5 mm) from the midline to the side and in depth, checking by endoscopic vision and palpation that there was no submucosal extension that compromised the margin.
Next, another incision was made perpendicular to the previous one at the level of the midline or a few millimeters on the contralateral side depending on the extension of the neoplasm, up to the vallecula. With a forceps the surgical specimen was tractioned and the deep muscles were sectioned from medial to lateral, at the vallecular level, maintaining a minimum tumor-free margin of 5 millimeters. Upon finding the lingual artery, it was ligated.
The resection was done in bloc and the specimen was oriented for the intraoperative histopathological study of the margins (Figure 1).
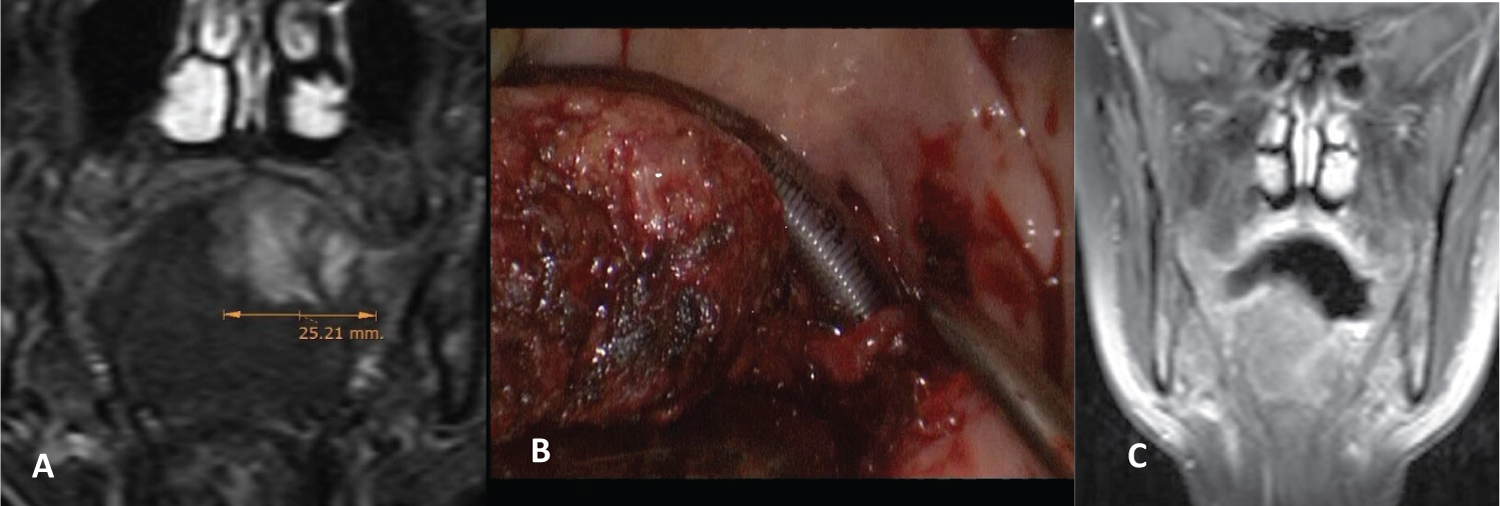 Figure 1: Adenoidecystic carcinoma. A) Preoperative magnetic resonance (MR); B) Tongue base hemiglosectomy; C) Posoperative MR.
View Figure 1
Figure 1: Adenoidecystic carcinoma. A) Preoperative magnetic resonance (MR); B) Tongue base hemiglosectomy; C) Posoperative MR.
View Figure 1
Table 1: Endoscopic transoral approaches to tongue base (RT/QT: Concurrent radio chemotherapy). View Table 1
In another, the same surgical technique was used but an oral and tongue base hemiglossectomy was performed due to the extension of the tumor.
Central glossectomies were performed, which included the resection of the middle sector of the oral and tongue base, preserving both lingual arteries.
In one patient, a Doppler ultrasound was used to locate and mark the lingual arteries in the oral sector of the tongue.
The area after the resection at the tongue base was left to heal by second intention (Figure 2 and Figure 3).
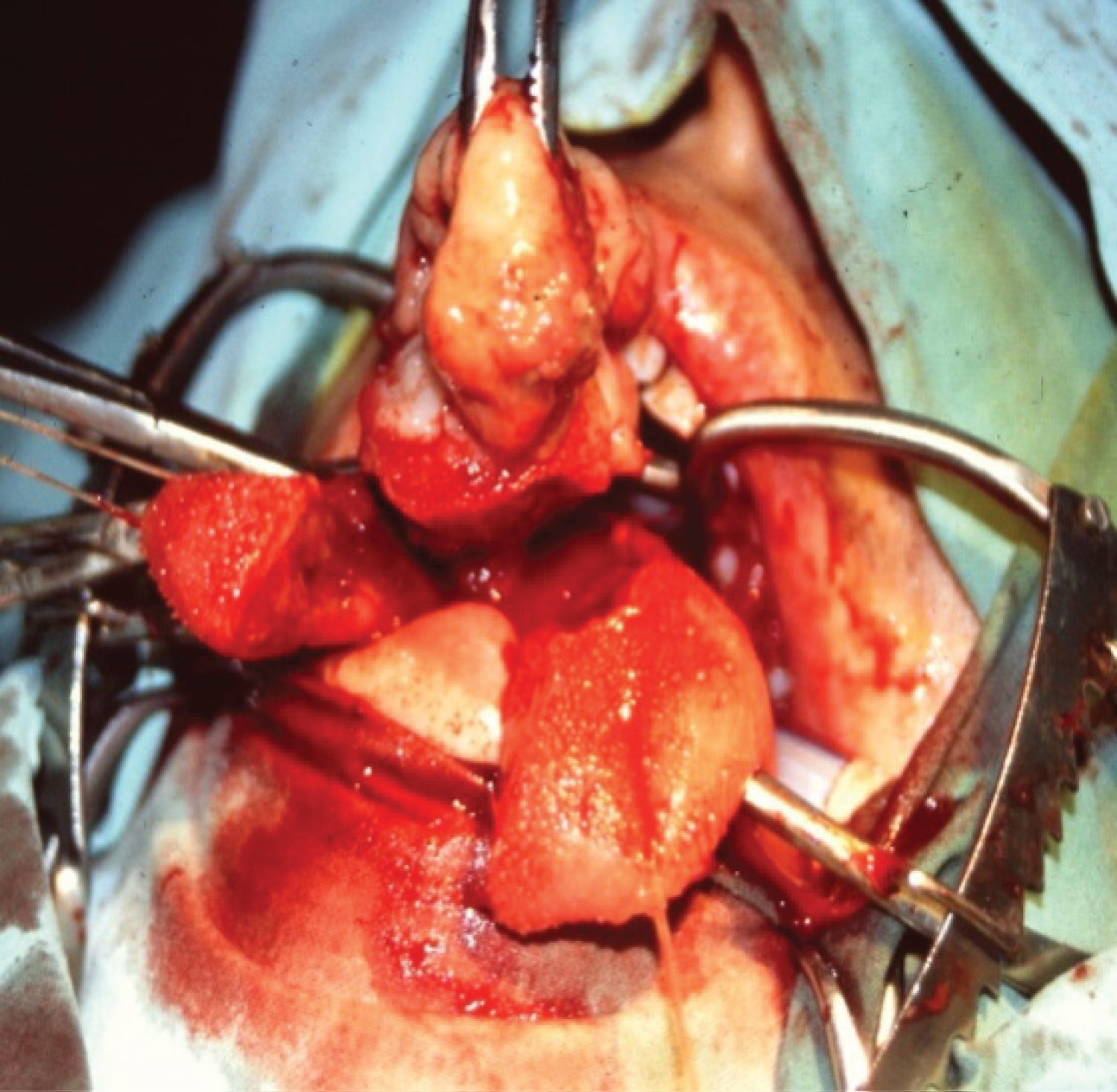 Figure 2: Oral and tongue base leiomyosarcoma: central glossectomy.
View Figure 2
Figure 2: Oral and tongue base leiomyosarcoma: central glossectomy.
View Figure 2
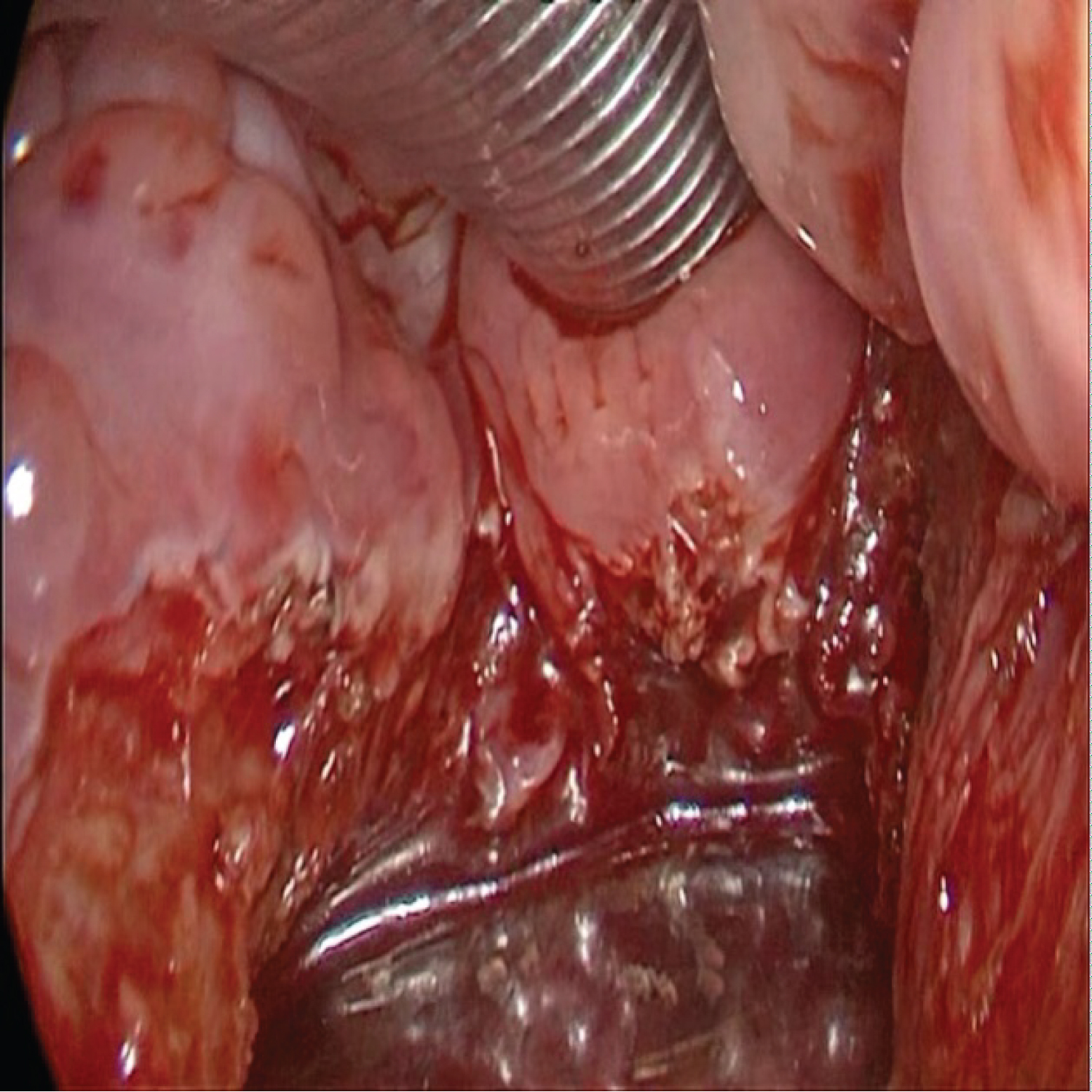 Figure 3: Central glossectomy of oral and tongue base due sleep apnea in a patient with Down syndrome (macroglossia).
View Figure 3
Figure 3: Central glossectomy of oral and tongue base due sleep apnea in a patient with Down syndrome (macroglossia).
View Figure 3
In one case of an ectopic thyroid at the tongue base, the lesion was resected with the same technique described preserving the deep muscles (Figure 4).
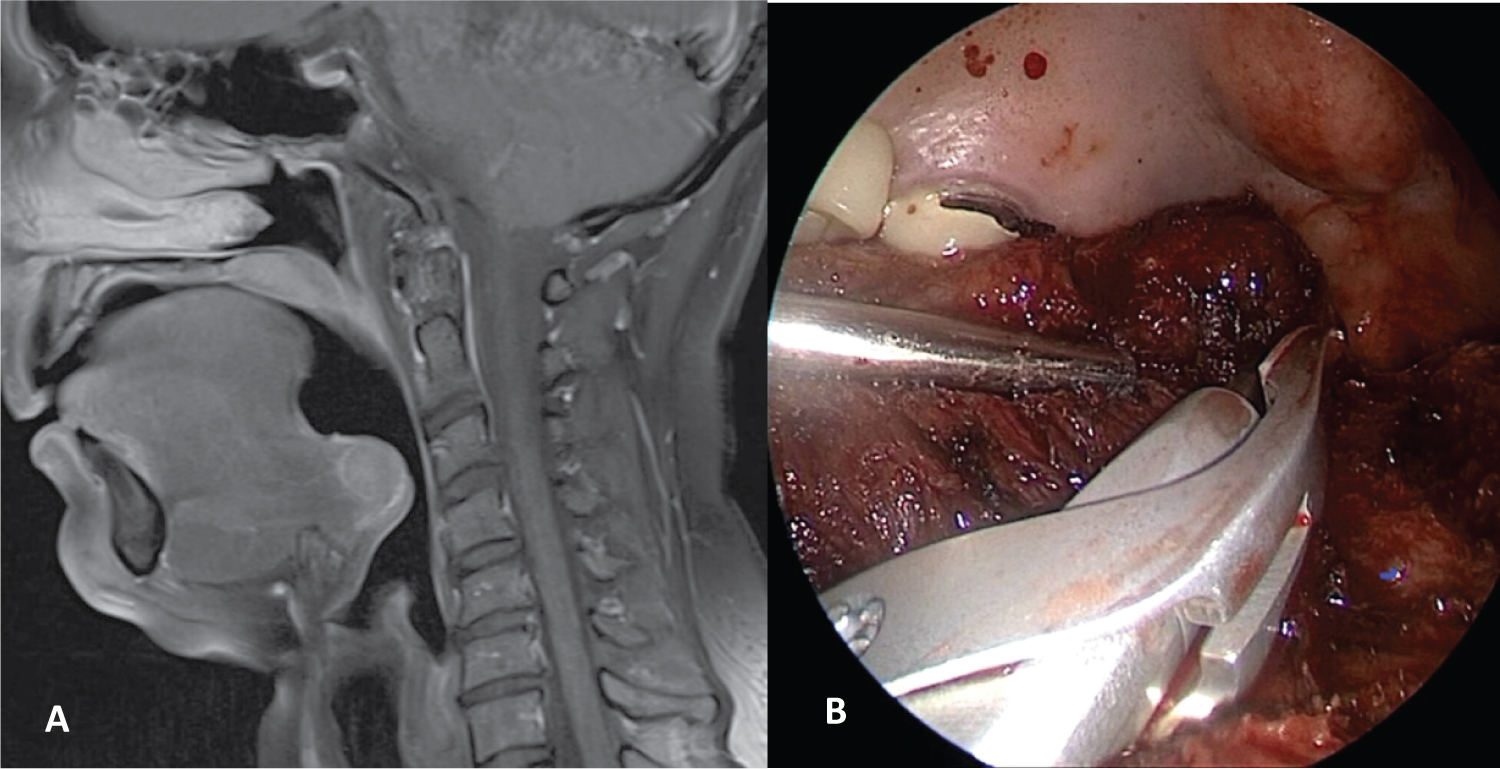 Figure 4: Lingual ectopic thyroid: A) MR; B) Transoral endoscopic resection.
View Figure 4
Figure 4: Lingual ectopic thyroid: A) MR; B) Transoral endoscopic resection.
View Figure 4
In other cases, an incision was made in the mucosa of the ventral sector of the tongue, 1cm above the Wharton's ducts holes and in an extracapsular plane they were dissected and excised two giant epidermal cysts that compromised the tongue base (Figure 5).
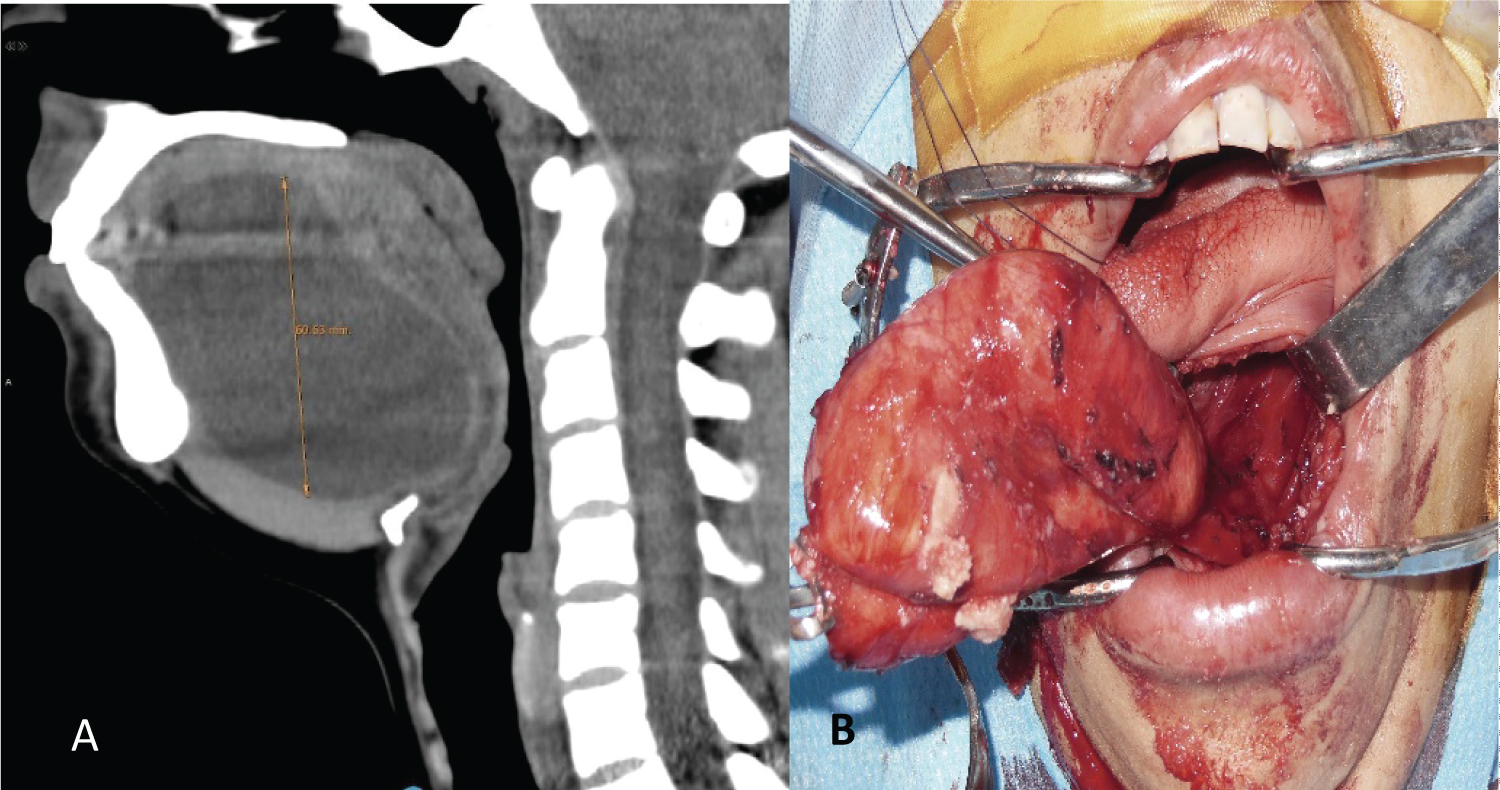 Figure 5: Tongue base epidermal cyst: A) MR; B) Endoscopic ventral approach.
View Figure 5
Figure 5: Tongue base epidermal cyst: A) MR; B) Endoscopic ventral approach.
View Figure 5
The patients were hospitalized for the first 24 hours in an intermediate therapy unit. In some, a functional study of swallowing was performed 24 hours after surgery. Surgery was considered effective when the pathologies treated could be exposed without inconvenience and the resections were adequate and complete (tumors) or resolved the disease.
Seven patients were treated by a transoral approach with endoscopes for pathologies that compromised the base of the tongue from March 2004 and April 2019 in the Otorhinolaryngology department of the Hospital Italiano de Buenos Aires.
All were women; the average age was 49.28 years.
Three had malignant tumors: Adenoidecystic carcinoma, squamous cell carcinoma, and leiomyosarcoma (they had prior treatment with chemo/radiotherapy at another center).
Another patient had an ectopic lingual thyroid, and another a macroglossia (Down syndrome) causing severe sleep apnea.
Two patients had epidermal cysts that involved the entire length of the tongue. Two patients underwent an oral and tongue base medial glossectomy (leiomyosarcoma and macroglossia). In another, an oral and base hemiglosectomy (staged T3N0 squamous cell carcinoma) witha selective bilateral neck dissection (level II, III, and IV) and in another a base hemiglossectomy (adenoidecystic carcinoma) were performed.
In the patient with a lingual ectopic thyroid, the lesion in the central region of the tongue base was resected. She had a history of previous surgery at another hospital where they were unable to expose and resect the lesion using a transoral microsurgical technique.
In patients with epidermal cysts, the lesion was excised through a ventral incision above the mouth of the Wharton's ducts, preserving the deep muscles of the tongue.
A functional swallowing study was performed in 3 patients 24 hours after surgery. None had aspiration and were able to feed orally.
The patient who had squamous cell carcinoma who underwent an oral and base hemiglosectomy was able to eat well after surgery. He underwent adjuvant treatment with postoperative chemo/radiotherapy and had aspiration for which he was fed by nasogastric tube and then by gastrostomy.
The average hospital stay was 2.28 days.
There was no need for tracheostomies and no patient had postoperative bleeding or other complications.
Surgical exposure was very good in all cases, allowing surgery to be performed according to preoperative planning and resections in cases of tumors and pseudotumors were complete.
The tongue base is the posterior region located behind the V lingual.
It has a vertical orientation and is a hidden area, not directly visible through the mouth and difficult to expose transorally.
Various surgical approaches can be used to expose and resect the deep muscular plane of the tongue base.
Externally, it can be accessed through a lateral, supra, trans, or infrahyoid pharyngotomy, or with a transmandibular approach, with a median glossotomy, or with a lateral incision to the tongue on the floor of the mouth.
All of these surgeries produce scars, require a tracheostomy, and a temporary nasogastric tube feeding.
The transoral approach using conventional or bivalve laryngoscopes with microscope allow to expose the tongue, but vision is reduced (through the diameter of the laryngoscope), and in some patients it may be difficult to achieve adequate exposure.
In a retrospective study conducted at the Mayo Clinic, they reported nine patients with lingual thyroid treated with surgery between 1994 and 2012.
In 4 they performed a transoral approach with a microscope and CO2 laser, in 3 they performed a TORS, in one a transoral approach without a microscope and in another they used an open technique using a modified Sistrunk procedure.
In seven they were able to perform a total lingual thyroidectomy and in two a partial one. Incomplete resection was attributed to difficult exposure [1].
In our study, the patient with a lingual ectopic thyroid had a history of surgery in another hospital, without being able to perform surgery due to inadequate exposure of the lesion through laryngoscopes.
Robotic transoral surgery (TORS) allows a good exposure of the region, magnified and angled vision, but the cost of the equipment and the procedure may be a limitation for its indication in some centers.
The transoral techniques used were diverse and were due to the different extension, location and type of pathology treated.
In middle glossectomies it is important to consider the location of the lingual arteries.
The lingual artery originates from the external carotid and runs lateral to the greater horn of the hyoid, and lateral to the median constrictor muscle of the pharynx. It curves between the greater horn and the styloglossus muscle, and then crosses lateral and inferior to it, originating the dorsal and deep lingual artery.
To avoid injury, the transoral surgeon must maintain the dissection medial to the stylohyoid ligament and the styloglossus muscle [2,3].
In the oral sector of the tongue, the arteries lie 1 cm from the midline and behind the V lingual they diverge away from the midline. This allows for larger resections in this area.
In studies carried out in cadavers, they described the location of the neurovascular bundle, 2.7 cm inferior and 1.6 cm lateral to the foramen cecum, 0.9 cm superior to the hyoid bone, and 2.2 cm to the mandible [4-6].
In another study, they determined the position of the lingual arteries using CT angiography with the tongue at rest and extended.
The depth of the arteries at the level of the foramen cecum was 27.9 mm + -3.2 mm, and 24 mm + -2.7 mm in the extended position.
They concluded that it is safer to consider the position of the artery with the tongue extended since when performing the transoral glossectomy, the mouth is open and the tongue is fully extended [7].
Another way to repair the course of the lingual arteries is using a dopler ultrasound, marking the course of the arteries previously on the tongue [8].
In hemiglosectomies of the tongue base, the lingual artery can be coagulated, ligated or clipped transorally, preserving the contralateral artery. We prefer to tie the artery.
In these cases the contralateral artery due to its abundant network of anastomoses, provides sufficient irrigation to maintain vital the remaining sector of the resected tongue [9,10].
Deep tongue resections were performed with electrocautery in five patients and the harmonic scalpel was used in one.
Due to the possibility of this latest equipment to coagulate vessels of up to 5 mm and to produce less damage and edema in the tissues due to the lower temperature it produces, we believe that it may be the best equipment to perform resections in this region [11].
In two patients with giant epidermal cysts, we performed the excision through an incision of approximately 1.5 cm in the ventral surface of the tongue, above the mouth of the Wharton's ducts and with the assistance of endoscopes, we dissected and excised the cyst of the depth of the tongue.
We have not found descriptions of a similar technique in the literature.
The use of endoscopes to perform transoral resections of tumors and other pathologies that compromised the medial or lateral tongue base allowed a good exposure of the posterior region of the tongue to the lingual aspect of the epiglottis and made it possible to perform complete resections or perform surgery according to preoperative planning.
The exposure obtained from the tongue base is better than with transoral microsurgery.
There were no complications. We believe that this technique could be of choice to treat pathologies in selected patients which deep resections at the tongue base are required.
None of the authors declare conflicts of interest.