Objectives: Schwannomas of the nasal cavity and paranasal sinuses are uncommon. Treatment is surgical and endoscopic excision is a main indication. Our aim was to determine the incidence of rhinosinusal Schwannomas and the effectiveness of endonasal surgery with endoscopes to treat these tumors.
Methods: The electronic medical records of all patients diagnosed with head and neck schwannomas were reviewed, excluding acoustic nerve neurilemomas and neurofibromas. Those who presented tumors located in the nose or paranasal sinuses were selected. They were treated with surgery in the Rhinosinusology section of ENT Department of the Hospital Italiano de Buenos Aires between March 1998 and December 2019.
Results: Eighteen patients were selected who had histological (15/18) and clinical and imaging (3/18) diagnoses of neural type neoplasia, located in the head and neck.
Two neck neurofibromas were excluded.
Five patients with schwannomas located in the nasal cavity and paranasal sinuses were treated with surgery and had histopathological confirmation. The surgical technique varied according to the time of its indication.
In four patients, an endonasal approach with endoscopes alone or combined with a frontal craniotomy was performed and in another a sublabial approach was made.
The resection was complete in 4 patients and subtotal in another (intracranial extension with bilateral compromise of visual acuity).
Conclusions: The incidence of sinonasal schwannomas within the nerve tumors diagnosed in the head and neck was 31.25% (5/16).
Endoscopic excision was very safe and effective to treat the patients with sinonasal schwannomas.
Schwannoma, Nasal, Paranasal sinuses, Endoscopic surgery
Schwannomas or neurilemomas are usually benign tumors that originate from Schwann cells that are part of the peripheral nerve sheath.
They are rare tumors and represent 1% of head and neck tumors. Between 25 to 40% of schwannomas originate in the head and neck region, being more common their origin in the auditory nerve (80%), the rest of exocranial tumors are distributed among the different sectors of the neck and the cavity nasal and paranasal sinuses [1].
The treatment is surgical and there are different approaches described to perform the complete excision of the tumor.
Endoscopic excision is an appropriate technique due to its lower morbidity, the excellent vision and magnification of the surgical field produced by high-definition endocameras and the possibility of performing skull base reconstructions if necessary with dissected flaps of the nasal cavity.
To determine the incidence of nasosinusal schwannomas and the effectiveness of endoscopic surgery to treat these tumors.
The electronic medical records of all patients diagnosed with head and neck schwannomas were reviewed, excluding acoustic nerve neurilemomas and neurofibromas.
Those who presented tumors located in the nose or paranasal sinuses were selected. They were treated with surgery between March 1998 and December 2019.
All patients with nasosinusal schwannomas were diagnosed by histopathological study and immunostaining (S-100 protein).
All were evaluated by nasal endoscopy and computed tomography (CT), and four with magnetic resonance imaging (MRI) with contrast.
Endonasal preoperative biopsies were performed in patients with voluminous tumors predominantly located in the nasal cavity and with intracranial extension.
The surgical techniques used varied according to time, before the year 2000 the surgeries were performed using an external approach (Figure 1) or a combination of an external and endonasal approach (cranionasal with endoscopes in conjunction with the neurosurgeon) (Figure 2).
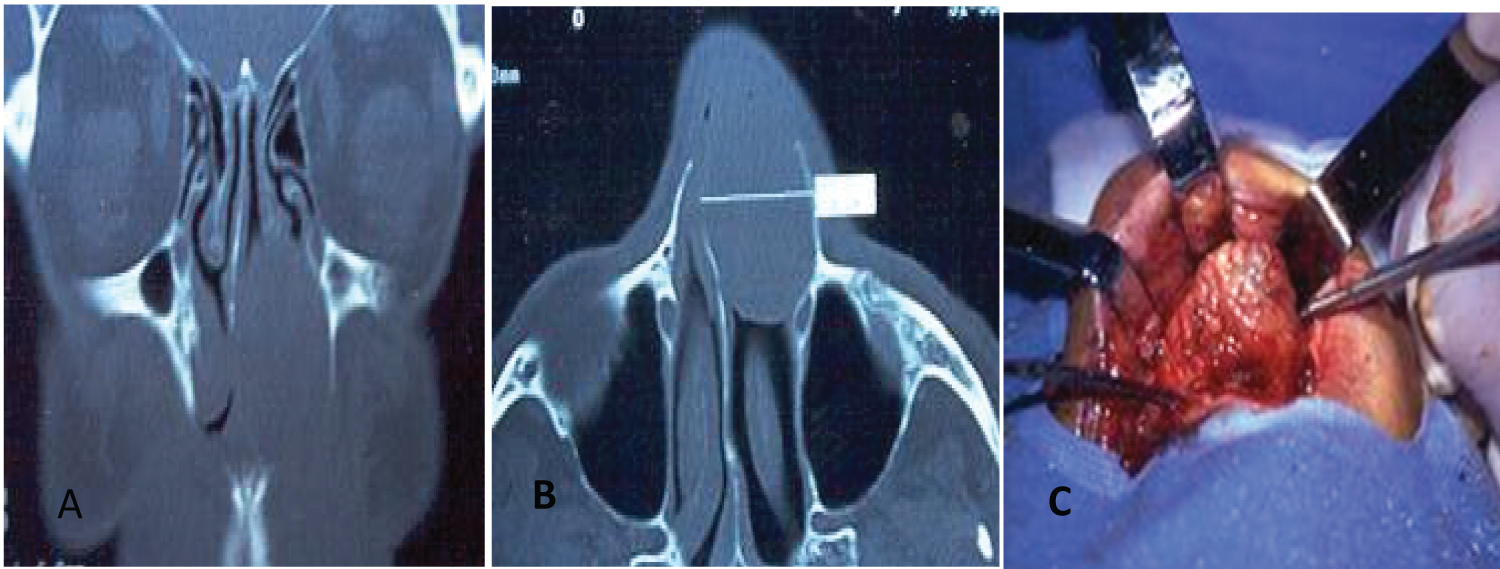 Figure1: Nasal cavity Schwannoma (A&B) Coronal and axial CT; (C) Sublabial approach.
View Figure 1
Figure1: Nasal cavity Schwannoma (A&B) Coronal and axial CT; (C) Sublabial approach.
View Figure 1
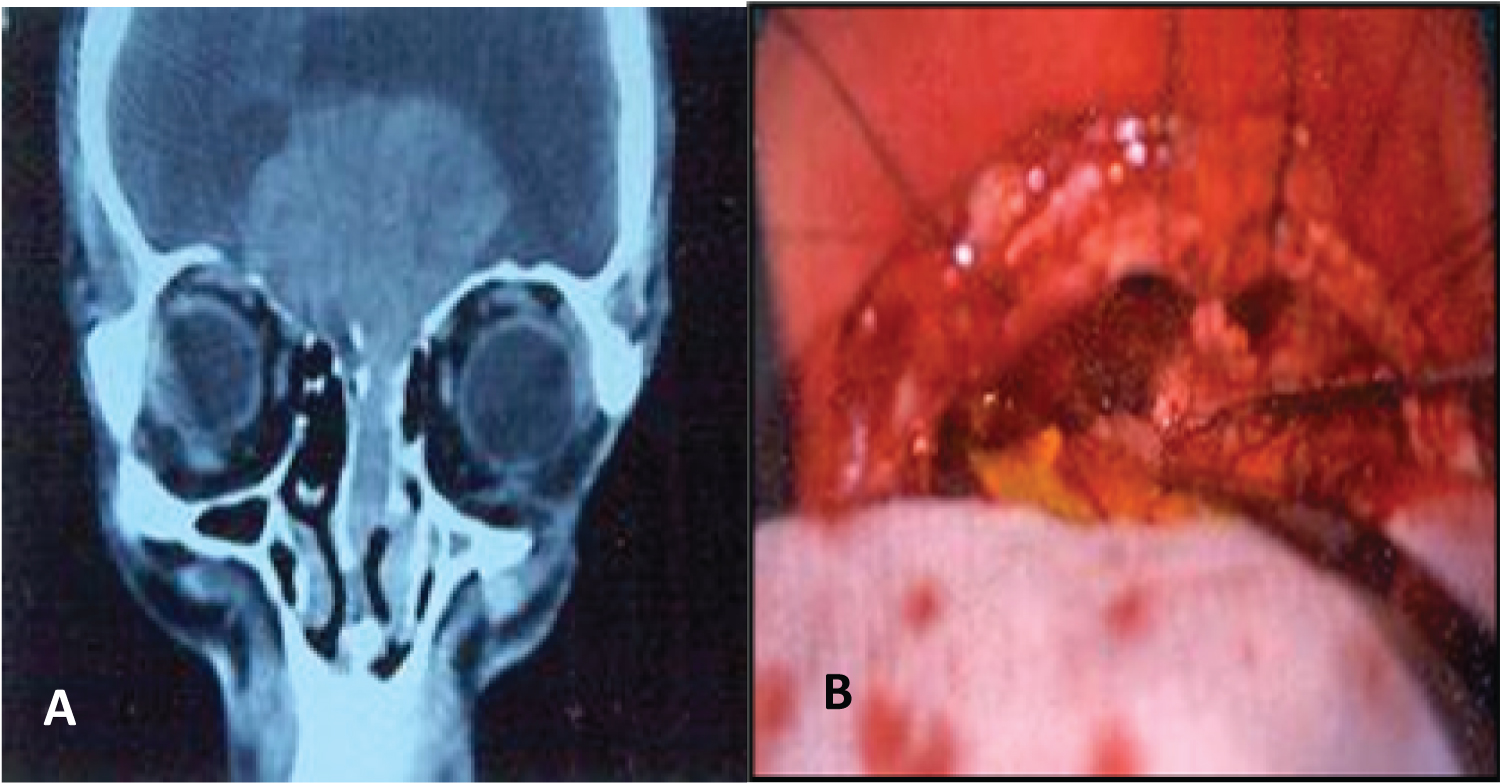 Figure 2: Schwannoma with endocranial involvement and bilateral decrease in visual acuity (A) Coronal CT; B) Endoscope-assisted cranionasal resection: View from the craniotomy.
View Figure 2
Figure 2: Schwannoma with endocranial involvement and bilateral decrease in visual acuity (A) Coronal CT; B) Endoscope-assisted cranionasal resection: View from the craniotomy.
View Figure 2
Reconstruction of the skull base was done with a pericranium flap.
After year 2000, the endonasal approach was used with 0° and 30° endoscopes. Tumors that were located in the nasal cavity and in the ethmoid were resected through this approach (Figure 3) and in another patient who had a schwannoma located in the maxillary sinus and pterygomaxillary fossa, a wide middle maxillary antrostomy with resection of the posterior wall of the maxillary sinus and an approach to the pterygomaxillary fossa was performed to resect the tumor (Figure 4).
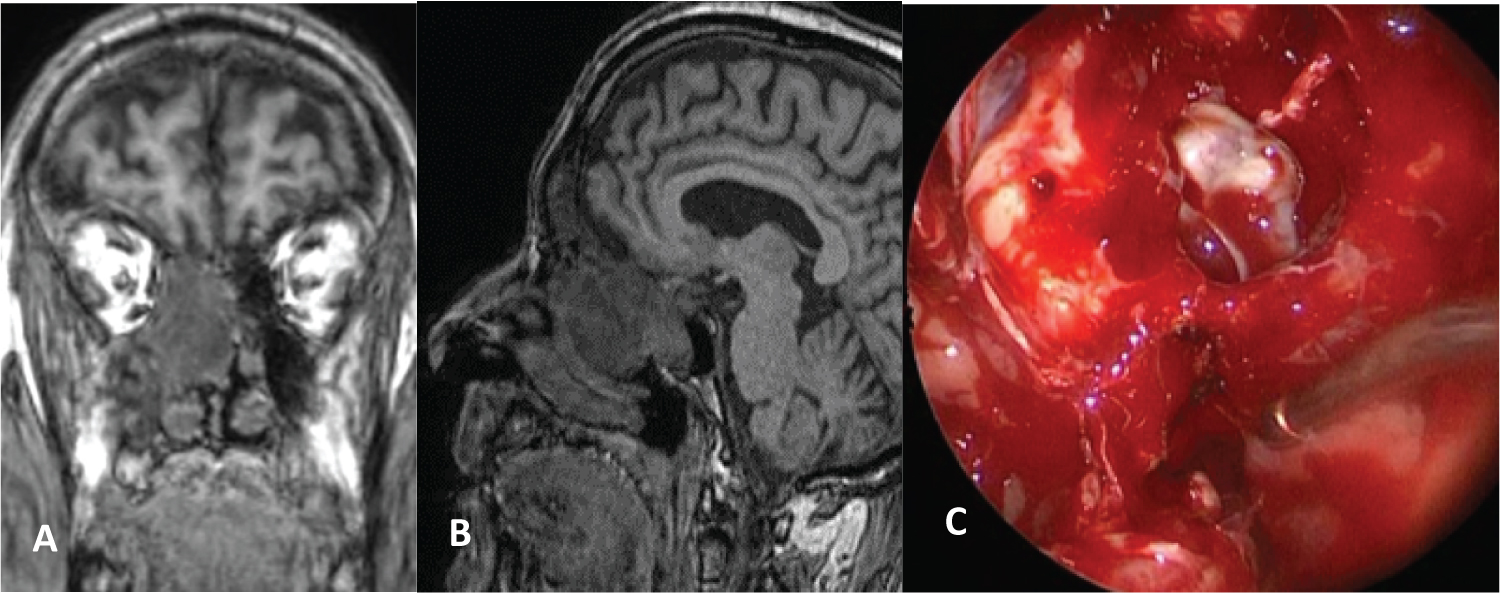 Figure 3: Ethmoidal Schwannoma. A) Coronal and sagittal MRI; B) Endoscopic resection; C) Maxillary antrostomy, anterior and posterior ethmoidectomy, sphenoidotomy and dissection of the tumor from the the skull base.
View Figure 3
Figure 3: Ethmoidal Schwannoma. A) Coronal and sagittal MRI; B) Endoscopic resection; C) Maxillary antrostomy, anterior and posterior ethmoidectomy, sphenoidotomy and dissection of the tumor from the the skull base.
View Figure 3
 Figure 4: Pterigomaxillary Scwhannoma. A) Axial CT; B) Endoscopic endonasal vision trough middle maxillary antrostomy, scalpel section and intracapsular dissection; C) Postoperative CT.
View Figure 4
Figure 4: Pterigomaxillary Scwhannoma. A) Axial CT; B) Endoscopic endonasal vision trough middle maxillary antrostomy, scalpel section and intracapsular dissection; C) Postoperative CT.
View Figure 4
The patient in whom the cranionasal approach was performed was admitted to the intensive care unit and another for his associated comorbidities in intermediate therapy. The others remained in the common room.
Controls were made with nasal endoscopy, computed tomography or magnetic resonance imaging for an average of 27 months.
Eighteen patients were selected who had histological (15/18) and clinical and imaging (3/18) diagnoses of neural type neoplasia, located in the head and neck. They were diagnosed in a period of 21 years.
Three elderly patients with a presumptive diagnosis of schwannoma were not operated (one had vocal cord paralysis and poor general condition, another did not want to undergo surgery, and the third had a small asymptomatic tumor located in the carotid space) and they had no histopathological confirmation of neurilemoma.
Two neck neurofibromas were excluded. Five patients with schwannomas located in the nasal cavity and paranasal sinuses were treated with surgery and had histopathological confirmation.
The incidence of nasosinusal schwannomas within the neurilemomas diagnosed in the head and neck was 31.25% (5/16).
Four were men and one woman, the average age was 58.2 years, the youngest was 29 and the oldest 79 years.
The possible site of origin was the ethmoid (2/5), maxillary sinus and pterygomaxillary fossa (1/5), inferior turbinate (1/5), and lateral wall of the nasal vestibule (1/5).
The symptoms were: Progressive unilateral nasal obstruction (2/5), unilateral nasal obstruction and hyposmia (1/5) unilateral nasal obstruction and bilateral decrease in visual acuity (1/5), facial pain in the infraorbital nerve territory (1/5).
All were evaluated by nasal endoscopy and computed tomography, and three also with magnetic resonance imaging.
In three patients, the presumptive diagnosis of neural tumor was established according to the location, endoscopic and especially imaging.
A previous biopsy was performed in three patients under general anesthesia. Surgical treatment was indicated in all. The surgical technique varied according to the time of its indication.
In four patients, an endonasal approach was performed with endoscopes alone or combined with a frontal craniotomy and in another trough a sublabial approach.
There were no complications during or after surgery.
The resection was complete in 4 patients and subtotal in another (endocranial extension with bilateral compromise of vision due to compromise of the chiasm and the proximal sector of the optic nerves).
In four patients during the mean follow-up time (2 years) no recurrences were detected. The patient with schwannoma who had intracranial extension improved vision and nasal obstruction, and residual tumor growth was not detected during the controls (Table 1).
Table 1: Schwannomas of nasal cavity and paranasal sinuses. View Table 1
Schwannomas are benign tumors that originate from Schwann cells, which constitute the sheath of peripheral nerves except the optic and olfactory nerves that do not have Schwann cells and are enveloped by the meninges.
They manifest as slow-growing solitary lesions and are not associated with genetic alterations. Other names by which they can be called are: neurilemoma and neurinoma, and they are included within spindle cell tumors.
They can originate in any part of the body, but are more frequent in the head and neck region (25-45%), their location in the nasal cavity and paranasal sinuses is rare (4%) [1-3].
In our study, nasosinusal neurilemmomas were more frequent than in other series (5/16: 31.25%).
Nasosinusal schwannomas probably originate from the ophthalmic or maxillary branches of the trigeminal nerve and also from the autonomic fibers of the carotid sympathetic plexus or the sphenopalatine ganglion [4] although most of the time it is very difficult to establish the nerve of origin.
Only in the patient with maxillary schwannoma could the origin of the tumor in the infraorbital nerve be identified on the MRI, due to the thickening of the nerve, and this was corroborated in surgery.
The ethmoid is the most common site of rhinosinusal location, followed by the maxillary sinus, the nasal cavity, and the sphenoid [5].
In a systematic review made in Pub-Med and Medline in 2014, they reported 94 cases of Schwannomas of the paranasal sinuses and anterior skull base [6].
Most schwannomas are benign, malignant tumors are exceptional, with 30 to 40 cases described in the literature [7]. In a review of 430,000 cases of non-epithelial tumors of the nasal cavity, paranasal sinuses and rhinopharynx, only 4 cases were reported [8].
The imaging characteristics of neurilemmomas are important because, together with the symptoms, they allow a presumptive preoperative diagnosis and sometimes determine the nerve of origin. This allows for better planning of surgery and prediction of possible residual nerve deficit.
On tomography, areas of central hypodensity are usually observed with peripheral enhancement due to greater vascularization versus cystic and necrotic regions.
In the MRI, they are isodense or hypodense on T1 and heterogeneously hyperintense on T2, and they enhance little with contrast [9].
In some cases, the neoplasm can be seen originating from a nerve trunk, as in the case described in the patient with a tumor originating from the infraorbital nerve.
In our study, we were able to make a presumptive preoperative diagnosis of a neural type tumor in three patients, according to the clinic, site of origin, and imaging characteristics in three patients.
However, we performed preoperative endonasal biopsies in two patients with bulky tumors and in another with intracranial extension.
The treatment of these tumors is surgical, with the intention of performing a complete resection. Its growth is slow, therefore subtotal resection may be indicated in tumors adhered to neurovascular structures, as in the case of the patient described in our study who had intracranial and vision compromise.
In patients with asymptomatic neoplasms, elderly patients, or with comorbidities, clinical monitoring may be indicated.
Depending on the location and size of the tumors, the surgical approach may vary. Endonasal surgery or the uses of an external approach assisted with endoscopes are the most widely used techniques.
The poor vascularization of these neoplasms favors endonasal resections, even in large tumors. The intracapsular dissection technique can be used to collapse the tumor and complete the resection or perform an extracapsular excision.
In tumors involving the pterygomaxillary fossa, the endonasal approach with endoscopes is also possible. Using a wide middle maxillary antrostomy, the pterygomaxillary fossa can be approached and complete resections performed, as in the case described in our study.
It is uncommon in the nasal cavity or in the paranasal sinuses to identify the origin of the tumor and try to preserve the function of the nerve.
Some studies describe the intracapsular dissection technique of neck schwannomas, especially those that originate from the pneumogastric nerve, identifying and preserving some nerve fibers to try to preserve the function of the nerve [10,11].
In the case of schwannoma originating in the infraorbital nerve, an attempt was made to preserve function by intracapsular dissection, but no nerve fiber could be preserved; despite this, the patient recovered sensitivity in the maxillary region, with only a small deficit persisting in the lower sector.
In a study of 52 patients with schwannomas of the nasal cavity and skull base operated endonasally with endoscopes (18/52) and through a transmaxillary sublabial approach assisted with endoscopes (34/52), they reported a total resection rate of 80.8% (42 patients), subtotal of 15.38% (8/52) and partial of 3.84% (2/52). They had 5 cerebrospinal fluid fistulas that were repaired with fascia lata and a nasoseptal flap. There were 4 recurrences during follow-up (6 to 134 months) [12].
In another study they reported 10 patients who were treated for schwannomas of the nasal cavity and paranasal sinuses by endoscopic surgery, all were disease-free during a follow-up of 2-120 months, and none required an external approach [13].
In our study, a complete resection was performed in 4 patients, and no recurrences were detected during an average follow-up of 2 years. In another patient with intracranial extension who had bilateral visual compromise, the resection was subtotal.
The incidence of nasosinusal schwannomas within the nerve tumors diagnosed in the head and neck was 31.25% (5/16).
Endoscopic excision was very safe and effective to treat the patients with nasosinusal schwannomas.
We believe that the endonasal approach with the assistance of endoscopes is the surgical technique of choice to treat schwannomas of the nasal cavity and paranasal sinuses, regardless of their size.
The authors have none to disclose.