Pathophysiology of benign paroxysmal positional vertigo (BPPV) is canalolithiasis in the semicircular canal. The principle of Epley maneuver is moving debris from a long arm to the utricle, therefore debris stimulates the utricular macula in the sitting position after the treatment. To clarify the characteristics of eye movements evoked by the stimulation of unilateral macula of the utricle.
The subjects were ten patients with posterior semicircular canal BPPV. After the diagnosis, we performed Epley maneuver immediately. We observed and recorded eye movements in the sitting position (chin-down 30°) just after the treatment.
No one showed nystagmus in the sitting position after the treatment. In all patients, positional nystagmus disappeared two days after the treatment.
Nystagmus does not occur by the stimulation to the macula of the utricle.
Benign paroxysmal positional vertigo, Canalolithiasis, Epley maneuver, Otolith ocular reflex, Video-oculography
Peripheral vestibular disorder, which causes provocative vertigo and robust torsional nystagmus in the head-hanging position, is known as benign paroxysmal positional vertigo (BPPV) and was formerly thought to be an otolith organ disorder [1]. However, the canalith repositioning procedure [2] and operative findings [3] supported the theory of canalolithiasis in the posterior semicircular canal. Previous studies demonstrated the efficacy of the Epley maneuver, and it is used worldwide for the purposes of treatment [4]. The principle of the Epley maneuver is the movement of debris from the long arm to the utricle, which stimulates the utricular macula in the sitting position after the treatment (Figure 1).
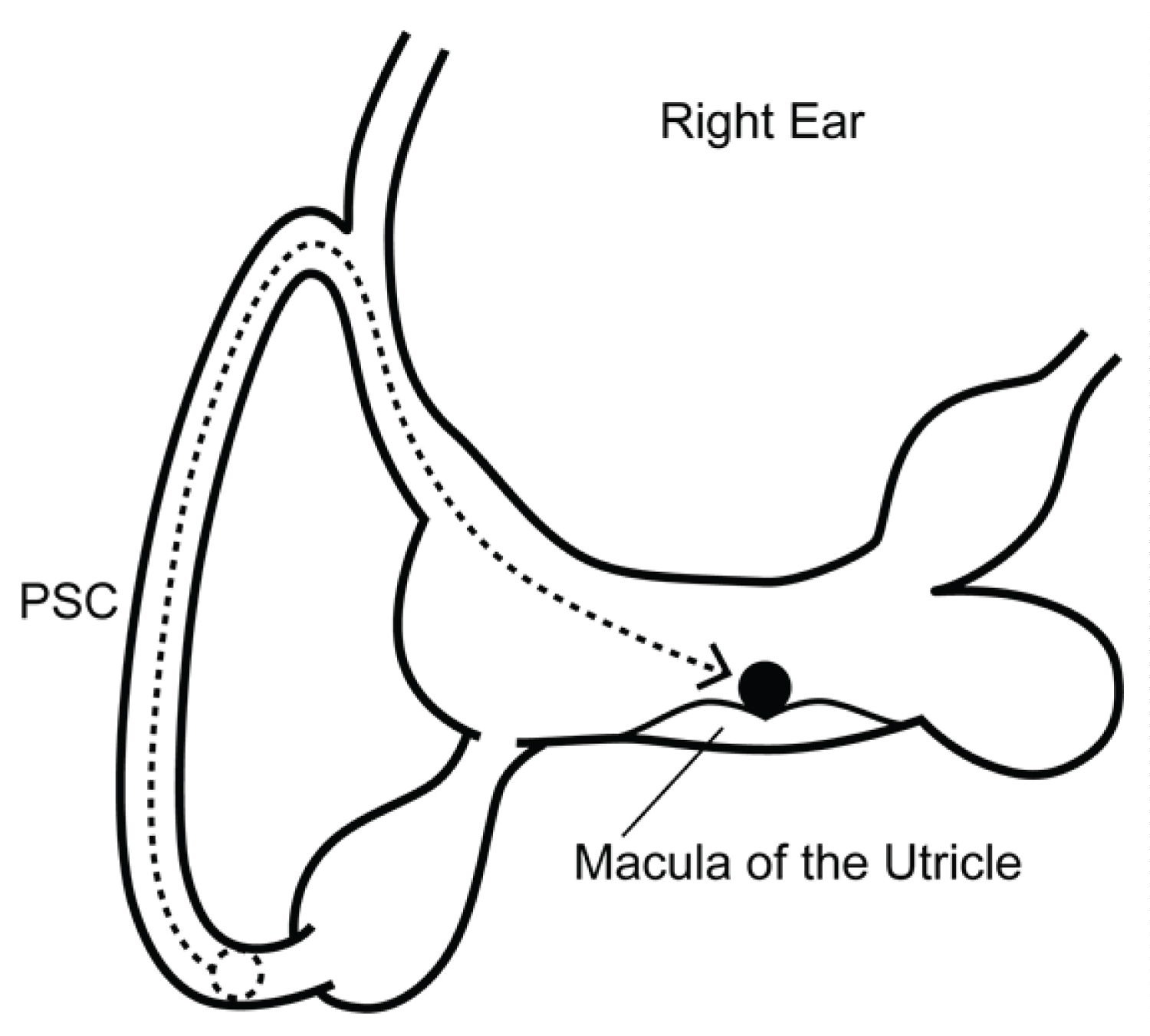 Figure 1: Pathological debris stimulates the macula of the utricle just after the Epley maneuver. For the sake of convenience, the lateral canal is omitted. Black circle means pathological debris. PSC = posterior semicircular canal.
View Figure 1
Figure 1: Pathological debris stimulates the macula of the utricle just after the Epley maneuver. For the sake of convenience, the lateral canal is omitted. Black circle means pathological debris. PSC = posterior semicircular canal.
View Figure 1
The utricular macula is located on the floor of the utricle, approximately in the plane of the lateral semicircular canal, and is oriented to respond best to lateral (ear to shoulder) tilts and side-to-side or fore-and-aft translations of the head. Although excitation of hair cells may produce eye movements, the details of the otolith ocular reflex are unknown.
In animal experiments, electrical stimulation of the utricular nerve produced various patterns of eye movements. Suzuki, et al. [5] reported that there was a vertical deviation of the optic axes (skew deviation) and a horizontal deviation, in addition to a torsional component. Moreover, Goto, et al. [6] reported that horizontal eye movements were evoked. However, there is not a physiological consensus regarding otolith ocular reflex.
The aim of the present study was to clarify the characteristics of eye movements evoked by the stimulation of unilateral macula of the utricle.
The subjects were ten patients with posterior semicircular canal BPPV who visited our institution between January 2022 and April 2022.
1. The Dix-Hallpike test [1] revealed upward vertical and torsional nystagmus with some latency period in the head-hanging position.
2. In the sitting position, vertical and torsional nystagmus occurred, and the direction was opposite to that in the head-hanging position.
3. In both positions, nystagmus stopped within 1 minute.
4. Epley maneuver was effective.
1. Cochlear symptoms related to vertigo.
2. Central nervous system disorders.
3. History of head trauma.
Nystagmus testing was performed in the dark with the patients' eyes open using an infrared charge-coupled device camera. Eye movements were recorded and converted to digital data. Three-dimensional video-oculography was performed using ImageJ version 1.36 software (a public domain, Java-based image-processing program developed at the National Institutes of Health). For analysis of horizontal and vertical components, the XY center of the pupil was calculated. For analysis of the torsional component, the whole iris pattern, which was rotated in steps of 0.1°, was overlaid with the same area of the next iris pattern, and the angle at which both iris patterns showed the greatest match was calculated [7].
After the diagnosis, we performed the Epley maneuver. The detail of treatment is available elsewhere [4]. We observed and recorded eye movements in the sitting position (chin-down 30°) just after the treatment.
Video-oculography results of patient no. 6 are shown in Figure 2. A movie of patient no. 3 is shown in Supplemental Material (Video 1). Just after the treatment, none of the patients showed nystagmus in the sitting position, and none complained of dizziness (Table 1). In all patients, positional nystagmus disappeared two days after the treatment. There were no complaints of residual dizziness.
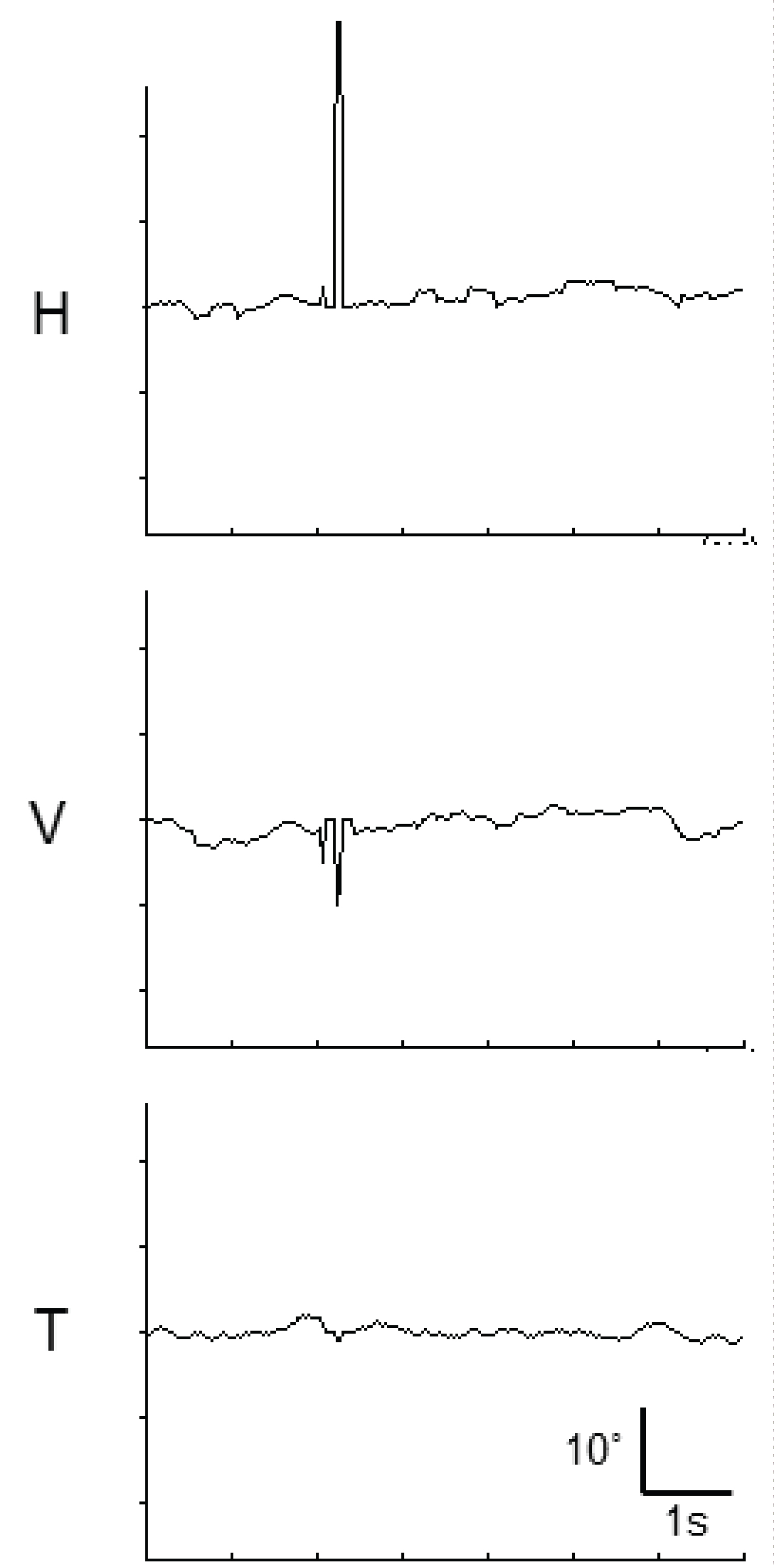 Figure 2: Video-oculography (position trace) of patient no. 5. Just after the treatment, nystagmus did not occur in the sitting position. The upward deflections in horizontal (H), vertical (V), and torsional (T) eye movements are indicated as being toward the right, upward, and right, respectively. Spikes are blinks.
View Figure 2
Figure 2: Video-oculography (position trace) of patient no. 5. Just after the treatment, nystagmus did not occur in the sitting position. The upward deflections in horizontal (H), vertical (V), and torsional (T) eye movements are indicated as being toward the right, upward, and right, respectively. Spikes are blinks.
View Figure 2
Table 1: Results. View Table 1
We found that nystagmus does not occur by stimulus to the unilateral macula of the utricle. In all patients, as both positional nystagmus and dizziness disappeared two days after the treatment, the debris returned to the utricle. Despite the debris stimulating the macula of the utricle, nystagmus did not occur. This phenomenon is a new finding regarding otolith ocular reflex.
Curthoys [8] reported that upward eye movements were evoked by stimulation to the unilateral macula of the utricle using guinea pigs; however, this finding may not be relevant to studies of human responses, because torsional eye movements occur by head tilt in humans.
When a human lies down on the right side, otoconia on the utricular macula move to the right side. If utricle ocular reflex occurs, leftward nystagmus should arise in the same fashion as a leftward lineal acceleration. However, nystagmus does not occur in actuality. This suggests that the utricle does not produce nystagmus (Figure 3).
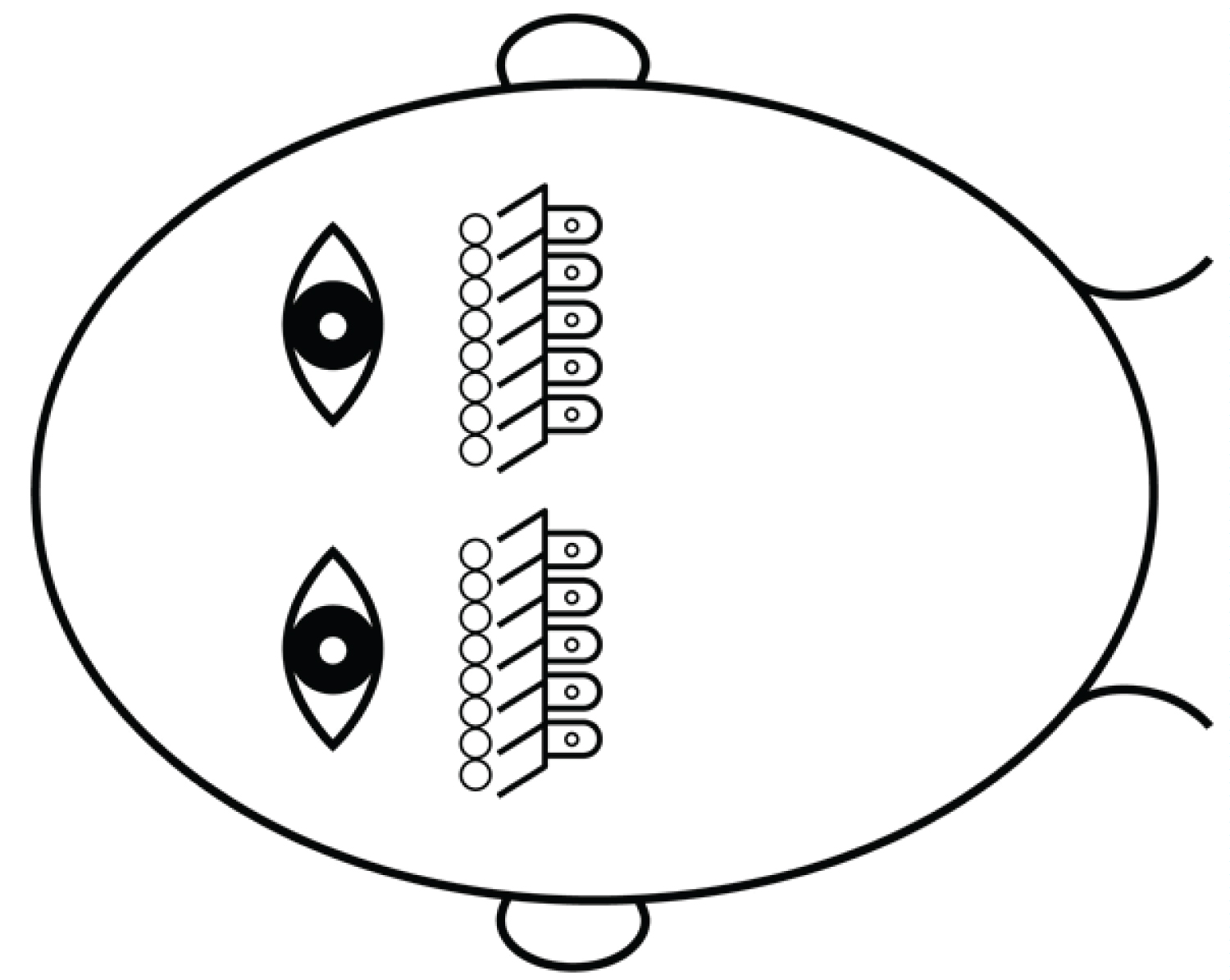 Figure 3: When a human lies down on the right side, otoconia on the utricular macula move to the right side. If utricle ocular reflex occurs, leftward nystagmus should occur in the same fashion as a leftward lineal acceleration; however, nystagmus does not occur in actuality.
View Figure 3
Figure 3: When a human lies down on the right side, otoconia on the utricular macula move to the right side. If utricle ocular reflex occurs, leftward nystagmus should occur in the same fashion as a leftward lineal acceleration; however, nystagmus does not occur in actuality.
View Figure 3
Our findings suggest that the semicircular canal ocular reflex responds to linear acceleration. The head has six semicircular canals that respond to all direction of acceleration. For example, side-to-side movements stimulate the lateral canal cupula and horizontal nystagmus occurs (Figure 4).
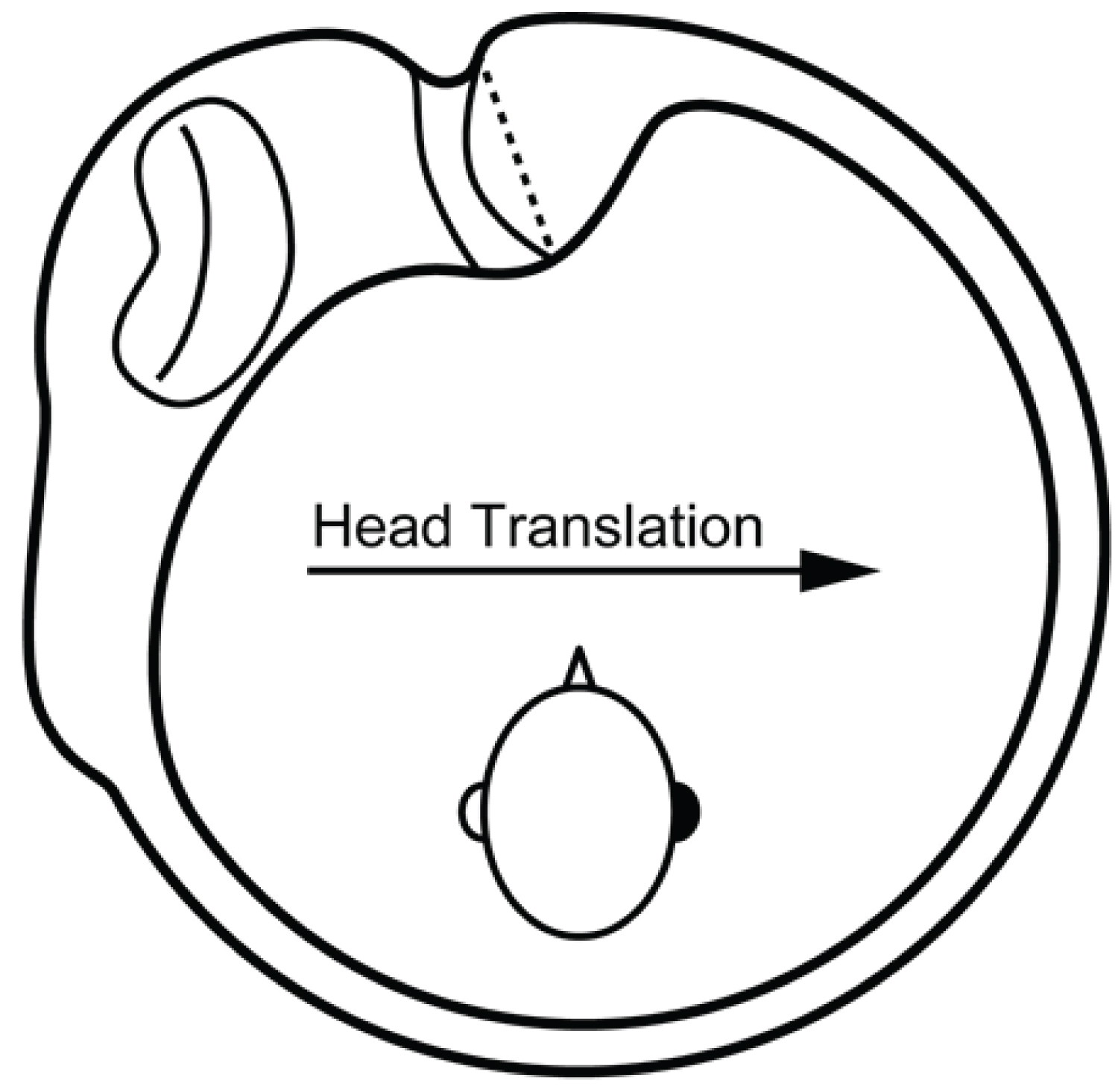 Figure 4: Right lateral semicircular canal. When a rightward force acts on a head, lateral semicircular canal cupulae are excited by the inertia and this leads to a leftward horizontal slow phase of the eyes. As a result, rightward nystagmus occurs.
View Figure 4
Figure 4: Right lateral semicircular canal. When a rightward force acts on a head, lateral semicircular canal cupulae are excited by the inertia and this leads to a leftward horizontal slow phase of the eyes. As a result, rightward nystagmus occurs.
View Figure 4
It is generally believed that ocular counter-rolling is derived from the utricle. There are two types of ocular counter-rolling: dynamic torsion and static torsion. This study suggests that dynamic torsion does not occur from the utricle and is a semicircular canal ocular reflex. However, we did not obtain any findings regarding static torsion because of the limitation of the device. Moreover, we were unable to assess skew deviation as we performed single eye recording.
Nystagmus does not occur by the stimulation to the macula of the utricle; hence, eye movements derived from a horizontal linear acceleration are a semicircular canal ocular reflex.
We thank Dr. Kazunori Futai for preparing some of the figures.
None.
We declare that we have no conflict of interest.
All procedures performed in study involving human participants were in accordance with the ethical board of the Hirosaki Medical Association (certificate number is 2022-12) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.