To investigate the gender distribution in current otolaryngology residency programs and examine associations between the presence of female program directors or department chairs, number of female faculty, and number of female residents within residency programs in the United States.
A cross-sectional analysis of current otolaryngology programs, presence of female chairs, program directors, faculty and residents in 2019 was performed. The gender of the program director, departmental chair, number of female faculty, number of residents within each program, and the gender distribution of listed residents was determined by visiting each otolaryngology training program's website.
Of the 1,641 otolaryngology residents in the United States, 569 were female (34.7%). There are currently 31 female program directors (26.5%), 5 female otolaryngology department chairs (4.2%), and 526 female faculty (24.5%). There was a significant association between the number of female faculty members and female residents (r = 0.545, p < 0.001).
The presence of a female department program director or chair was not associated with the current number of female residents. However, the number of female faculty was positively correlated with the number of female residents within a program.
Program directors, Gender balance, Department chair
Historically, women were discouraged from pursuing education in general, and particularly medicine, throughout the first millennium A.D. In fact, medical education was outlawed for women throughout Europe [1]. Within the last 200 years, the presence of women in medicine has steadily changed. Multiple medical schools, including The Women's Medical College of Pennsylvania, later renamed to The Medical College of Pennsylvania, opened in the 1850's. This provided opportunities for women to breach a historically patriarchal medical community [2].
In otolaryngology, there have been a number of influential women. Margaret Butler, MD is widely regarded as the first female otolaryngologist, and Eleanor Maxine Bennett, MD, is considered to be the first female department chair in the United States [2]. While significant changes have occurred in many areas of medicine resulting in more equitable distribution, other areas continue to lag behind in equitable gender representation.
In 1985, only 25% of medical students were female [3]. In 2019, for the first time, females were the majority (52.4%) of matriculating medical students [4]. In 2017, women represented 35.2% of all actively practicing physicians across all specialties in the United States [5]. There is significant gender disparity within specialties demonstrated and various explanations have been given regarding the reasons some specialties have more females (Figure 1) [5].
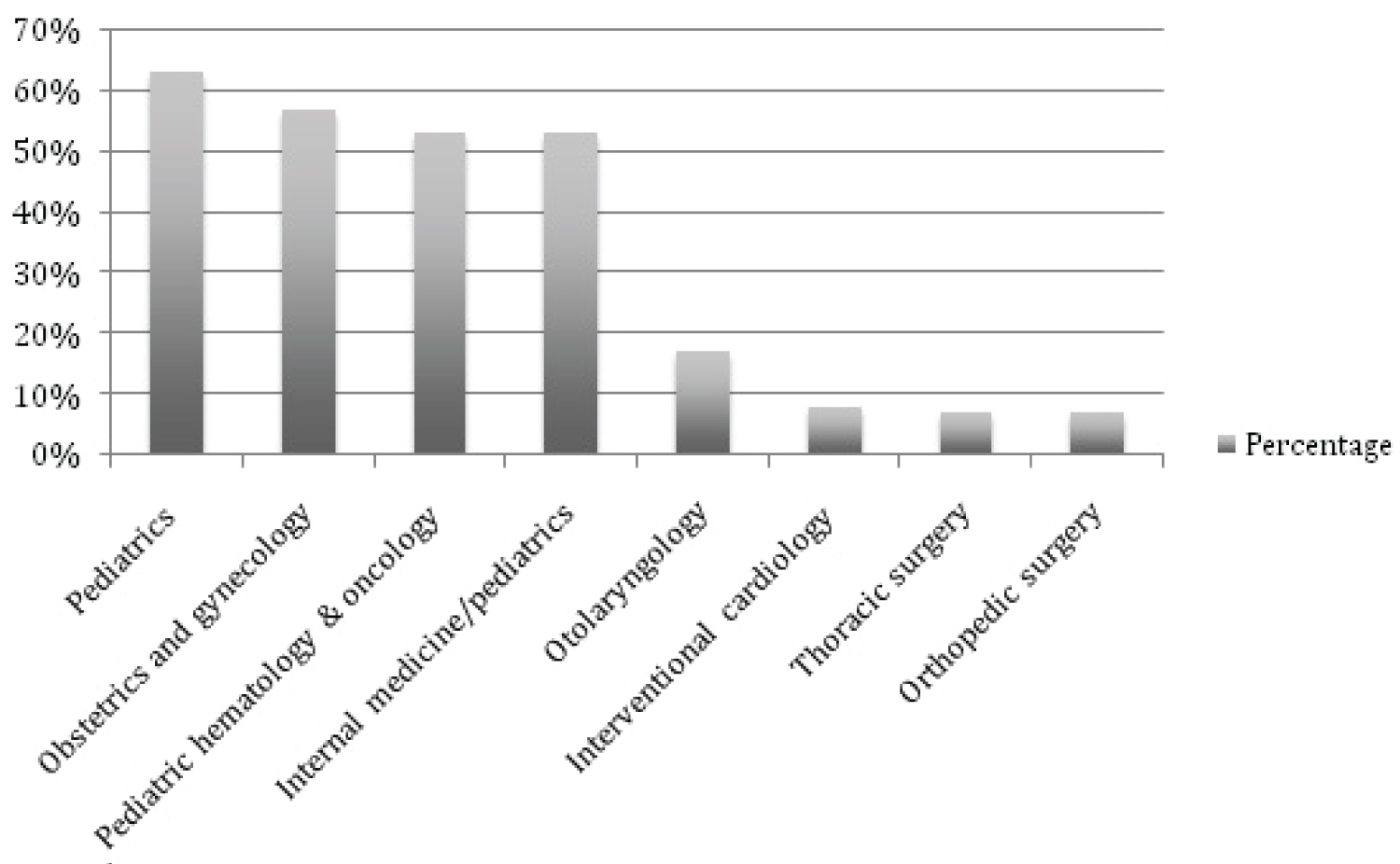 Figure 1: Percent of active female physicians by specialty [5].
View Figure 1
Figure 1: Percent of active female physicians by specialty [5].
View Figure 1
In 1963, 0.3% of practicing otolaryngologists were women [2] and the percentage has steadily increased to 11.2% in 2008, and to 17% by 2017 [5-7]. This is a significant change in 50 years, but otolaryngology-head and neck surgery lags behind the representation of women in other specialties (Figure 2). Litvack, et al. reported that women were underrepresented on 8 of 9 otolaryngology editorial boards. Women had representation at the associate or section editorship level; however, none of the journals had women editor-in-chief's [8]. Epperson, et al. noted that women are underrepresented in positions of department chair and residency or fellowship director [9]. It is important to note that this gender disparity in academic appointments is consistent across all medical specialties and academia more generally. Jena, et al. noted that women physicians at medical schools were significantly less likely than men to be full professors [10]. Silver, et al. reported that in particular neurology women are often underrepresented and less frequently named for physician recognition awards [11].
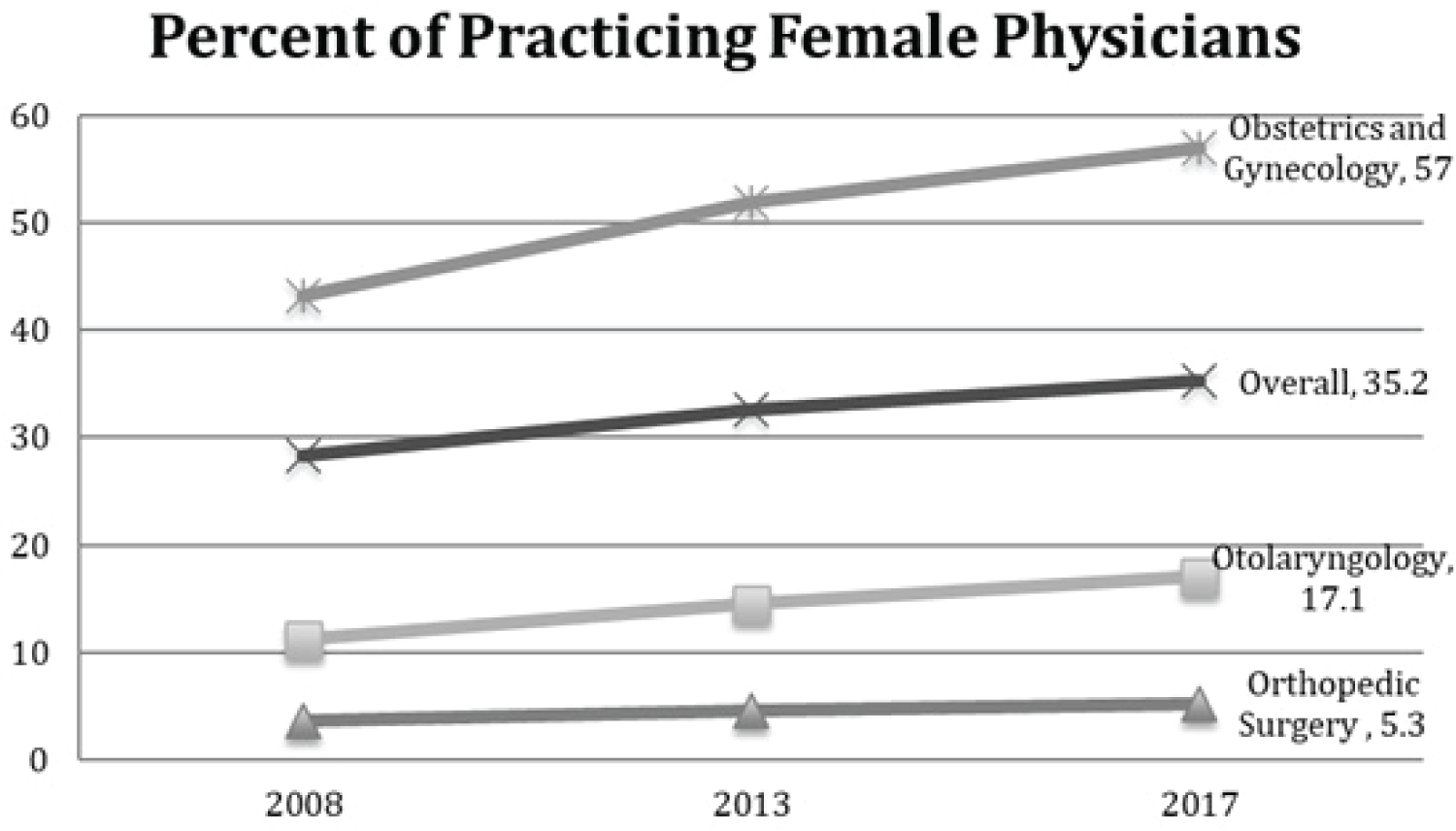 Figure 2: Practicing female physicians by specialty in 2008, 2013, and 2017 [5-7].
View Figure 2
Figure 2: Practicing female physicians by specialty in 2008, 2013, and 2017 [5-7].
View Figure 2
It is unclear why fewer women choose otolaryngology as a career than certain other medical or surgical specialties. Science, technology, engineering and mathematics have been recognized as areas where gender and racial disparities exist [12]. Discussions have centered on whether it is an issue of "pipeline", which refers to sufficient input of students at the beginning of their studies, and retaining these students through completion of their academic program. It is not possible to become an otolaryngology resident if an appropriate number of women are not in medical school. The fact that the majority of medical students are female does not explain why fewer women choose surgical subspecialties and comprise less of the workforce [4]. Work life balance and lack of role models within certain surgical specialties has been suggested as possible reasons for the disparity [13].
The current study aims to investigate the gender distribution in modern otolaryngology training programs and determine if there is an association between the presence of female program directors, departmental chairs, and number of female faculty and the number of female residents in residency programs in the United States.
A cross-sectional analysis of current otolaryngology training programs in the Summer of 2019 was performed. The gender of the program director, chair, and number of female faculty, number of residents within each program, and the gender distribution of current residents was gathered via the available otolaryngology training program's website.
Exploratory analyses were performed to examine the distribution of each variable, to determine the Spearman's correlation coefficient between number of female faculty and number of female residents, and the number of female residents by the gender of the department chair (i.e., female or male chair) or program director. Because the dependent variable is a count measure, univariate Poisson regression models were constructed where the number of female residents was the dependent variable and the number of female faculty, whether a program's chair was female, and whether a program director was female were each independent predictors. Results are presented using exponentiated beta estimates and their 95% CIs. Statistical significance is set at p < 0.05. All analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, NC).
One hundred seventeen otolaryngology training programs were analyzed (Table 1). In the United States, there were 5 female chairs out of 97 chairs of otolaryngology nationally in 2019, accounting for 4.9% of all otolaryngology chairs. There were 31 female program directors, representing 26.5% of all otolaryngology program directors. There were 2,140 active faculty in 106 training programs and of these, 526 (24.6%) were women. Eight programs did not have any female faculty. The highest number of female faculty in a program was 21. There were 1,641 otolaryngology residents within the United States and 469 (34.7%) were female.
Table 1: Descriptive statistics at level of training program. View Table 1
Data regarding current program chairs was unable to be obtained for 15 training programs. Faculty data was unable to be obtained for 11 programs. For those programs in which these data were unavailable, the majority were programs sponsored by the Army or Navy programs, which did not list their faculty or residents.
Using Spearman's correlation coefficient, an association between the number of female faculty members and female residents was positively correlated (r = 0.545, p < 0.001). The Poisson regression estimate in Table 2 for female faculty is 1.08 (95% CI 1.06, 1.10) indicating that for every 1-person increase in female faculty, the number of female residents increases by 8%.
Table 2: Effect of each independent variable on the number of female residents. View Table 2
The mean number of female residents in the 5 institutions with female chairs was 5.2 (standard deviation [SD] = 2.2), while it was 5.3 (SD = 3.2) in the 97 institutions with male chairs. The Poisson regression estimate in Table 2 for female faculty was not statistically significant at 0.98 (95% CI 0.66, 1.46). The mean number of residents in programs with female chairs (M = 16.6, SD = 5.7) was not statistically significant (p = 0.489) when compared to the mean number of residents in all analyzed programs (M = 14.7, SD = 5.9).
The mean number of female residents in the 31 institutions with female program directors was 5.2 (SD = 3.3) while it was 5.8 (SD = 3.1) in the 86 institutions with male program directors. The Poisson regression in Table 2 for female program directors was not statistically significant at 1.08 (95% CI 0.90, 1.29). The mean number of residents in a program with a female program director is 14.5 (SD = 7.1). The mean number of residents in a program with a male program director is 13.9 (SD = 5.6). This was not significantly different (p = 0.852).
An increased number of female faculty was positively associated with the number of female residents in an otolaryngology residency program. The presence of a female program director or department chair was not significantly associated with an increased number of female residents. Eloy, et al. postulated that a contributing factor to the data showing female medical students gravitating towards primary care positions and away from surgical subspecialties was due to a lack of female mentorship in surgical subspecialties [14]. Adler noted that mentees tend to look for a mentor who is in similar likeness [15]. The residency selection process is usually done with the input of the residency program faculty regarding the applicants that are invited to interview and then ranked. The presence of an increased number of women involved in the selection process may impact the selection for interview and eventual ranking of female applicants. This might be the reason for the increased number of female residents at residency programs with a greater number of female faculty.
The National Resident Matching Program uses an algorithm to "match" medical students to residency positions. The algorithm is applicant-proposing and matches the preferences of both the applicant and the program, with the applicant preference taking priority [16]. Within this system, it is important to have an adequate number of female applicants interested in the residency program since the process, in some degree, is bidirectional. Johnson, et al. noted that as the number of women in an applicant pool increases, there is a higher likelihood of the female applicant being hired [17]. This is evident in more female-prevalent fields such as obstetrics and gynecology, where 57% of the practicing physicians are female [5]. While obstetrics and gynecology is a surgical specialty with significant on-call demands, female medical students continue to gravitate to the practice. It is assumed that female faculty are mentoring medical students and residents within these training programs. Additionally, as people inherently tend to gravitate towards likeness, an increased number of female faculty could make female applicants more comfortable and attract more female medical students. Indeed, the data of the current study supports this, indicating that with each incremental increase of 1 female faculty within a department, the number of female residents within the program increases by 8%.
It is important to note that there are only 5 female program chairs within the United States. Colletti, et al. noted that the factors that seem to make women more hesitant to pursue academic positions are feelings of responsibility to one's family, lack of mentorship, and gender bias [18]. However, in the current study, the presence of a female chair, a highly visible position, was not associated with an increased number of female residents within that program.
Females currently comprise 34.7% of all otolaryngology residents. If one were to extrapolate this data, it can be expected that the number of female practicing otolaryngologists will continue to increase. While it is known that women are underrepresented in academic leadership positions [9] and on otolaryngology journal editorial boards [8], women are proportionately represented in junior leadership positions [9].
Limitations of this study include the fact that it is a cross-sectional analysis of residents in 2019. Therefore, the length of time that each faculty member was in their position was not available to determine if it impacted resident selection. It was also not possible to determine the number of female applicants for each program that resulted in the number of females being invited for interview and ranked in the match. The very small sample size of female chairs (N = 5), confounds the data that the presence of a female chair does not correlate with an increased percentage of female residents. Finally, the data for the current study relied on what was available on the program website during the Summer of 2019. It is not known how often programs update their websites and how accurate information on the websites are. Additionally, there were programs that did not have data listed, particularly those in the military.
Despite these limitations, the current study offers a view of gender distribution in otolaryngology departments and training programs. Future research should evaluate the process used during application, interview, and ranking of female applicants to otolaryngology residency training. Qualitative research examining the reasons behind applying, offering interviews, and ranking of female applicants would aid in better understanding the gender disparity that currently exists within otolaryngology.
A possible lack of female mentorship has been hypothesized as a source of female medical students' lack of pursuit of a career in otolaryngology. The current study demonstrated an association between an increased number of female faculty and an increased number of female residents within a residency. Further research is needed to better understand how female medical students navigate the application process and the methods that programs use to select and rank applicants.
The authors have no funding, financial relationships, or conflicts of interest to disclose.
The data from this manuscript was presented as an oral presentation at the Triological Society Combined Sections Meeting, Coronado, CA, USA, January 23-25, 2020.