Objectives: Infants born with giant head and neck (HN) masses can experience deficits in feeding-swallowing function in early infancy. This study aims to characterize the feeding-swallowing patterns of these infants and highlight trends in this unique population.
Methods: This is a retrospective chart review of infants with giant HN masses born via EXIT (Ex Utero Intrapartum Treatment) procedure who received speech pathology services for feeding and swallowing between 2009 and 2019 at a tertiary children’s hospital. Primary diagnoses included both teratoma and lymphatic malformation. Demographic data, surgical data, and speech pathology findings including clinical swallow evaluations (CSE) and video fluoroscopic swallow studies (VFSS) were collected and analyzed.
Results: 5 patients were identified. 60% of patients were female, gestational age at birth ranged from 29 weeks to 37 weeks and the average age at the time of initial clinical swallow evaluation was 9.4 weeks (range: 2 weeks to 6 months). The majority of the patients were noted to demonstrate feeding deficits based on findings from first clinical swallow evaluation with deficits in latch (100%), suck coordination (100%) and suck-swallow ratio (60%). 100% of patients presented with some degree of oropharyngeal dysphagia based on VFSS findings. 40% of patients exhibited laryngeal penetration in isolation, and 40% of patients exhibited tracheal aspiration. At initial swallow study, 100% of aspiration events were “silent,” without a triggered cough response or clearance of aspirated material from the airway. Of the two patients with aspiration, repeat VFSS noted resolution in one patient and persistent aspiration in the other. All patients included in this study were discharged home either with a nasogastric tube or gastrostomy tube as a supplement to oral feeding.
Conclusion: The results of this case series emphasize the importance of timely and comprehensive feeding-swallowing assessment and intervention for infants with giant airway masses. The vast majority of the infants in this study demonstrated some degree of oral-pharyngeal dysphagia, but with consistent and targeted intervention, they were able to initiate oral intake, eliminate use of a feeding tube over time, and ultimately achieve a regular (unmodified) diet relative to peers.
Giant head and neck mass, Teratoma, Lymphatic malformation, Videofluoroscopic swallow study, Pediatric dysphagia, Infant swallowing, Infant feeding
Advances in fetal imaging have resulted in the identification of congenital head and neck (HN) masses prenatally [1]. Giant fetal HN masses, typically either teratomas or lymphatic malformations, are often deemed or suspected to be life-threatening during delivery [2]. In many of these cases, the airway can become distorted or obstructed leading to polyhydramnios in utero , and respiratory distress or apnea after birth [3]. In these cases, an ex-utero intrapartum treatment procedure (EXIT) is utilized for safe delivery of these infants [2]. To date, there has been published data on medical-surgical management of giant masses [2,4,5]; however, minimal to no data regarding swallowing abilities and outcomes has been published on this unique population.
Feeding-swallowing is a complex task requiring infants to coordinate sucking, swallowing, and breathing. Giant HN masses, by the nature of their location, place infants at high risk for feeding-swallowing difficulties. Theoretically, large masses affecting the oral cavity can potentially inhibit intrauterine swallowing, thus resulting in less swallowing “practice” prenatally. Additionally, structural differences of the head/neck caused by the mass such as cleft palate or jaw immobility can also negatively impact feeding success following birth [6]. Lastly, the possibility of continued post-natal airway instability particularly for the demands of feeding and/or the presence of a tracheostomy tube can also influence feeding outcomes. To the best of our knowledge, this series is the first to exclusively focus on feeding-swallowing trends in infants born with giant HN masses necessitating EXIT procedure for safe delivery. The purpose of this study is threefold: 1) Document results and timeliness of clinical swallow evaluations, 2) Describe swallow physiology deficits on VFSS and subsequent interventions, and 3) Detail feeding-swallowing outcomes in this distinct group of infants.
With approval from the institutional review board, a retrospective chart review of infants born via EXIT procedure due to giant HN masses and who also received speech pathology services from 2009 to 2019 at a tertiary children’s hospital was completed. A total of 5 infants met the criteria. Data captured included: Gender, diagnosis, airway status, surgical history, presence of nasogastric tube, presence of gastrostomy tube, and details on feeding-swallowing findings including clinical swallow evaluation and videofluoroscopic swallow study (VFSS) results. Qualitative results were compiled to highlight the infant’s feeding-swallowing assessment and feeding outcomes.
Clinical swallow evaluations (CSE) were completed by speech-language pathologists. Information gathered included: Age at initial CSE, mode of nutrition, presence of respiratory support, and descriptive oral-pharyngeal swallow findings. VFSS was performed by a certified pediatric speech-language pathologist and a pediatric radiologist. If a patient had more than one VFSS completed, data from the first and the last exam were reported. Varibar products were utilized. Half nectar (slightly thick) was achieved by mixing 50% Varibar thin liquid barium and 50% Varibar nectar barium. Data from the VFSS reports were separated into two categories: Oral phase and pharyngeal phase. The oral phase included documentation of the following components: (1) Latch (2) Suck-swallow-breathe coordination (3) Suck-swallow ratio (4) Bolus formation and (5) Oral residue. Pharyngeal phase components included: (1) Velo- pharyngeal closure/pharyngonasal reflux (2) Level of initiation of swallow response (3) Tongue base retraction and (4) Pharyngeal residue. The infants were classified as demonstrating oral phase dysphagia and/or pharyngeal phase dysphagia if at least one abnormal component was identified (see Table 1). Information on laryngeal penetration and tracheal aspiration was also extracted from reports, including Penetration- Aspiration Scale (PAS) score [7]. Interventions attempted during the exam were also cataloged. Lastly, each patient was given a Functional Oral Intake Scale-Suckle Feeds and Transitional Feeds (FOIS) score, determined by a pediatric SLP retrospectively based on notes from medical chart review [8].
Table 1: Definitions of Oral and Pharyngeal Phase Components [9]. View Table 1
Five patients were identified who met the criteria (refer to Table 2 for demographic information). 40% of patients received a tracheostomy, with one receiving tracheostomy at the time of birth and the other patient receiving a tracheostomy at 3 months of age. Mass removal was performed in all patients, with a mean age at removal of 32.2 days. Other surgical procedures included GT placement (n = 4), cleft palate repair (n = 2), epiglottopexy (n = 1), and supraglottoplasty (n = 1). The age at initial clinical swallow evaluation varied from 2 weeks of age to 6 months of age. 40% of patients were tracheostomy/ventilator-dependent at the time of initial evaluation, 20% required 0.5L at 21% FiO 2 via nasal cannula, and 40% required no supplemental oxygen support. At the initial SLP evaluation, 40% of patients were already consuming some degree of oral intake, while the other 60% were NPO pending SLP evaluation. The mean age at the time of initial VFSS was 2.86 months, ranging from < 1 month to 8-months-old. 80% of patients received at least two VFSS. The mean age at final VFSS exam was 6.75 months (range 4 to 13 months).
Table 2: Summary of patient data. View Table 2
Mean age at initial SLP clinical evaluation was 9.4 weeks (range 2 weeks to 6 months). 100% of patients demonstrated oral phase deficits. Specifically, all patients demonstrated impaired latch to a bottle nipple and impaired suck-swallow-breathe (SSB) coordination. 40% of patients were judged to have a normal suck-to-swallow ratio whereas the other 60% exhibited impaired suck-to-swallow ratio. All patients were observed to have “stress cues” during the initial clinical feeding and swallowing assessment. “Stress cues” were defined as exhibiting any of the following: Brow-Raising, audible gulping/hard swallows, finger splaying, hiccups, and change to behavioral state. Physiologic changes from baseline, identified as respiratory rate, heart rate, or oxygenation outside of parameters set by the medical team, were noted in 40% of patients (n = 2) with both patients exhibiting tachypnea. With regard to concern for pharyngeal phase impairments, pharyngeal “congestion” or “wetness” was not observed in any patients, and overt coughing was only observed in one patient.
Following clinical evaluation, all patients were evaluated via videofluoroscopy. FOIS score at the time of exam for 80% of patients was documented as a “2” (inconsistent or minimal oral intake and still dependent on a supplemental feeding system). This indicated that the patient was only consuming some degree of oral feeding in the context of therapy sessions with speech pathology. 20% scored a “3,” indicating more consistent oral intake (being offered multiple oral feeds per day with nursing staff and/or family but still requiring supplemental nutrition). 100% of patients exhibited some degree of oral phase dysphagia. As seen on clinical evaluation, all patients demonstrated an impaired latch on VFSS; however, suck-swallow-breathe coordination was only judged to be impaired in 40% of patients (not reported in one patient) versus all patients on clinical exam. Suck to swallow ratio was impaired in 40% of patients, normal in 40% of patients, and not applicable in one patient (20%) due to use of a syringe for bolus delivery of thin liquids instead of a bottle. This subject did not demonstrate adequate oral motor skills to consume liquids from a bottle for the exam. Bolus formation was impaired for all patients, and all patients demonstrated oral residue. 100% of patients demonstrated some degree of pharyngeal phase dysphagia. Onset of the pharyngeal swallow response occurred at the level of the pyriform sinuses for all patients. Tongue base retraction was incomplete in 60% of patients, and presence of pharyngeal residue was observed in 80% of patients. Of patients who exhibited pharyngeal residue, 50% were noted to have residue on the tongue base, 50% in the valleculae, and 75% in the pyriform sinuses. Specific location of pharyngeal residue was not reported in one patient. All 5 patients were assessed with thin liquid, and 40% exhibited aspiration of thin liquid with a penetration-aspiration scale (PAS) score of 8, indicating “silent aspiration” for all the patients that aspirated. Of the 60% of patients who did not demonstrate aspiration, 66% were observed to have “deep” laryngeal penetration reaching the vocal folds, or a PAS score of “4,” and were judged to be at high risk for aspiration without certain modifications/interventions.
Pharyngonasal backflow was observed in 40% of patients due to the presence of a cleft palate. All patients with intact palatal structure exhibited functional velopharyngeal closure with no pharyngonasal backflow. Interventions assessed under fluoroscopy included the following: Change of nipple flow rate, change of manner of intake (syringe vs bottle), change in viscosity, facilitation of dry swallows with use of a pacifier, and small/controlled bolus size (via delivering specific volume by syringe). 40% of patients were evaluated with use of thickened liquids as an intervention strategy under fluoroscopy. This was not judged to be an effective treatment strategy for improved airway protection in any subject, as PAS score remained the same between thin and thickened liquids, and thickened liquids were not recommended as an alternative to thin liquids in any of the patients. Dry swallows facilitated with non-nutritive sucking on a pacifier were attempted in 40% of patients and judged to be effective (with clearance of pharyngeal residue observed and subjectively decreased risk of aspiration) in 100% of subjects who received this intervention. Smaller bolus size, whether achieved by use of a slower flowing nipple or delivering small, controlled bolus size via syringe, was judged to be an effective treatment strategy in 100% of patients who were offered this intervention.
FOIS score at the time of the final exam was a “2” for 25% of patients and a “3” for the other 75%. 20% (n = 1) exhibited a decrease in oral intake following the results of the first videofluoroscopic swallow study, while 80% (n = 4) of patients demonstrated an ability to advance oral intake following completion of the first exam. Oral phase deficits persisted in 100% of patients who were evaluated by repeat fluoroscopy. Latch was impaired in 75% of patients, SSB coordination in 50% (not documented in one patient), SSR in 50%. Impairment in bolus formation and in oral residue was observed in 100% of patients. Pharyngeal phase deficits also persisted to some degree in 100% of patients; however, overall airway protection was improved from first videofluoroscopic swallow study to the last. The majority of patients continued to demonstrate onset of the pharyngeal swallow at the pyriform sinuses with only one patient triggering a swallow consistently in the valleculae. Tongue base retraction was incomplete in 75% of patients. Pharyngeal residue was noted in 100% of patients. Laryngeal penetration was observed in 50% of patients. Tracheal aspiration only persisted in 25% (n = 1) of patients with continued silent aspiration of thin liquid observed. Pharyngonasal backflow continued to be observed in the patient who had an unrepaired cleft palate, but velopharyngeal closure was functional in all other patients with no pharyngonasal backflow observed.
All patients discharged from the NICU with supplemental tube feeds, with 80% receiving gastrostomy tube placement and 20% discharging with a nasogastric tube. 80% of patients discharged with a combination of oral feeds and supplemental tube feeds, with only one patient discharging solely with tube feeding. Based on a review of the electronic medical record in 2020, 80% of patients in this cohort have had their GT or NGT removed due to the ability to safely and efficiently consume full nutrition and hydration by mouth. The average age of elimination of the supplemental feeding system was 14.25 months (range 10 months to 18 months).
This study detailed primary characteristics of oropharyngeal dysphagia seen within the population and showcased the effects of subsequent dysphagia treatment performed by Speech-Language Pathologist while highlighting the clinical importance of progression from initial clinical swallow evaluation (CSE) to instrumental evaluation (VFSS). There was some degree of variability in the age at which infants underwent their first CSE, ranging from 2 weeks to 6 months. This was likely influenced by each patient’s medical status and hospital course, including surgery. As expected, completion of CSE identified feeding stress cues such as gulping, finger splaying, and changes in state. Given some degree of airway instability, these findings were anticipated and reinforce the need for comprehensive swallowing assessment not only to begin oral feeding early, but also to alleviate feeding stress cues in order to obtain optimal feeding outcomes.
Due to the significant airway/structural anomalies, VFSS were completed on all infants. Oral swallow physiology deficits were noted and expected given anatomy alterations caused by the masses. Deficits such as reduced latch, reduced suck- swallow-breathe coordination, residue, and reduced bolus formation all align with infants with either oral anatomy alteration or breathing inefficiencies. Improvements in oral phase deficits were noted between first and last swallow study for most of the patients, which can be attributed to patient-tailored therapy and therapeutic feeding practice.
Deficits in pharyngeal swallow physiology included boluses reaching the pyriform sinuses prior to onset of the swallow, reduced tongue base retraction, and pharyngeal residue. Again, given that masses previously occupied the oropharnyx or cervical region, alterations in pharyngeal sensorimotor function were to be expected, and likely account for the deficits noted. Regarding airway protection, the vast majority were able to protect their airway in a functional manner despite the presence of oral and pharyngeal phase deficits. Overall airway protection was improved from the time of initial VFSS to the last. It is hypothesized that improvement stemmed from consistent and targeted intervention. Another notable finding of this case series is that all patients had persistent oropharyngeal dysphagia from first to last instrumental evaluation; however, despite these deficits, patients were functional with improvement seen in progression towards age-appropriate oral diet, with reduced reliance on supplemental forms of feeding. All patients, except for one, showed an increase in their FOIS scores over time which reflected the gradual improvement in overall intake due to improvement in skills with guided practice and appropriate interventions. Also of note, the presence of gastrostomy tube remained in one patient due to oral phase deficits which limited the patient's efficiency and volume of intake without concern for swallow safety or pharyngeal phase impairments.
The primary limitations of this study include limitations common to retrospective analysis and a small patient population, as it is difficult to draw definitive conclusions from a case series. Given the retrospective nature, some data pieces were missing; therefore, interpretation was performed from the information provided via chart review.
All patients in this study demonstrated evidence of dysphagia in both oral and pharyngeal phases of swallowing; however, with consistent and targeted intervention, all were able to initiate oral intake, eliminate use of supplemental nutrition over time, and ultimately intake a regular, unmodified diet relative to peers. Facilitation of early speech intervention was a direct byproduct of the collaborative dyad between speech pathology and otolaryngology which is critical for patient care and favorable outcomes. While limited in nature, the findings of this case series may be applied to future patients with large head-neck masses (Figure 1, Figure 2 and Figure 3) within the aerodigestive tract and serve as a launching pad for future research.
 Figure 1: Infant with large neck mass.
View Figure 1
Figure 1: Infant with large neck mass.
View Figure 1
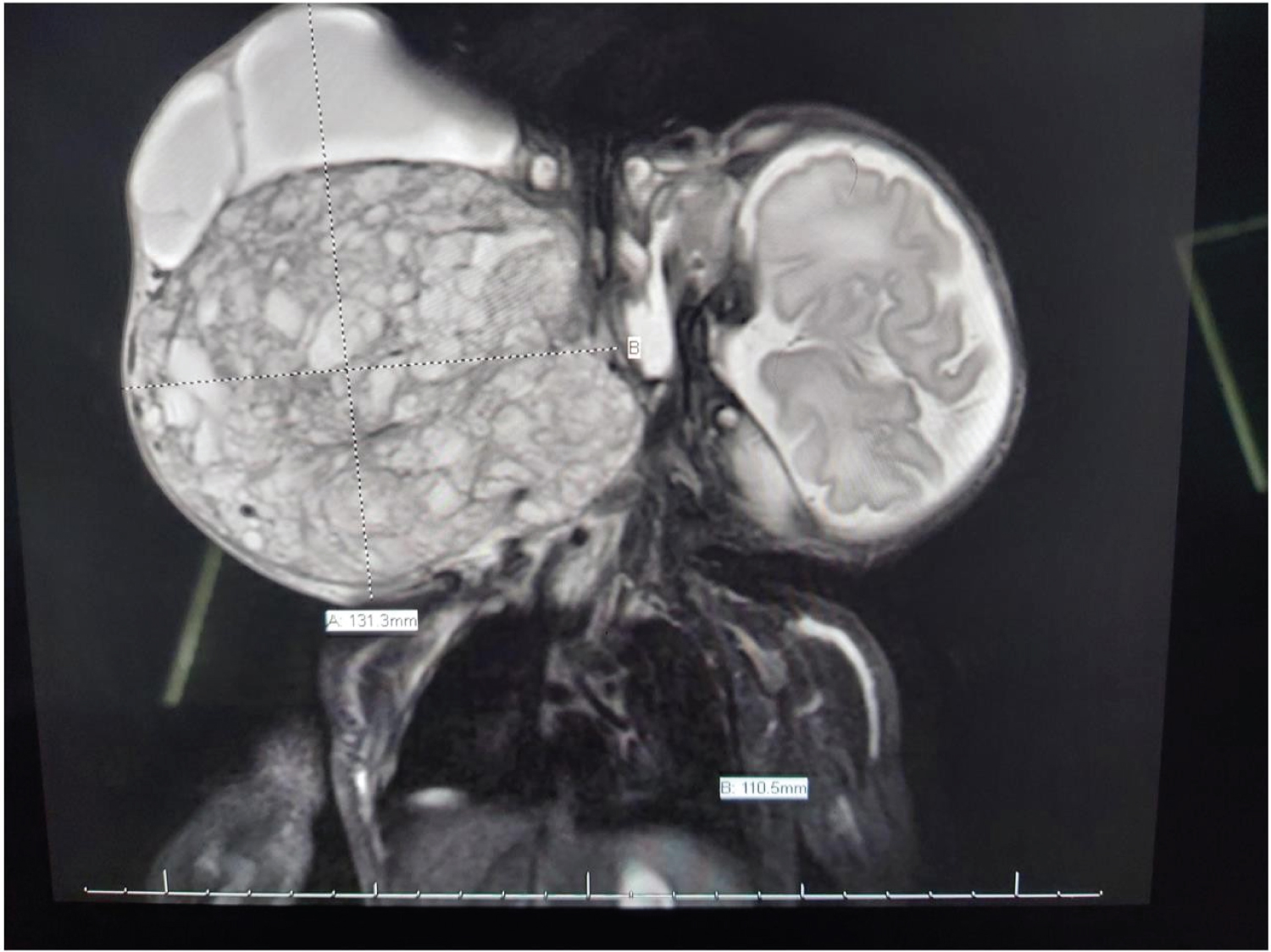 Figure 2: Radiographic image of infant with large neck mass.
View Figure 2
Figure 2: Radiographic image of infant with large neck mass.
View Figure 2
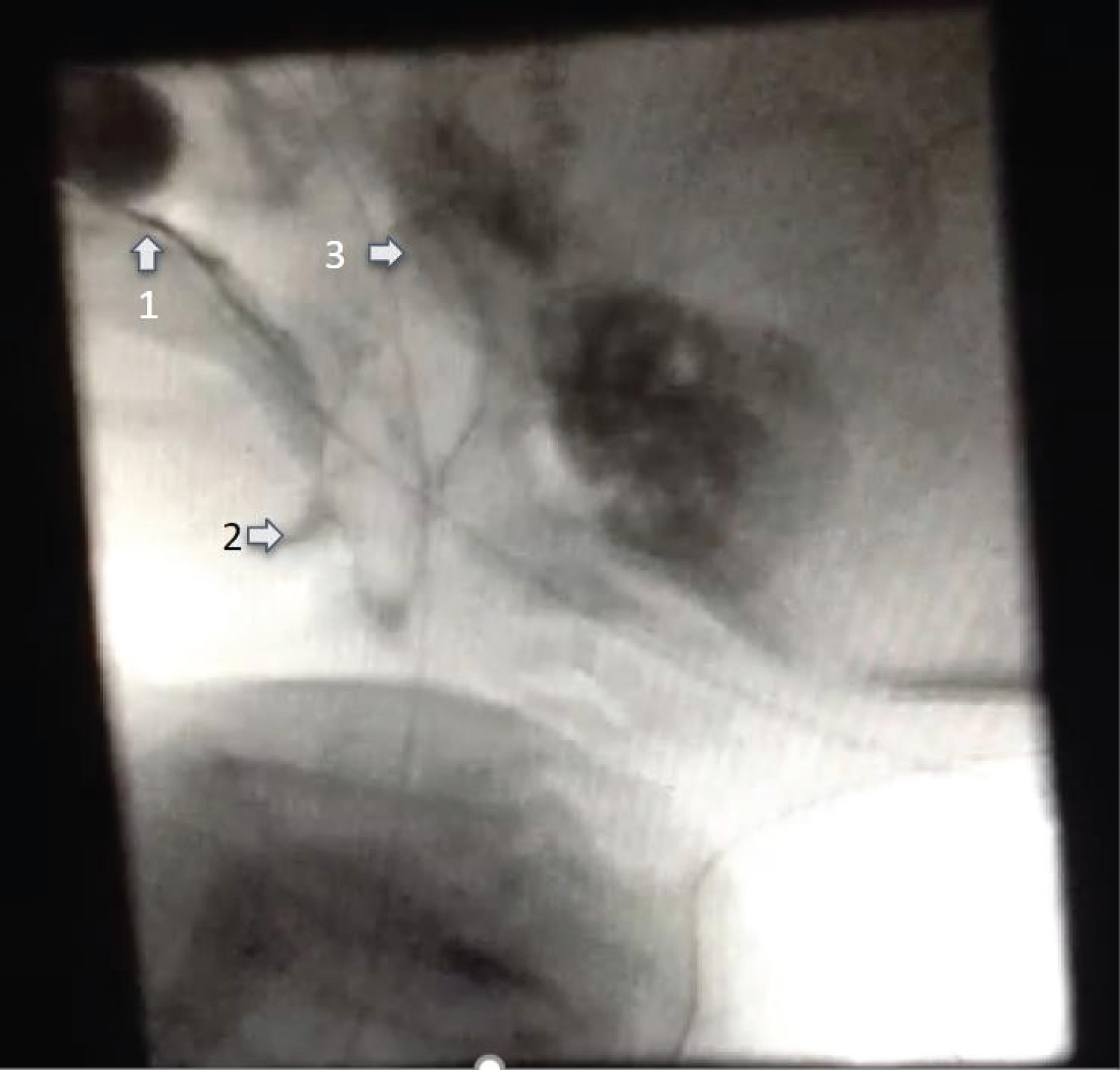 Figure 3: VFSS in a patient with large neck mass: (1) oral residue; (2) pharyngeal residue; (3) pharyngonasal regurgitation.
View Figure 3
Figure 3: VFSS in a patient with large neck mass: (1) oral residue; (2) pharyngeal residue; (3) pharyngonasal regurgitation.
View Figure 3
The authors have no funding, financial relationships, or conflicts of interest to disclose.