Implantation of a voice prosthesis has become a standard practice for vocal rehabilitation in patients that have undergone a laryngectomy. Their complications usually concentrate in the throat region and few were reported being gastrointestinal. We describe a case of a life-threatening intestinal perforation related to the unnoticed ingestion of a voice prosthesis in a laryngectomized patient.
A 75-year-old patient, known for a glotto-supraglottic carcinoma who had undergone total laryngectomy with voice prosthesis replacement, was referred for acute abdominal pain. An emergency median laparotomy showed a perforation of the distal ileum due to seven foreign bodies turning out to be voice prostheses.
In patients with phoniatric devices with (unnoticed) ingestion, abdominal pain can be a sign of a life-threatening complication such as intestinal perforation.
Voice prosthesis, Intestinal perforation, Mechanical ileus
In the past decades, implantation of voice prostheses has become standard practice for vocal rehabilitation in patients that have undergone a laryngectomy [1]. Although the attractiveness of these devices and the simplicity of their use have been well established [2], they are not without complications. In the literature, few reports have evaluated the range of these adverse events and they seldom go beyond the scope of the tracheoesophageal complications (leakage, phonatory failure, prosthesis dislodgement, infection, aspiration) [3]. We describe a case of a life-threatening intestinal perforation related to the unnoticed ingestion of a voice prosthesis in a laryngectomized patient.
In February 2021, a 75-year-old man was referred to our emergency department due to acute abdominal pain and constipation.
The patient was known for a glotto-supraglottic squamous cell carcinoma (T2 N0 M0) which was treated in 2007 by tracheotomy and total laryngectomy with voice prosthesis placement. In 2008, he presented a first laryngeal stenosis requiring placement of a silicone canula before placement of a Provox-free hand device in 2009. Between 2011 and 2015, he underwent several interventions for obstructions of the trachea motivating a Provox prosthesis replacement size 10 mm.
In May 2018, the patient was diagnosed with a relapse of squamous cell carcinoma of the left amygdalian pillar and palace veil which was treated with radiotherapy and monoclonal antibody treatment. He needed a percutaneous endoscopic gastrostomy that he kept for a year. After this episode, his alimentary habits were normal.
In early 2020, pulmonary nodules compatibles with metastasis were detected, with further investigations refused by the patient.
In December 2020, he was hospitalized for an incidental inhalation of his voice prosthesis, after referring ongoing laxity of his prosthesis. A bronchoscopy retrieved the prosthesis in his right bronchus. The intervention was followed by the implantation of a smaller Provox prosthesis, size 8 mm. However, the patient was readmitted for a total of three episode of prosthesis inhalation. Due to the prosthesis laxity, the ENT surgeon chose to close the tracheoesophageal fistulae and introduced a Fistula Prosthesis. The patients took care of his prosthesis daily and autonomously.
In February 2021, the patient was referred to our emergency department due to abdominal pain, abdominal distension and total constipation throughout a 72 hours' period. He presented with nausea and vomiting through the tracheostomy. He did not refer swallowing his voice prosthesis and had an unremarkable digestive history. He was dyspnoeic (respiratory rate 23/min) with 92% of saturation, had tachycardia (100/min), normal blood pressure (135/90) but was afebrile. The abdomen was painful on palpation with tenderness in four quadrants. Laboratory work-up indicated an inflammatory syndrome with CRP of 428 mg/L and leucocytosis of 12.9 G/L. The blood gas showed acidemia with hyperlactatemia (3.2 mmol/l). A CT-angiography of abdomen revealed a pneumoperitoneum in the right iliac fossa associated with intra-abdominal free fluid. The walls of the distal ileum were globally thickened (Figure 1). Remarkably, 7 tubular foreign bodies were discovered inside the ileum.
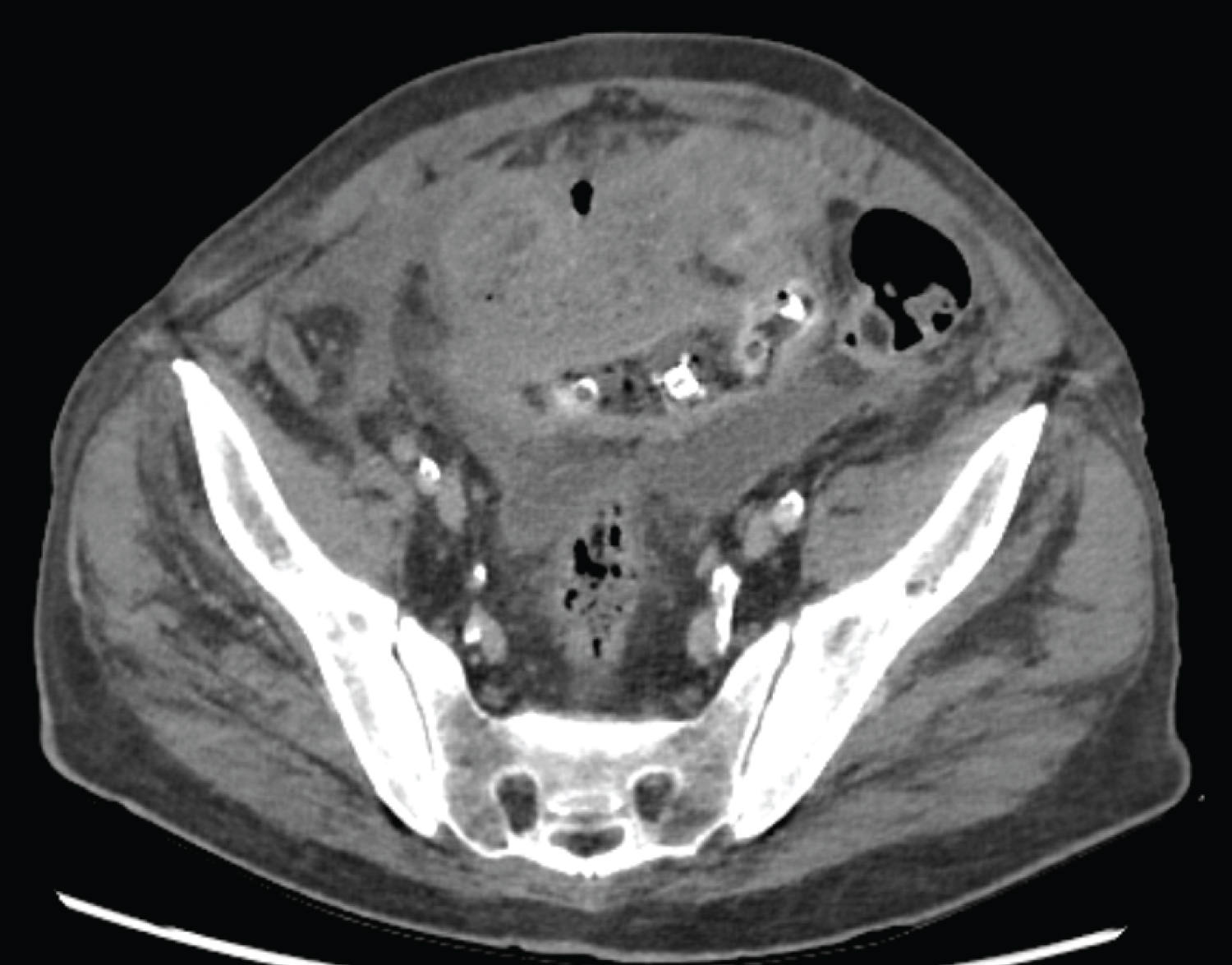 Figure 1: Thickness of the walls of the distal ileum.
View Figure 1
Figure 1: Thickness of the walls of the distal ileum.
View Figure 1
At this point, a differential diagnosis of ileum perforation or mesenteric ischemia could not be ruled out due to the foreign body or/and due to a systemic disease. An antibiotic treatment with piperacillin-tazobactam was initiated.
The patient was brought to the operating room for urgent exploration. We performed a rapid sequence induction and proceeded to intubation with a Laryngoflex® tube 8.0 mm through the tracheostomy. We had no complication and inserted a nasogastric tube to empty the stomach.
An urgent median laparotomy demonstrated a four quadrant-peritonitis with pus. After it was cleared with 29 litres of peritoneal lavage it revealed a covered perforation of the distal ileum at 15 cm from the ileocecal valve. Around the perforation, 10 cm of the segment was inflammatory, fragile and the 7 foreign bodies could be palpated (Figure 2). We opened the segment and discovered the pieces of 7 phonatory valves (Figure 3 and Figure 4).
 Figure 2: Seven foreign bodies further identified as phoniatric valves located in the distal ileum.
View Figure 2
Figure 2: Seven foreign bodies further identified as phoniatric valves located in the distal ileum.
View Figure 2
 Figure 3: Phoniatric valves after surgical removal.
View Figure 3
Figure 3: Phoniatric valves after surgical removal.
View Figure 3
 Figure 4: Phoniatric valve after surgical removal.
View Figure 4
Figure 4: Phoniatric valve after surgical removal.
View Figure 4
A segmentectomy of the ileum was performed and the abdominal wall was closed with a laparostoma. A second look two days later found that the abdomen had no more signs of infection or inflammation; the anastomosis of the small intestine was performed and the abdominal wall closed.
The bacteriology of the peritoneal fluid returned positive for Escherichia coli and multi sensitive Enterococcus avium. The antibiotic was deescalated after 7 days to amoxicillin-clavulanic acid which was administered during 7 more days.
The patient's evolution was favourable and the laboratory results improved over this time period. However, the ENT team still had to manage tracheoesophageal fistula, the patient was discharged 21 days later.
As expected, the results of the pathology showed intraluminal foreign bodies with an extensive mucosal ulceration and a covered perforation with severe acute and subacute peritonitis. The pathologists could not exclude an inflammatory bowel disease (IBD). Thus, we decided to perform a colonoscopy and ileoscopy 6 weeks after the first operation. The biopsies of the colon and the ileum were normal, without any sign of inflammation.
To the best of our knowledge, a mechanical ileus with perforation due to the voice prosthesis has never been yet described in the literature.
With an estimate of 500,000 new cases each year, oral and oropharynx cases remain among the most common cancers worldwide [4]. In some of these patients, the treatment includes a laryngectomy, which involves the excision of the larynx and a tracheostomal formation in the upper sternal notch resulting in loss of voice [5]. Vocal restoration is thus a major concern in the subsequent care and rehabilitation of these patients. Voice prosthesis are nowadays the standard of care for such purposes. In 1980, Blom and Singer created the first device which was then modified through the years, followed by Eska-Hermann and then in 1988, the Provox prosthesis was developed with many new models coming up. These devices, when placed in a surgically formed tracheoesophageal fistula, create an air shunt from the respiratory system into the oesophagus, thus allowing for a hands-free communication [6]. Their main advantage lays in the simplicity of their maintenance. Especially with new prostheses as Eska-hermann or Provox. Comparison of those prosthesis shows differences in complications and quality. Blom-Singer prostheses showed more complications and less longevity [7]. Even though Provox provides more quality speech, Eska-Hermann shows less complications [8]. According to Alper Yenigun & co [9] the most important factor influencing the longevity of the Provox voice prostheses is the follow-up. The mean duration is usually 14-19 months. The success of prosthetic voice rehabilitation in laryngectomies depends upon qualified follow-up care by the otorhinolaryngologist [10].
Also, Demir, et al. showed that in situ lifetime of Provox was not influenced by age, radiotherapy, insertion time, and the period between radiotherapy and insertion time of prosthesis [11]. The patient factor is the most important factor that affect the in situ lifetime of Provox [11]. In our case, the patient was followed by ENT doctors and came to the hospital only for complications. The loss of those several valves had not apparently been noticed.
Nevertheless, these tracheoesophageal fistulae are not without complications. In the few reports available in the literature, the most frequently reported complications are leakage around the prosthesis (from 5 to 65%), prosthesis displacement (5-32%), widening or narrowing of the tracheostoma (5-21%), aphonia or dysphonia (5-7%), aspiration of the prosthesis (5-7%) and infection or colonization (4-5%), cervical cellulitis, mediastinitis, deep neck abscess. Development of granulation tissue around the prosthesis and/or shunt insufficiencies are relatively rare [10].
All digestive complications described were rare and reported as gastric distension, dysphagia and gagging [1-3,12]. Other complications described were oesophageal perforation [9].
To our knowledge, the only report of a severe abdominal complication related with these devices was described by Hiltmann, et al. [6] "a case of a mechanical ileus shortly after device replacement". As in our report, the patient also presented a prosthesis retention in the ileocecal valve and required laparotomy for the extraction of the foreign body.
Foreign body ingestion, though frequent in children, is not rare in adults. 80 to 90% will pass through the digestive tract without any complication, but an endoscopic (10-20%) or even surgical intervention is sometimes required (1-14%) [13]. The surgical approach is often reserved for patients in which endoscopic retrieval was unsuccessful or complications emerge, such as perforation, GI tract obstruction or bleeding [14]. Perforation is the most frequent complication (< 1%) and clinical presentation may vary, depending on the composition, the time since ingestion, and site extrusion. Indeed, perforation is frequently more severe in jejunum and ileum, when compared with stomach or large intestinal ones [15]. Clinical history and computed tomography remain gold standard for the preoperative diagnosis, especially for nonmetallic objects or when doubts of complications are suspected. Though a laparoscopic retrieval may be advantageous because of the increased magnification and direct illumination - especially in case of small foreign bodies-, laparotomy remains preferable for the management of complications [13].
This case highlights the difficulties in the management of voice prosthesis, whose digestive complications however rare must not be underestimated. The ingestion of any type of foreign bodies, even small blunt ones which are considered low risk, is not to be belittled as it can cause severe, potentially life-threatening, complications. Because it can be unnoticed and life-threatening, clinicians should be aware of gastro-intestinal complications, such as perforation, caused by ingestion of a voice prothesis. We suggest that a revision of any oro-esophageal implanted medical device should be considered in patients with phoniatric device who present an abdominal pain of unclear origin.
None.
None.