Sinonasal undifferentiated carcinoma (SNUC) is a rare tumor which usually seen in nasal cavity and maxillary sinus. It has different clinical courses in contrast to sinonasal carcinoma and has poor prognosis. We have encountered a case of SNUC in frontal sinus which is a very rare site for SNUC to occur.
A 47-year female presented to ENT OPD with swelling over forehead of 3-month duration. She was also complaining of swelling in the right eye. On examination she was found to have a swelling over the forehead in the brow region approximately 3 × 2 cm extending from midline to the right side. Swelling was firm, had ill defined margins all around with mild tenderness to touch. It was extending inferolaterally so as to push the eyeball outward, inferiorly and laterally. However, she did not have diplopia and visual disturbances. There was no history of nasal discharge, nasal bleeding or loss of smell sensation. Endoscopic examination of nasal cavity was within normal limits. There was no history of smoking, radiation or exposure to chemicals. She did not have co morbidities such as diabetes mellitus, hypertension etc (Figure 1).
 Figure 1: (a) Preoperative (left); (b) Postoperative 1 month (right).
View Figure 1
Figure 1: (a) Preoperative (left); (b) Postoperative 1 month (right).
View Figure 1
She was advised to get routine investigations, FNAC from forehead swelling and CECT PNS done. FNAC revealed epithelial malignant neoplasm. CECT showed a heterogeneously enhancing soft tissue density epicentered in the right frontal sinus, eroding both anterior and posterior bony tables of the right frontal sinus. It was extending medially to involve the part of left side of the frontal sinus. CEMRI was done to ensure extent of intracranial extension. Fortunately, tumor was extradural, not involving frontal lobe. Considering the limited extension of tumor, decision of upfront surgery was taken by multidisciplinary tumor board (Figure 2).
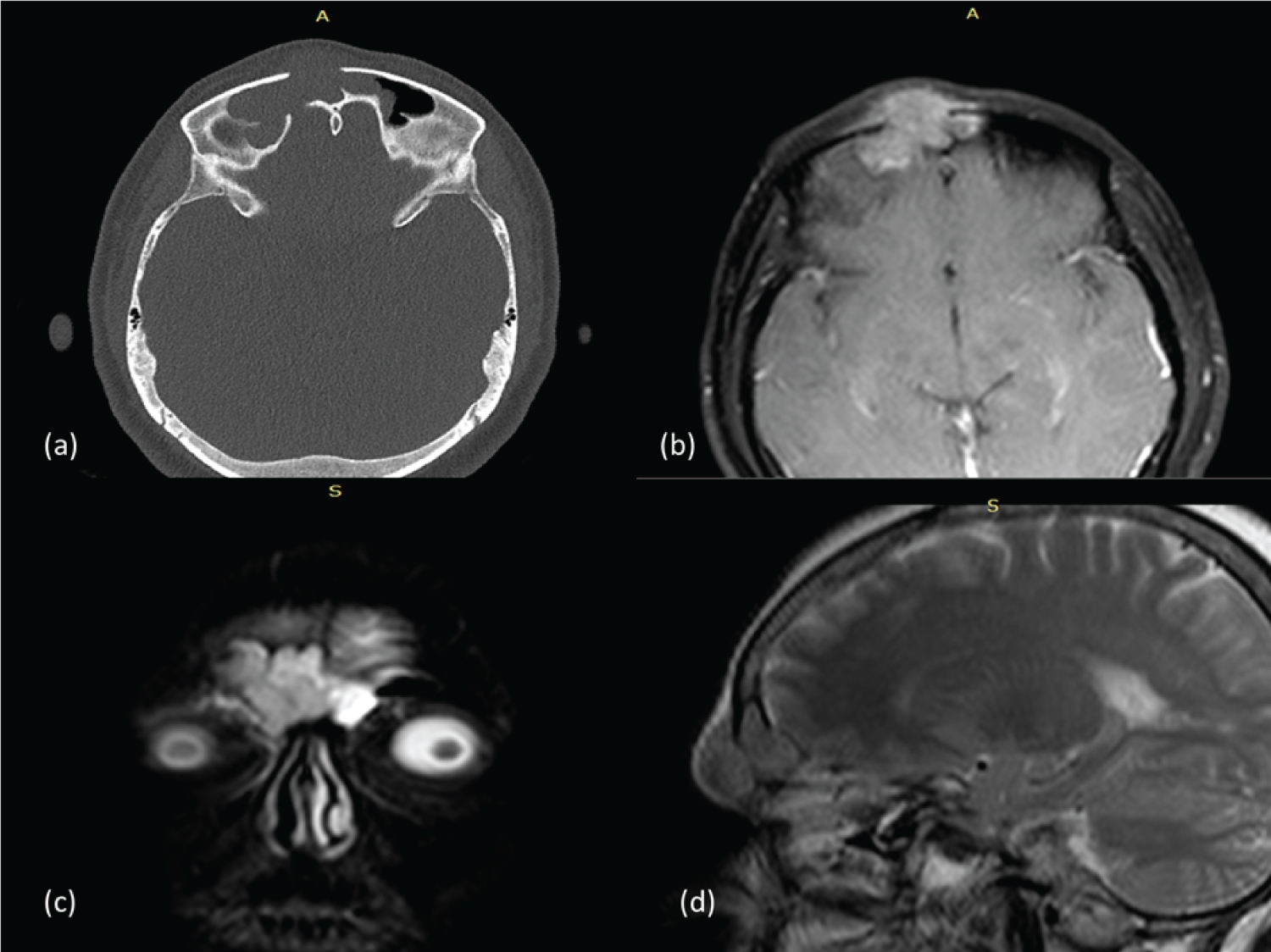 Figure 2: (a) Axial CECT bone window showing erosion of anterior and posterior table of frontal sinus; (b) Axial CEMRI T1 W showing enhancing tumor; (c) Coronal T2W MRI; (d) Saggital T2W MRI.
View Figure 2
Figure 2: (a) Axial CECT bone window showing erosion of anterior and posterior table of frontal sinus; (b) Axial CEMRI T1 W showing enhancing tumor; (c) Coronal T2W MRI; (d) Saggital T2W MRI.
View Figure 2
Patient underwent excision of tumor followed by frontal sinus obliteration (Figure 3).
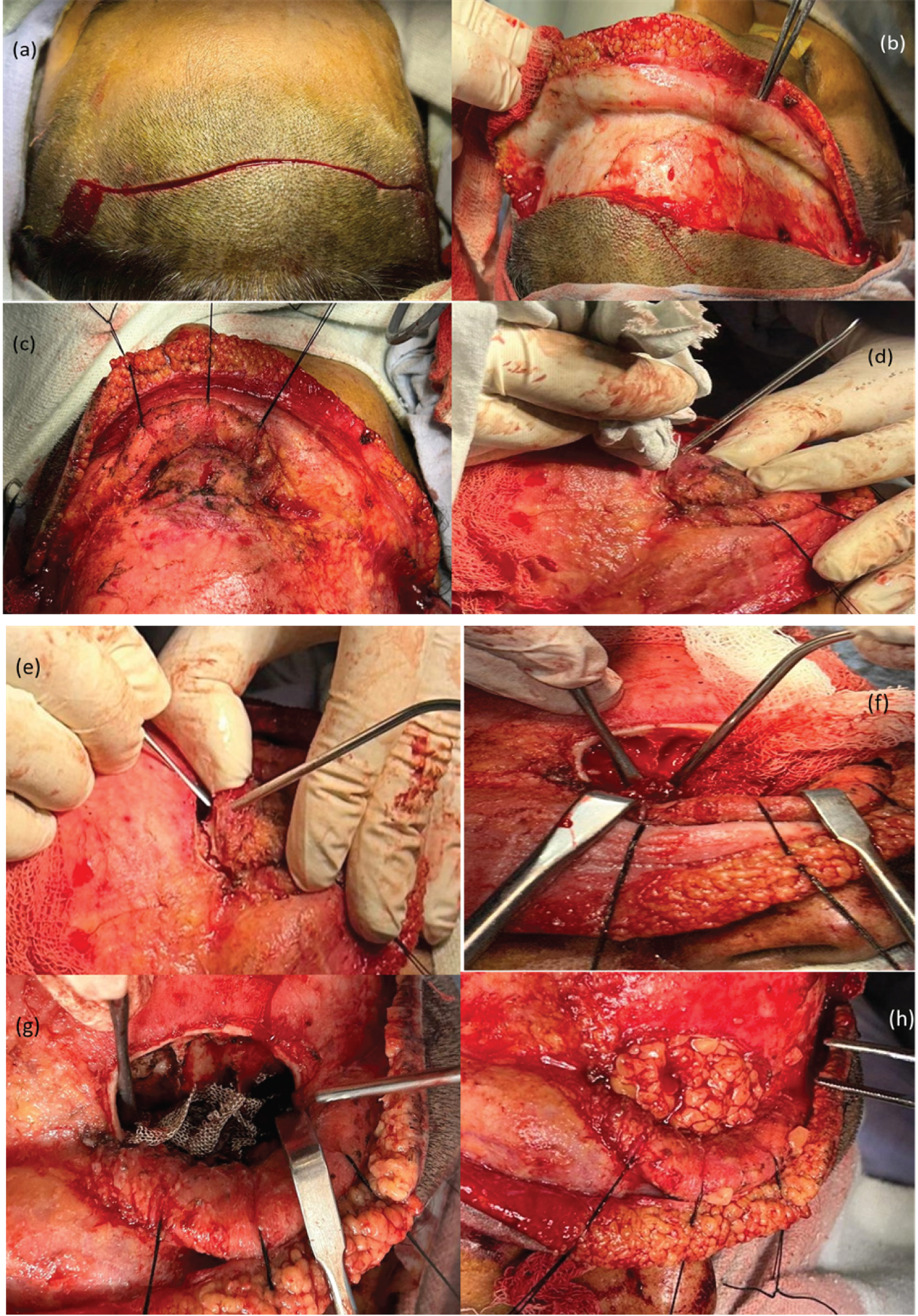 Figure 3: (a) Skin incision; (b) Subgaleal flap elevation; (c) Tumour delineation; (d) Drilling of bone with safety margin; (e) Removal of anterior bony table of frontal sinus with tumor; (f) Tumor removal from posterior wall; (g) Complete tumor removal done; (h) Fat obliteration.
View Figure 3
Figure 3: (a) Skin incision; (b) Subgaleal flap elevation; (c) Tumour delineation; (d) Drilling of bone with safety margin; (e) Removal of anterior bony table of frontal sinus with tumor; (f) Tumor removal from posterior wall; (g) Complete tumor removal done; (h) Fat obliteration.
View Figure 3
Surgical steps -
1. Bicoronal incision in the scalp skin was made few centimeters behind hair line in curvilinear fashion.
2. Skin flap was elevated in subgaleal plane till the supraorbital ridge bilaterally.
3. While raising skin flap, tumor was encountered few centimeters superior to supraorbital ridge. Galea aponeurotica (epicranial aponeurosis) was found to be involved by tumor in this region hence flap was elevated in subcutaneous plane.
4. Tumor was delineated all around. Soft tissue and bone cuts were made with oncological safe margin.
5. Growth was epicentered in the right frontal sinus, eroding the anterior table of frontal sinus, was extending medially to involve the mucosa of left frontal sinus. It was also extending inferolaterally causing erosion of roof of right orbit. However it did not involve the periorbita. There was small area of bony erosion in the posterior table of frontal sinus on the right side and growth was abutting duramater in this region, however, it was not involving the duramater or frontal lobe.
6. Tumor was removed in toto along with anterior table of frontal sinus. Left over posterior table bone was drilled to ensure complete clearance of tumor followed by frontal sinus obliteration using fascia lata and fat which was taken from right side of thigh.
On examination of H&E stained slides on 100X, sheets of undifferentiated pleomorphic malignant epithelial cells were seen. On further examination with immunohistochemistry, cells are found to have CK7 and CKAE1/AE3 positivity (Figure 4).
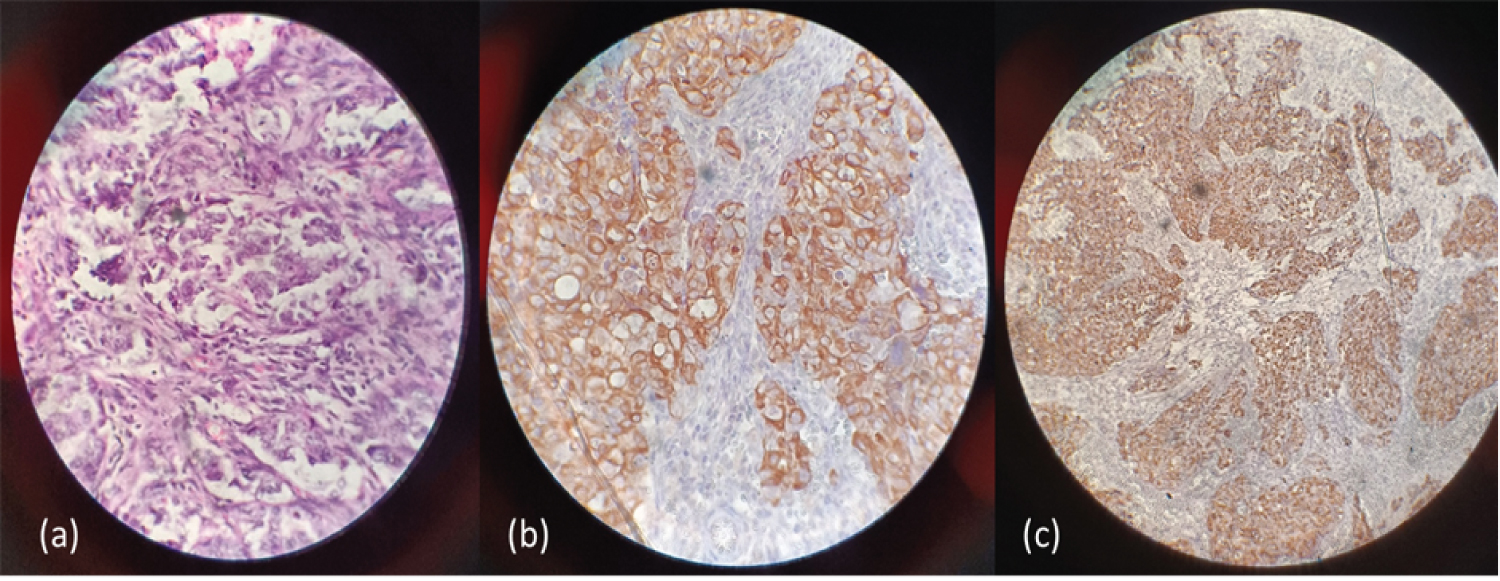 Figure 4: (a) Sheets of undifferentiated pleomorphic malignant epithelial cells on H&E 100X; (b) CK7 positivity; (c) CKAE1/CKAE3 positivity.
View Figure 4
Figure 4: (a) Sheets of undifferentiated pleomorphic malignant epithelial cells on H&E 100X; (b) CK7 positivity; (c) CKAE1/CKAE3 positivity.
View Figure 4
Sinonasal Undifferentiated carcinoma is one of the rare malignancies of paranasal sinuses. It was first described in 1986 by Frierson & colleagues based on its distinct histology, immunohistochemical profile and clinical course [1]. SNUC is clinicopathologically distinctive from other tumours but is difficult to study due to its incidence as low as 0.02 per 100000.
It arises from the Schneiderian epithelium or from the nasal ectoderm of the paranasal sinuses or the nasal cavity [2] & is thought to have a male preponderance &bimodal distribution with median age of presentation being 50 years (range 20-77 years) [3]. The exact etiology is unknown, but a history of smoking and radiation exposure is often noted.
Since it is a highly aggressive malignancy, it usually presents with advanced clinical features due to the local invasion of orbit, anterior cranial fossa, nasopharynx, sphenoid & frontal sinuses. The symptoms have a propensity to develop over a short period of time ranging from few weeks to months due to its highly aggressive nature [4]. The most common symptoms include nasal obstruction, epistaxis, proptosis, periorbital discomfort with swelling, visual impairment (due to compression of optic nerve) and cranial nerve palsies [1]. About one third of the patients present with locoregional nodal involvement and distant metastases, particularly to the lung and bone.
To diagnose SNUC, Electron microscopy & Immunohistochemistry are required; however, simple differentiation of SNUC from other undifferentiated tumours can be done on light microscopy as well. Histologically, intermediate-to-large polygonal undifferentiated cells arranged in sheets or trabeculae with large ovoid nuclei and prominent nucleoli, numerous and often aberrant mitotic figures, and vascular invasion can be seen with central necrosis. SNUCs show reactivity for Keratin, Epithelial membrane antigen, sometimes for Neuron specific enolase and CD99 also with no reactivity for chromogranin, synaptophysin, S-100 and vimentin [1]. They typically stain negative for Epstein-Barr virus unlike nasopharyngeal carcinomas.
The differential diagnosis includes Squamous cell carcinoma, Olfactory neuroblastoma, Small-cell undifferentiated neuroendocrine carcinoma, Lymphoepithelial carcinoma of the sinonasal tract, Mucosal malignant melanoma, Hematolymphoid malignancies, Rhabdomyosarcoma.
A CT scan of PNS should be done which typically shows a non calcified mass arising from nasal cavity or paranasal sinuses showing bone destruction with or without the invasion of the nearby structures like the anterior cranial fossa, orbit etc. MRI may aid in the staging of the disease as it gives a better picture of soft tissue involvement.
SNUCs are often unresectable at the time of presentation as the patients present in advanced stages owing to the locally destructive nature of the tumour. However, the disease in our case was limited to frontal sinus only; hence it was possible to remove tumour in toto. Since the complete removal of the tumour with wide margins is often not possible because of the complex anatomy of the head & neck, the treatment involves a combination of Surgery (craniofacial resection), chemotherapy & radiotherapy with the goal being control of local disease, preservation of vision and limiting significant intracranial extension. Different combinations of chemotherapy, radiotherapy, and surgical resection have been used and there is not a universal treatment strategy. Few studies have reported that surgery combined with radiotherapy, either given preoperatively or post-operatively, have the highest locoregional control while some recommend the use of induction chemotherapy followed by concurrent chemoradiation as the primary treatment. The chemotherapeutic agents often used are cyclophosphamide, doxorubicin, vincristine, etoposide, cisplatin & 5-flourouracil [5,6].
The prognosis associated with SNUC is poor, and death often occurs within a short span of time following the diagnosis. In the original report by Frierson, et al. the median survival was only 4 months in patients of SNUC treated with radiotherapy alone. Improved survival (median 53.6 months) results for SNUC were reported by Deutsch, et al. by using aggressive multimodality approach [7]. Since then, there has been a trend towards improvement in survival of the patients owing to proper management [5,6]. Despite the advances, the cure rate for SNUC remains low, recurrence rate is very high and many patients die of disease within months of diagnosis [8].
No funding.
No conflict of interest.