Organized Hematoma (OH) are benign hemorrhagic lesion that developed in the nasal sinuses. This tumor is a disease that requires attention because it is sometimes accompanied by bone destruction and can grow invasively into the surrounding area. A 17-year-old Japanese male patient visited our hospital complaining of nasal obstruction from about a month ago. CT and MRI imaging studies showed that the tumor was confined to the nasal cavity. Two times biopsies were performed prior to surgery, which allowed for the diagnosis of organized hematoma. A combination of imaging and pathology tests made this diagnosis possible. The surgery was performed under general anesthesia and no preoperative embolization of the tumor was performed. We could intraoperatively identify a cord flowing into the tumor from the medial mucosa of the uncinate process. This cord-like object was considered the base, and with proper treatment, the tumor could be safely removed. Although OH confined to the nasal cavity is rare, it can be safely treated if diagnosed preoperatively and the base is detected intraoperatively.
Organized hematoma, Nasal cavity, Endoscopic surgery, Tumor base
Organized hematoma is the general term for tumorous lesions, mainly hemorrhagic images and clots, and is a rare benign non-neoplastic disease occurring in the sinonasal sinuses. OHs are often associated with bone destruction and must be differentiated from malignant tumors [1]. OHs are locally destructive and dilated and have an occasionally aggressive appearance on imaging studies, but the treatment of organized hematoma is simple and in most case nasal endoscopic surgery provides marked clinical improvement [2]. Several hypotheses have been suggested to explain the etiology of OH, but their exact etiology or pathophysiology has not been elucidated [3,4]. The majority of OH occur in the paranasal sinuses, mainly in the unilateral maxillary sinus, and are rarely confined to the intrinsic nasal cavity [5]. In the present report, we describe our experience with a rare nasal hematoma in a young man, in addition to a case in which the base of the tumor could be identified intraoperatively.
A 17-year-old Japanese male patient visited our hospital with nasal obstruction from about a month ago. No previous history of major illness, he had no regular internal medication. No history of drug treatment for allergy. A nasal fiberscopy performed at the initial examination showed an easily hemorrhagic neoplastic lesion occupying the account for the majority of nasal cavity (Figure 1), a biopsy was carried out. Post-biopsy hemorrhage was minimal and hemostasis was achieved in a few minutes with gauze compression. Five days after biopsy, he was visited again at our hospital for frequent small epistaxis, and also for persistent epistaxis from one hour ago. Persistent bleeding from the tumor was observed and hemostasis was achieved by inserting gauze compressions for 3 days. Because the pathological diagnosis did not lead to a diagnosis, the biopsy was performed again under general anesthesia about two weeks later. The results of the second biopsy showed necrosis, hemorrhage, fibrin precipitation, hemosiderin deposition, vascular growth, there was no evidence of tumor growth (Figure 2). Contrast-CT scan of the head confirmed the presence of a 54 mm mass with strong contrast effect from the early phase in the left nasal cavity (Figure 3). The paranasal sinuses showed soft tissue density, but no obvious contrast effect, which was considered to be a fluid retention. Contrast-CT scan also showed no bone destruction and no tumor infiltration on the base of the skull. Magnetic resonance imaging also showed a mass occupied the middle and inferior nasal passages and protrude into the naopharynx, with moderately low signal intensity on T1-weighted images and uneven high signal intensity with some high signal areas on T2-weighted images (Figure 4). Based on the imaging results, the radiologist suggested the possibility of nasal papilloma. However, based on the results of the second biopsy and imaging studies, we diagnosed a nasal organized hematoma and endoscopic nasal surgery was performed after a further two weeks. The surgery was performed under general anesthesia and no preoperative embolisation of the tumor was performed as there was little or no bleeding observed after the second biopsy. In surgery, after confirming endoscopically that there is no adhesion to the nasal base and nasal septal mucosa, the tumor was reduced from anteriorly while checking for bleeding. After reduction of the anterior part of the tumor, we could identify a cord flowing into the tumor from the medial mucosa of the uncinate process (Figure 5).
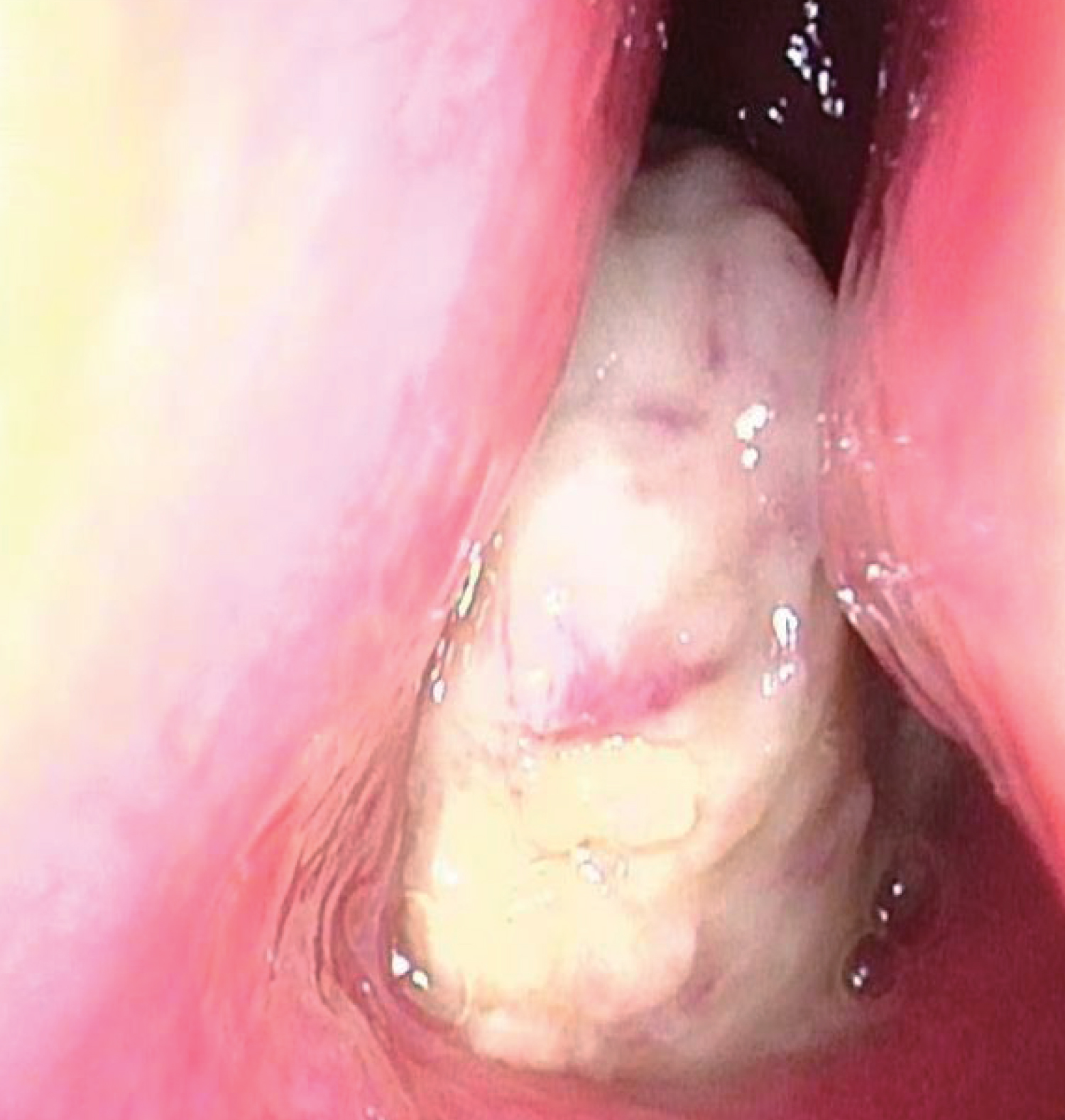 Figure 1: Views of the patient's nasal cavity. The hemorrhagic neoplastic lesion occupied the account for majority of right nasal cavity.
View Figure 1
Figure 1: Views of the patient's nasal cavity. The hemorrhagic neoplastic lesion occupied the account for majority of right nasal cavity.
View Figure 1
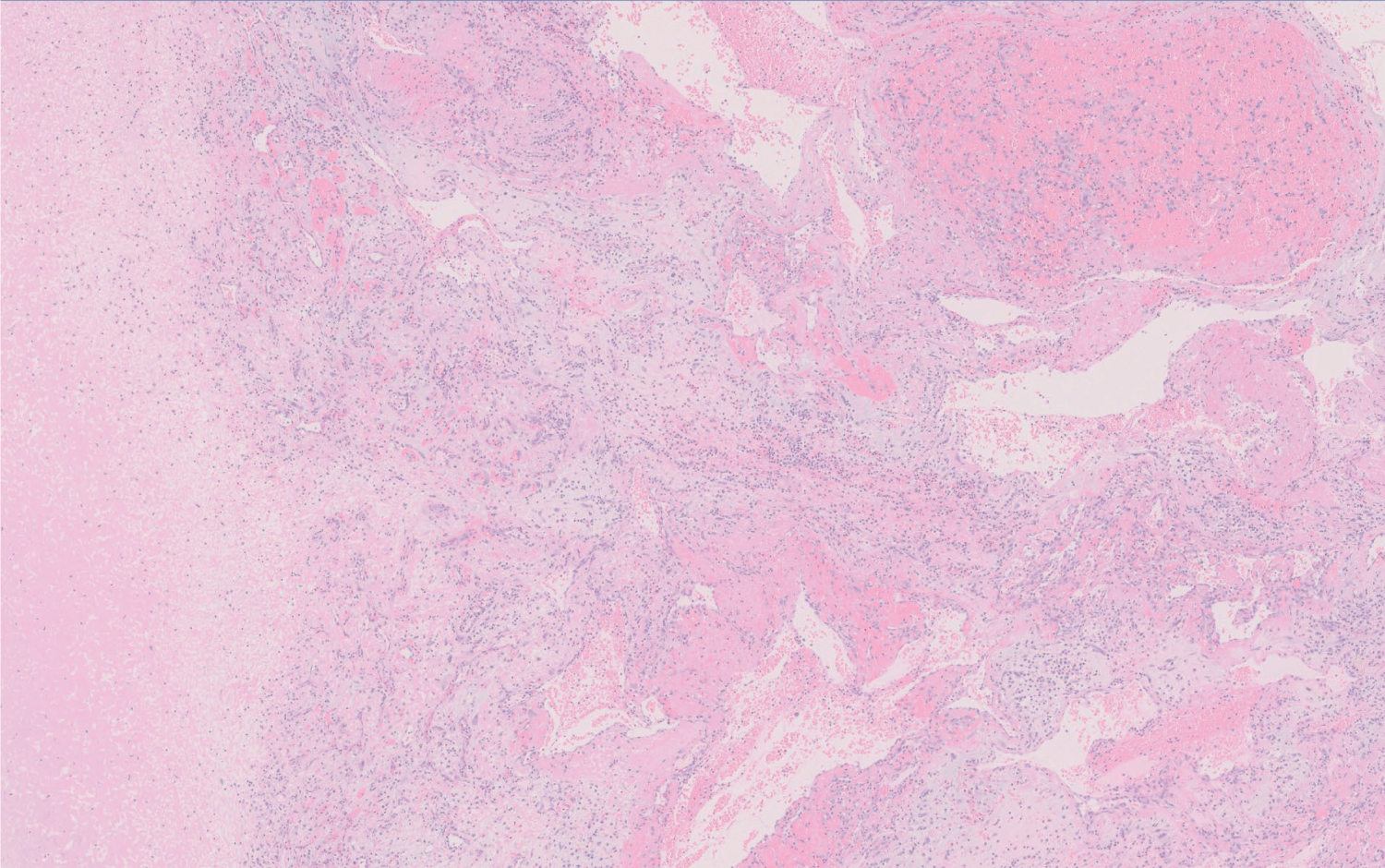 Figure 2: Histopathological evaluation of a biopsy specimen of the tumor necrosis, hemorrhage, fibrin precipitation, hemosiderin deposition, and vascular proliferation were observed in the specimens, but no tumor growth was observed.
View Figure 2
Figure 2: Histopathological evaluation of a biopsy specimen of the tumor necrosis, hemorrhage, fibrin precipitation, hemosiderin deposition, and vascular proliferation were observed in the specimens, but no tumor growth was observed.
View Figure 2
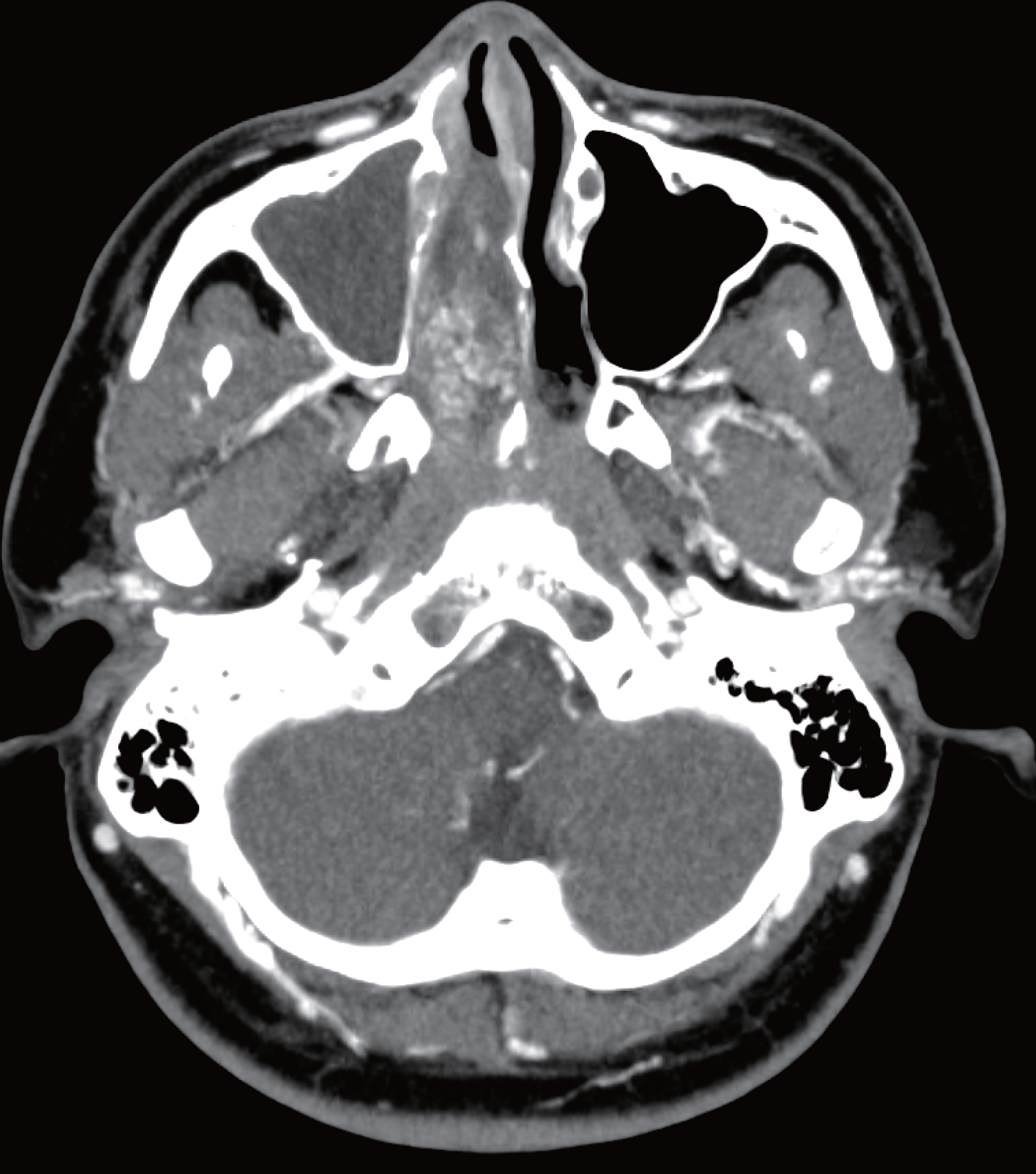 Figure 3: Contrast-enhanced CT showed strong speckled contrast effect in the left nasal cavity. The tumor can be seen enlarged to the nasopharynx.
View Figure 3
Figure 3: Contrast-enhanced CT showed strong speckled contrast effect in the left nasal cavity. The tumor can be seen enlarged to the nasopharynx.
View Figure 3
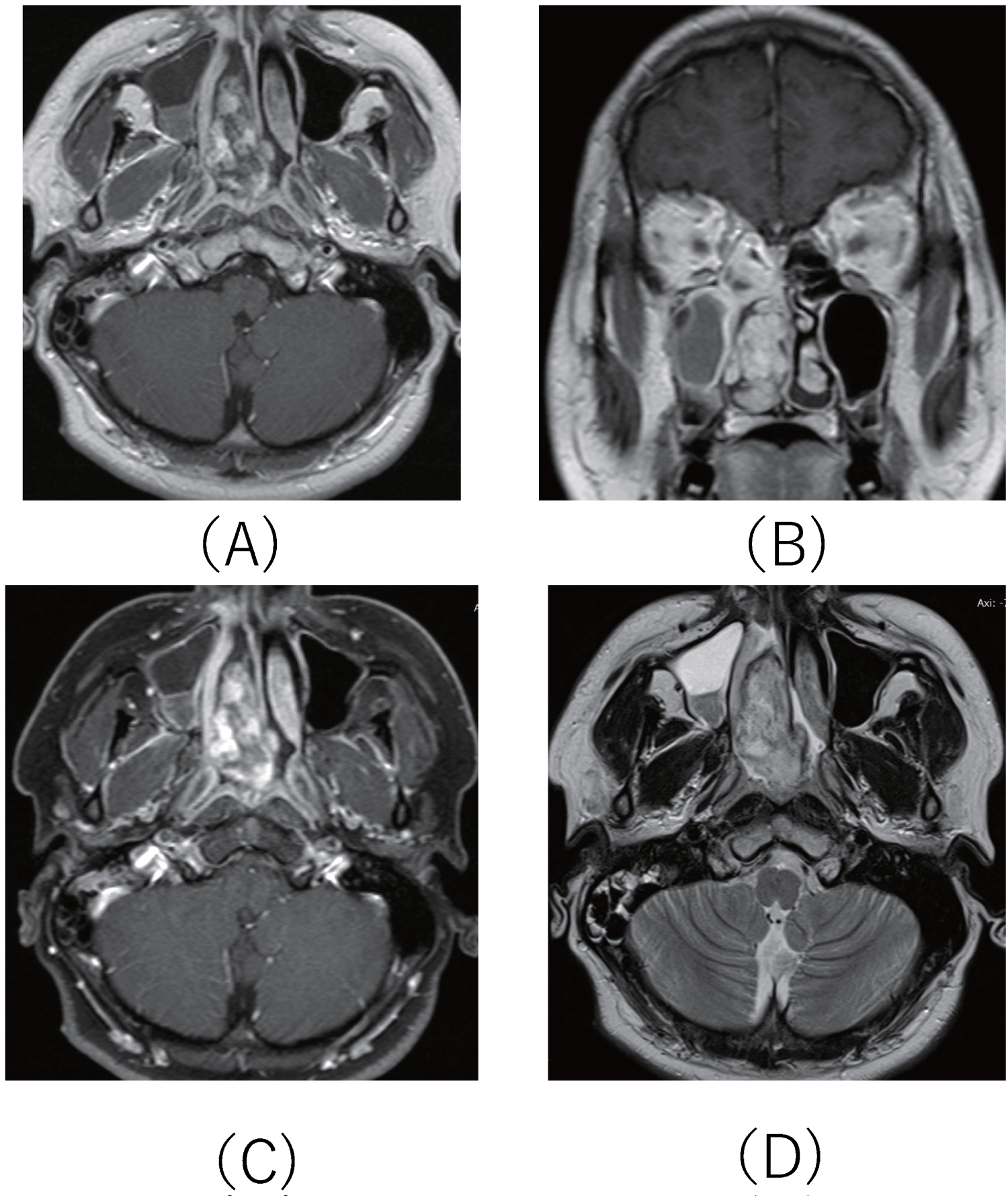 Figure 4: MRI images before surgery.
Figure 4: MRI images before surgery.
The tumor in the right nasal cavity was approximately 54 mm in size with moderately low signal intensity on T1-weighted images and uneven high signal intensity with some high signal areas on T2-weighted images. (a) T1-weighted axial image; (b) T1-weighted coronal image; (c) T1-weighted enhanced axial image; (d) T2-weighted axial image.
View Figure 4
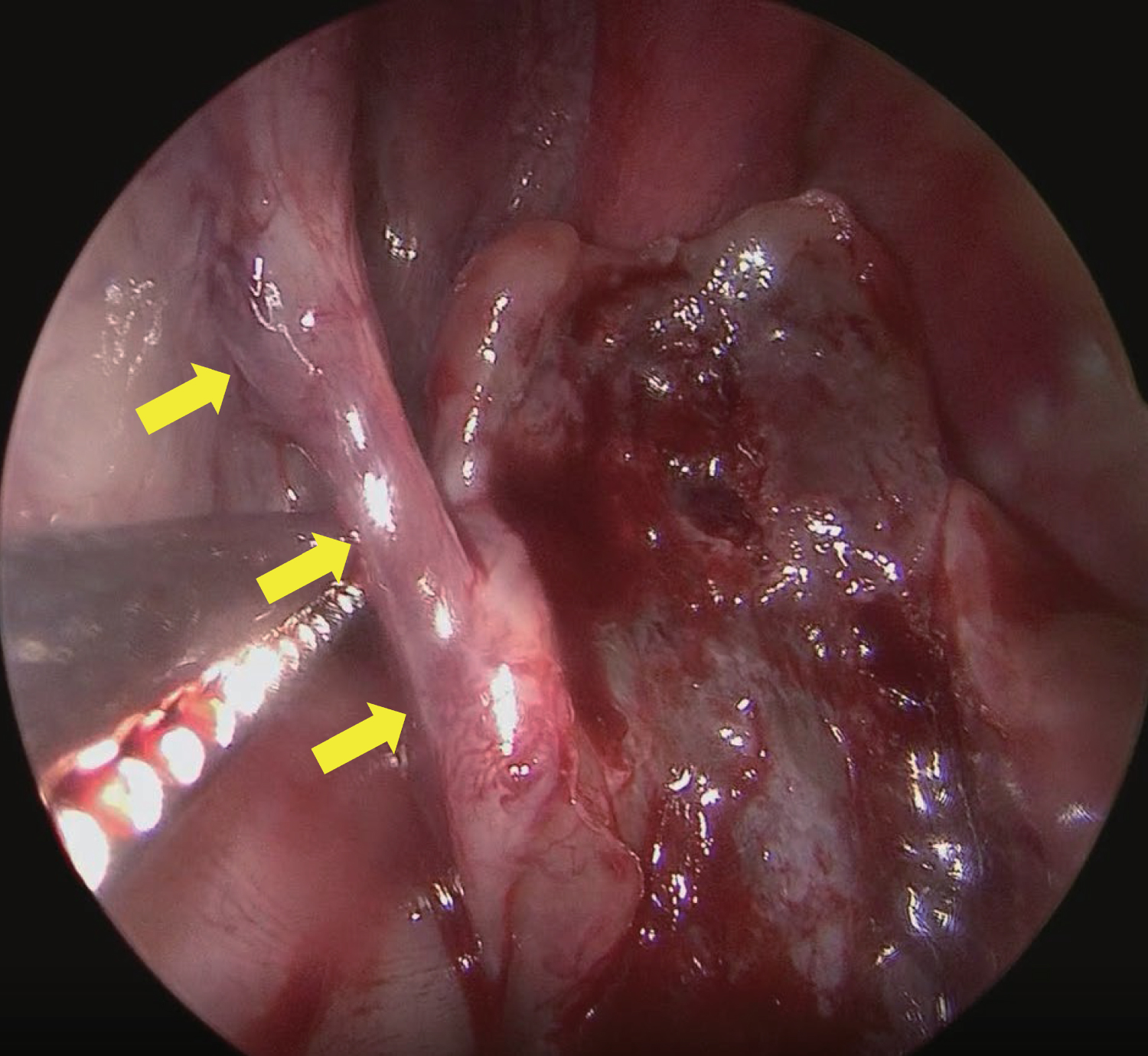 Figure 5: Operative findings. A cord flowing into the tumor from the medial mucosa of the uncinate process could be confirmed (arrow head).
View Figure 5
Figure 5: Operative findings. A cord flowing into the tumor from the medial mucosa of the uncinate process could be confirmed (arrow head).
View Figure 5
Careful observation showed that this cordate was not beating. As there were no areas of adhesion to this organized hematoma and inflow mucosa other than this cordate, this cordate was identified as the base of tumor. After ligating this cord in two places using clips (Figure 6), then excised and the remaining lesion was removed in one lump. Currently, six months have passed since this operation and there has been no bleeding and no evidence of recurrence (Figure 7).
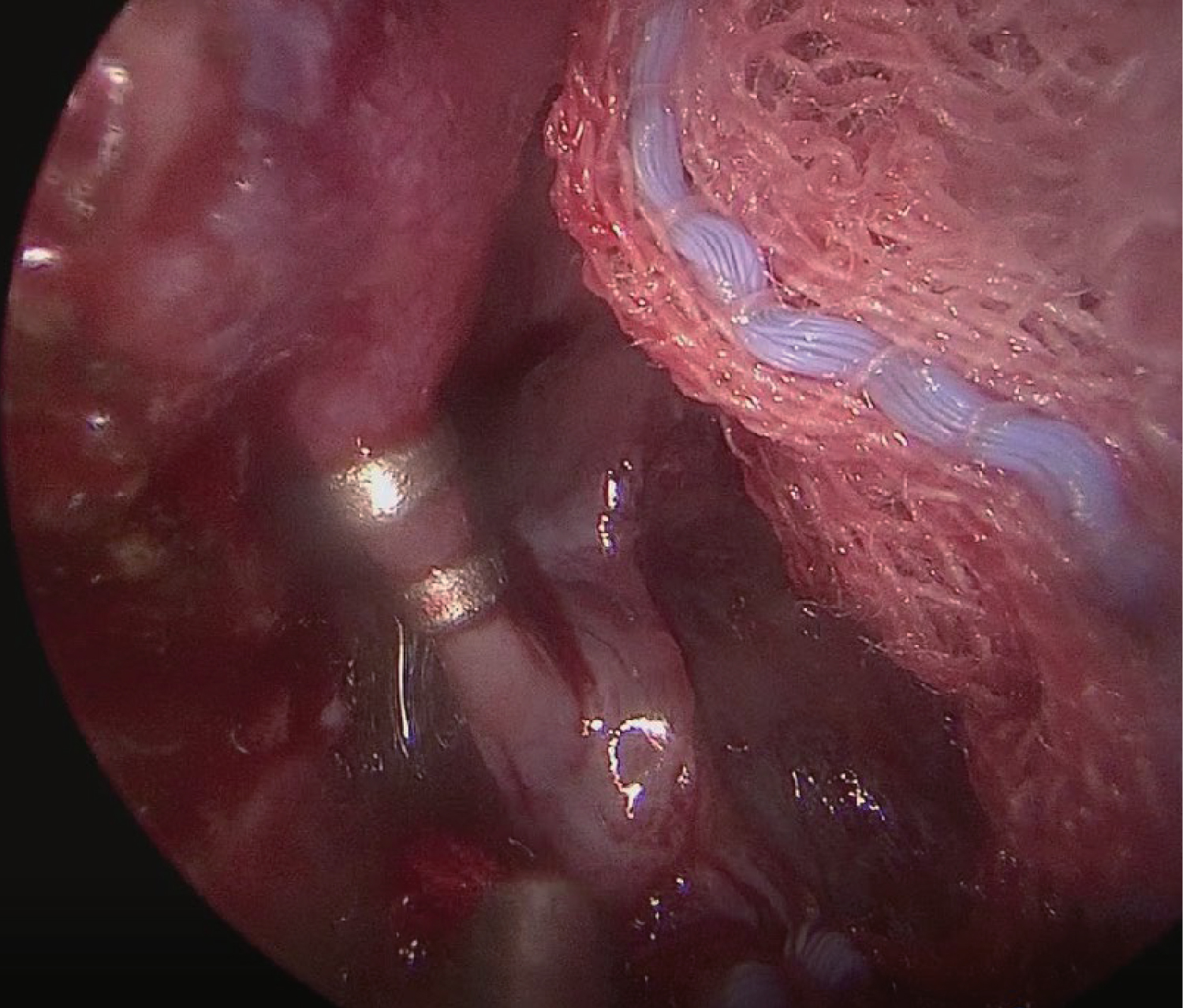 Figure 6: Operative findings. The cord presumed to be the base was detached after clipping.
View Figure 6
Figure 6: Operative findings. The cord presumed to be the base was detached after clipping.
View Figure 6
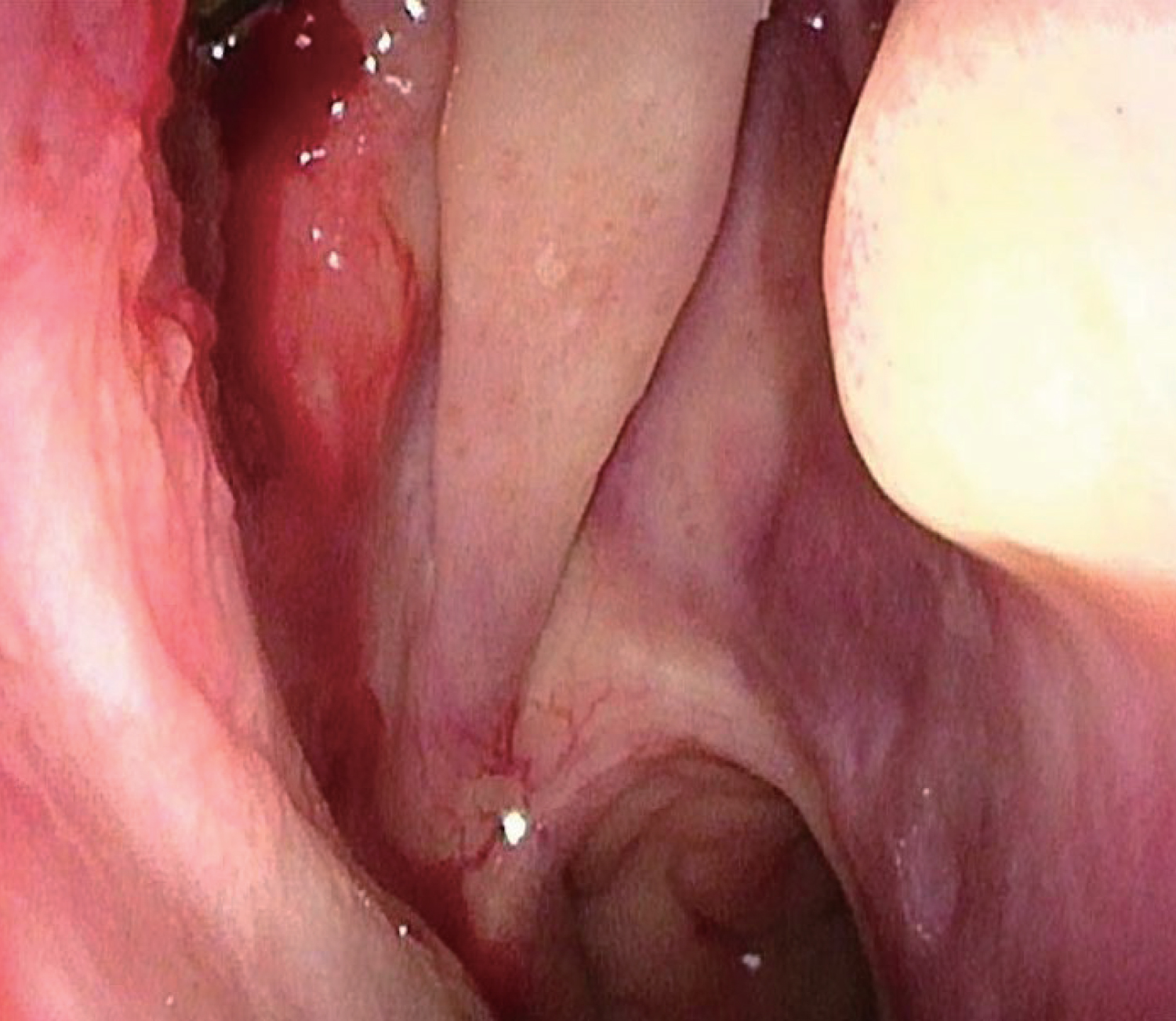 Figure 7: Endoscopic view 6 months after the surgery. There was no obvious recurrence of the organized hematoma.
View Figure 7
Figure 7: Endoscopic view 6 months after the surgery. There was no obvious recurrence of the organized hematoma.
View Figure 7
OH has been first reported by Tadokoro in 1917 [6]. More than a century has passed since the first report, but a few reports on OH have been published in the English literature. Most of the reported cases are from East Asia, particularly from Japan and South Korea [7]. The OH had been described with various other terms, such as blood boil, pseudotumor, organizing hematoma, hematoma like mass, hematoma [6,8-11]. More than a century has passed since the first report, but the exact etiology remains unclear. It is suggested that the predisposing factor of the development for OH include trauma or sinus surgery, radiation, fungal infection, bleeding diathesis, or underlying hemorrhagic lesion [8,12] . In this case, the patient was a naturally healthy young man with no such complications.
OH is known to occur more frequently in relatively younger than maxillary cancer, Song, et al. reported in the 75 cases from the literature that the mean age was 43.5 year, with an age range of 12 to 78 years [2]. Wenhui also reported in the 84 cases from the literature that the mean age was 50 year, with an age range of 9 to 81 years [5]. OH mainly originated in the maxillary sinus, few cases are confined to the intrinsic nasal cavity. Wenhui reported that 2 of 84 cases were confined to the intrinsic nasal cavity and others were maxillary sinuses. So in this case was shown to be a relatively young case, it was considered very rare in terms of occurrence location [5].
An OH is a chronic state of fibrotic tissue surrounding a hemorrhage, and the lesions are mainly composed of an OH, regardless of their origin [9]. Pathological findings include hematoma, fibrosis, neovascularization, and no evidence of malignant neoplasm. The features on paranasal sinus computed tomography are heterogeneous patchy enhancement of the lesion with post-enhancement images and enhanced lesions are located in the center or periphery of the tumor [2]. In addition, features on magnetic resonance imaging are intermediate signal intensity with scattered foci of hyperintensity on T1-weighted MR image and the lesion are more heterogeneous with a surrounding hypointense peripheral rim that corresponds to fibrous pseudocapsule on T2 weighted MR image [8,13]. OHs typically also have areas of marked irregular nodular, papillary, or frondike enhancement on both CT and MR images [8]. In this case, CT and MRI images showed features typical of OH, but the radiologist who diagnosed this patient on the images alone would have suggested the possibility of an inverted papilloma because the images showed some papillary and lobulated areas and the tumor was confined to the nasal cavity. We were able to obtain a diagnosis of organized hematoma before surgery because of the typical findings on the second pathological result. In the report of Soo, et al. 2 out of 16 cases were also considered papillomas in the initial radiological diagnosis alone [2]. In the present case, in which there was no bone destruction and the lesion was confined to the nasal cavity, a combination of biopsy and imaging studies was especially considered important to make a preoperative diagnosis.
Endoscopic nasal sinus surgery for excision of the OH was performed under general anesthesia. The treatment of organized hematoma is generally considered simple and surgical treatment is the only option [3]. Total removal under general anesthesia is necessary for radical cure. If the lesion is small and can be approached endoscopically, ESS should be chosen. On the other hand, if the lesion is big and there is advanced destruction of the surrounding bone tissue, the transmaxillary approach may be chosen. Soo et al. in their review of 75 cases reported that endoscopic removal was the most commonly conducted surgery in OH (50.7%), followed by Caldwell-luc, excision via lateral rhinotomy, and Denker approaches [2]. To decrease the intraoperative bleeding volume, embolization can be performed if found with angiography. But there are no reports discussing the need for embolization. If embolization is to be performed before surgery, the risks should be considered, and the patient should be fully informed consent and the indications discussed. In this case, because the lesion was confined to the nasal cavity and there was minimal bleeding even at the time of the second biopsy, only an endoscopic nasal surgery was performed without embolization. We could intraoperatively identify a cord flowing into the tumor from the medial mucosa of the uncinate process. Since no other areas of adhesion to the nasal cavity and cordate material were identified, this cord was confirmed as the base of the tumor. In previous systematic reviews, surgical approaches and other methods have been discussed, but none have been described with respect to the tumor base [2,5]. By finding the base and treating it appropriately, this tumor could be removed with little or no bleeding. In the case of organized hematoma that is confined to the nasal cavity, the tumor may be more easily removed if the base is carefully explored during surgery.
We treated a very rare case of organized hematoma in which the base of the tumor can be identified. Because organized hematoma may clinically simulate a malignant process, a combination of biopsy and imaging studies was especially considered important to make a preoperative diagnosis. The surgery itself for organized hematoma is simple, but it is a hemorrhagic disease, and if the base can be identified, the surgery can be performed more safely.
None.
None.
None declared.