Background: The increasing global prevalence of overweight and obese adults underscored the importance of evidence-based practices within primary care clinics to confront this enduring health issue. One such approach, the 5As model (Ask, Assess, Advise, Agree, Assist), was widely adopted in primary care settings, providing healthcare providers with a systematic approach to facilitate behavioral changes conducive to healthier weight management behaviors and lifestyles.
Methods: The 5As model impact was assessed using a paired data measurement strategy, which involved pre- and post-implementation assessments. These assessments measured patient-reported weight management behaviors using the Weight Control Strategies Scale (WCSS) survey and Body Mass Index (BMI) scores. Data collection spanned three months and included repeated measurements at two separate time intervals.
Results: All data was analyzed using the Statistical Package for the Social Sciences (SPSS) software for a statistical comparison. The pre- and post-intervention data assessments were depicted using percentages, medians, interquartile ranges (IQR), and the Wilcoxon signed-rank test. Findings confirmed the measures' reliability and demonstrated the intervention's positive impact, showing the effectiveness of the 5As model in improving weight management behaviors, reducing BMI scores, and enhancing patient-provider outcomes in the primary care clinic (PCC).
Conclusions: The project enhanced obesity prevention and management care in the primary care clinic (PCC) by implementing the 5As model, resulting in notable improvements in WCSS scores and reduced BMI scores. It demonstrated how the implementation of the 5As model improved patient outcomes and enhanced healthcare provider skills in preventing and managing obesity.
Body Mass index, Obesity, Overweight, Primary care, The 5As model, Patient-reported Weight management behaviors, Evidence-based practice, Weight control strategies scale survey
DNP: Doctor of Nursing Practice; EHR: Electronic Health Record; PCC: Primary Care Clinic; BMI: Body Mass Index; HCP: Healthcare Provider; WCSS: Weight Control Strategies Scale; IQR: Interquartile range; SPSS: Statistical Package for the Social Sciences
The global rise in obesity reached critical levels, with projections suggesting that by 2025, approximately 2.7 billion adults would be overweight, and 1 billion would be classified as obese [1]. This widespread prevalence presented an unprecedented public health challenge, emphasizing the urgent need for effective evidence-based practices. Recognizing obesity as a chronic condition amenable to prevention and reversal, highlighted the crucial role of primary care providers in its proficient management [2]. In this context, integrating evidence-based practices became pivotal, empowering healthcare providers to deliver comprehensive weight management counseling and promote health-conscious weight management behaviors within primary care settings.
The 5As model (Ask, Assess, Advise, Agree, Assist) provided primary care providers with a systematic and evidence-based approach to address obesity through behavior change (Refer to Figure 1). This model had the potential to positively impact patient-reported weight management behaviors and body mass index (BMI) scores. Its adoption equipped healthcare providers with enhanced capabilities to initiate weight management services within primary care settings. Recognizing its efficacy, the United States Preventive Services Task Force endorsed the 5As model as a behavioral counseling paradigm for addressing obesity in outpatient settings. Healthcare providers utilized the 5As model to guide behavioral changes among adult patients contending with overweight or obesity, facilitating a comprehensive approach that included swift weight assessment, provision of weight management counseling, and the development of an effective, personalized weight management plan.
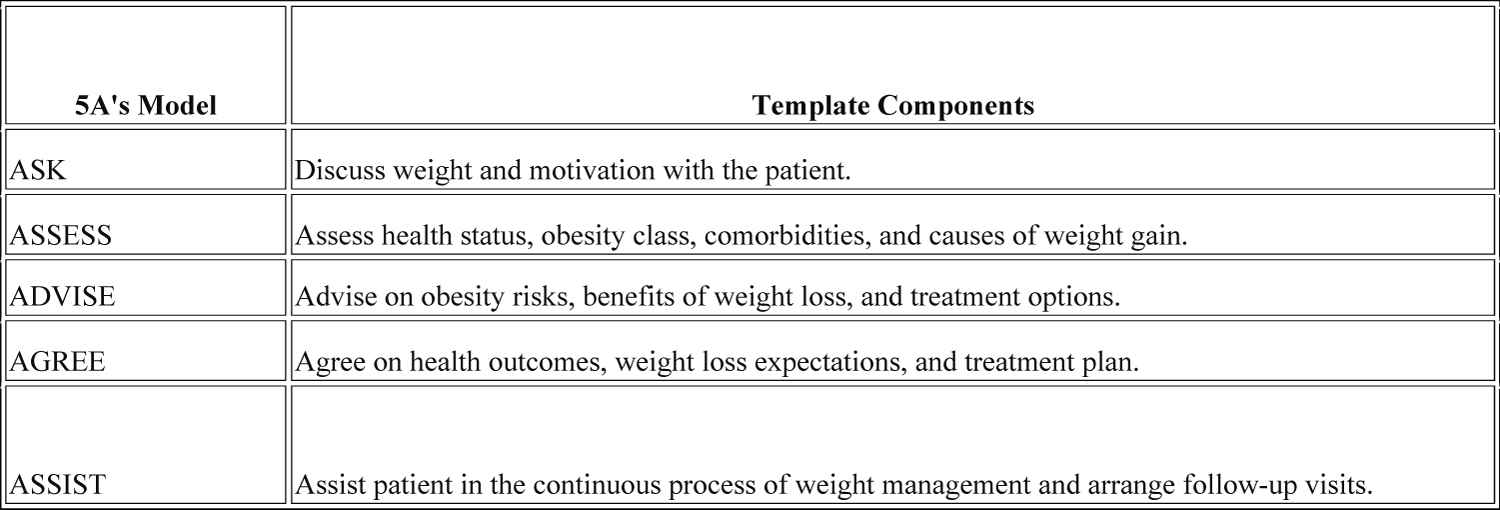 Figure 1: The 5As Model Template (Ask, Assess, Advise, Agree, Assist).
View Figure 1
Figure 1: The 5As Model Template (Ask, Assess, Advise, Agree, Assist).
View Figure 1
Effectively supporting obese adult patients within primary care settings requires HCPs to deepen their understanding of the application of the 5As model. Rooted in a synthesis of theory and evidence-based practices, the 5As model empowered primary care providers to actively assist patients in realizing their weight loss goals [3]. Primary care practices that had embraced the 5As model reported a noteworthy twofold increase in weight management success rates, with follow-up and coordination efforts tailored to each patient's specific needs [4]. These literature perspectives aligned with the principles of the 5As model, emphasizing the importance of asking about obesity-related factors, assessing the individual's condition comprehensively, advising on appropriate interventions, reaching an agreement on the treatment plan, and arranging follow-up to address obesity within primary care settings.
The aim of the project was to improve obesity prevention and management care within a primary care clinic (PCC) through the implementation of the 5As model. The objectives involved improving the capabilities of the HCP in evaluating, advising, managing, and treating adult patients with overweight or obesity. The project successfully elevated the proficiency of the HCP, particularly in conducting obesity screening and delivering comprehensive weight management counselling to patients with excess weight. Concurrently, it led to direct benefits to overweight or obese adult patients, resulting in improvements in their patient-reported weight management behaviours and corresponding reductions in BMI scores. The project’s overarching clinical question, "In adult populations with a BMI of 25.0 or greater (P), does the implementation of the 5As model (I), compared to pre-implementation practices (C), lead to improvements in patient-reported weight management behaviours (O) within a three-month timeframe (T)?" guided the evaluation process, which provided insights into the impact of the 5As model on both HCP practices and patient outcomes within the specified timeframe.
The recruitment process consisted of 25 participants who met predetermined inclusion criteria. These criterions mandated that participants, regardless of gender, were 18 years of age or older and had a BMI score of 25.0 or higher. Notably, 15 participants chose not to disclose their BMI scores to the HCP, resulting in their exclusion from the project. Collaborative efforts were undertaken to ensure a thorough understanding of the assessment process among relevant stakeholders, including the HCP and project participants. This collaborative approach fostered a comprehensive and nuanced understanding of the participant selection and engagement processes within the project.
The adult PCC located in the southwestern region of Florida was exclusively operated by an Autonomous Advanced Practice Registered Nurse - Healthcare Provider. The patient population served by the clinic ranged from 18 to 80 years of age, with a significant proportion falling within the overweight or obese BMI categories. Utilization of an Electronic Health Record (EHR) system at the clinic facilitated seamless access to collect both pre-intervention and post-intervention measurement data. Notably, there were no associated costs incurred with the implementation of this project.
The primary metric focused on patient-reported weight management behaviors, which were systematically evaluated and quantified through the 30-item Weight Control Strategies Scale (WCSS) survey, with each item rated on a scale from 0 (Never) to 4 (Always) (Refer to Figure 2) [5]. The WCSS survey comprised four distinct subscales -dietary choices (WCSS-DC), self-monitoring (WCSS-SM), physical activity (WCSS-PA), and psychological coping (WCSS-PC)- which demonstrated strong reliability and validity within the cohort of overweight and obese patients [6]. Notably, increased WCSS scores correlated with corresponding changes in weight [6]. BMI scores were employed as a secondary metric.
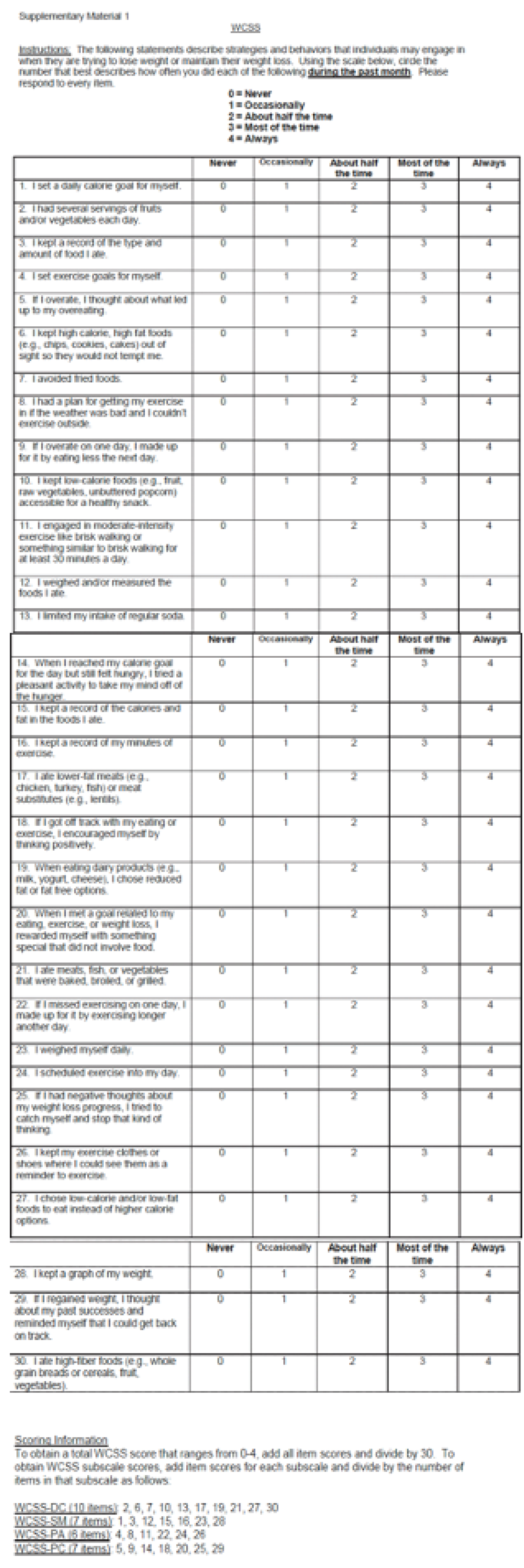 Figure 2: WCSS survey (patient-reported weight management behaviors).
View Figure 2
Figure 2: WCSS survey (patient-reported weight management behaviors).
View Figure 2
A comprehensive six-day training session was held for the HCP from August 26 th to August 31 st , 2023. Data collection occurred at two distinct intervals: June 25 th to August 25 th , 2023 (pre-implementation), and September 1 st to December 1 st , 2023 (post-implementation). Throughout the project's duration, collaborative efforts were made to engage with relevant stakeholders, including the HCP and project participants, ensuring a holistic comprehension of the project's dynamics. The intervention required the HCP to assess and document WCSS surveys and BMI scores from the project participants. Conversations about their current BMI and willingness to adopt behavioral changes were conducted, and evaluated through the WCSS survey (Ask, Assess). The HCP provided pertinent information on the potential health benefits associated with weight management interventions (Advise). A collaborative approach was fostered, with the HCP and project participants working together to devise a personalized care plan delineating attainable weight loss objectives (Agree). The HCP offered unwavering support to encourage the commencement of behavioral changes (Assist). Before project participants left the PCC, the HCP scheduled a three-month follow-up appointment to undergo reassessment of their WCSS surveys and BMI scores (Assist). Accurate data was collected from the EHR system, including variables such as age, gender, BMI, and WCSS survey scores. The implementation phase spanned three months in duration.
Utilizing the paired data measurement methodology, the project assessed variables both before and following the implementation of the intervention, including age, gender, BMI scores, WCSS total scores, and their respective subscale scores. All data was analyzed using the Statistical Package for the Social Sciences (SPSS) software for a statistical comparison.
The project participant cohort (N = 10) comprised an equal distribution of gender (50% male, 50% female) with ages ranging from 29 to 68 years. The median age remained constant at 49.50 years, with an interquartile range (IQR) of 21, indicating no significant change in participant ages before and after the intervention (Refer to Figure 3). Before the intervention, the median BMI was 30.50 (IQR: 4), which decreased to a median of 27.00 (IQR: 3) after the intervention, illustrating a notable reduction in BMI scores following the intervention. The median WCSS total score increased from 1.5500 (IQR: 0.61) before the intervention to 2.8350 (IQR: 0.71) after the intervention, indicating an improvement in overall patient-reported weight management behaviors post-intervention. Across all WCSS subscale scores, there were increases in median scores from pre- to post-intervention: WCSS-DC: Median increased from 1.900 to 3.100; WCSS-SM: Median increased from 1.3600 to 2.4300; WCSS-PA: Median increased from 0.9150 to 3.3000; WCSS-PC: Median increased from 1.7100 to 2.4300. These median increases indicate improvements achieved within each specific domain of patient-reported weight management behaviors after the intervention.
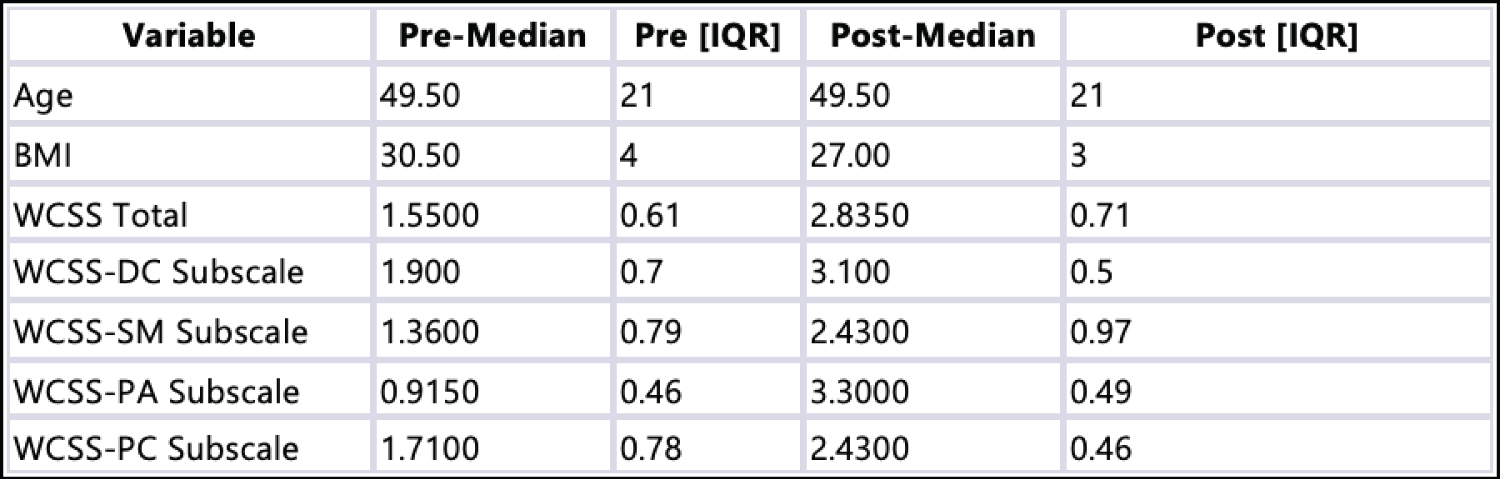 Figure 3: Median and Interquartile Range (IQR).
View Figure 3
Figure 3: Median and Interquartile Range (IQR).
View Figure 3
The non-parametric Wilcoxon Signed Ranks Test was used to evaluate the significance of changes in various key variables between post-intervention and pre-intervention assessments (Refer to Figure 4). The comprehensive analysis revealed statistically significant results across all variables examined, underscoring the positive impact of the intervention. Particularly noteworthy were the significant differences observed in BMI scores (Z = -2.848b, p = 0.004), WCSS total scores (Z = -2.810c, p = 0.005), alongside its constituent subscale scores: WCSS-DC (Z = -2.807c, p = 0.005), WCSS-SM (Z = -2.807c, p = 0.005), WCSS-PA (Z = -2.809c, p = 0.005), and WCSS-PC (Z = -2.549c, p = 0.011). These findings underscored significant improvements across the board following the intervention's implementation, as evidenced by the attainment of statistically significant p-values. They highlight the effectiveness of the intervention in eliciting positive changes in both physiological and behavioral dimensions related to weight management. Negative ranks in the comparison between post-intervention and pre-intervention scores (BMI2 vs. BMI) signified a decrease in participants' BMI scores following the intervention, indicating positive effects such as weight loss or maintenance. Conversely, positive ranks in the comparison between post-intervention and pre-intervention scores (WCSS2 Total vs. WCSS Total) suggested an improvement in patient-reported weight management behaviors post-intervention. Similar outcomes were observed in the subscale scores (WCSS-DC2, WCSS-SM2, WCSS-PA2, WCSS-PC2 vs. WCSS-DC, WCSS-SM, WCSS-PA, WCSS-PC), further highlighting the improvements in patient-reported weight management behaviors after the intervention.
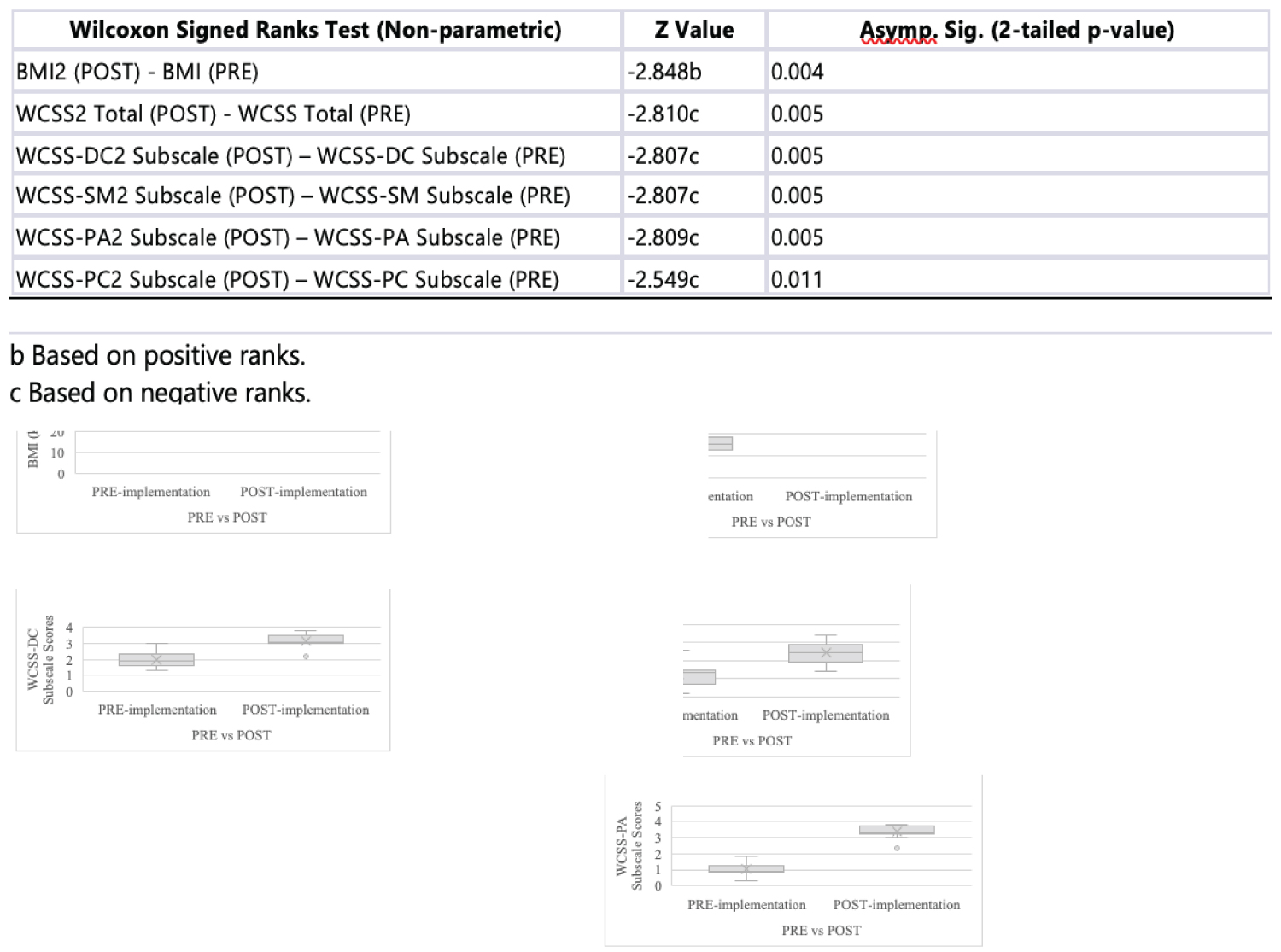 Figure 4: Wilcoxon signed ranks test& box plots.
View Figure 4
Figure 4: Wilcoxon signed ranks test& box plots.
View Figure 4
The statistical analysis revealed a correlation between improved WCSS and reduced BMI scores, indicating positive outcomes in both physiological and behavioral aspects of weight management. The 5As Model intervention effectively promoted healthier behaviors and yielded positive results for all participants. These improvements in BMI and WCSS scores suggested the intervention's success in fostering healthier behaviors. It also significantly impacted participants' weight management approaches, resulting in favorable changes in both physical health and weight management strategies. Consistent findings across all participants highlighted the intervention's robust effect within the studied population, demonstrating its efficacy in promoting healthier behaviors and weight management outcomes. Furthermore, statistical analyses confirmed the reliability and validity of BMI and WCSS scores among project participants, providing additional evidence of the intervention's effectiveness.
The implementation of the 5As model in the primary care clinic for preventing and managing obesity demonstrated significant potential in enhancing healthcare practices and advancing patient outcomes. The findings of the project provided valuable insights into the effectiveness of the 5As model in facilitating weight management interventions and improving patient-reported behaviors. One notable strength of the 5As model was its evidence-based systematic approach to addressing obesity through behavior change. By following the steps of Ask, Assess, Advise, Agree, and Assist, the HCP guided the project participants through a structured process aimed at promoting healthier habits and facilitating sustainable weight loss. Additionally, this structured approach empowered the HCP to engage in meaningful conversations with the project participants, assessing their readiness for change, and tailoring interventions to individual needs and preferences.
The results of the project demonstrated significant improvements in both patient-reported weight management behaviors and BMI scores following the implementation of the 5As model. This indicated that the intervention effectively prepared the HCP to establish weight management services within the primary care environment and aided overweight or obese adults in achieving their weight loss goals through behavioral changes. The observed enhancements in patient-reported behaviors, as measured by the WCSS survey, underscored the positive impact of the 5As model on promoting healthier lifestyles and fostering behavior change among patients. The results of this project were consistent with prior research that validated the effectiveness of the 5As model in addressing obesity within outpatient settings. The 5As model offered promise for enhancing obesity prevention and management within primary care settings by empowering healthcare providers with improved abilities to initiate weight management services and assist patients in behavior change.
The project, while holding significant promise, encountered inherent limitations that necessitated careful consideration. One notable constraint was the relatively brief implementation duration, which spanned a concise three-month period. While this temporal constraint contributed to the project's focused nature, it may have affected the depth and comprehensiveness of the insights obtained. Additionally, the project faced a modest sample size, deliberately chosen to meet specific research objectives but imposing limitations on the generalizability of findings to broader populations. Awareness of these potential biases underscored the commitment to transparent reporting and rigorous methodological scrutiny.
The global epidemic of obesity presented a significant public health challenge, necessitating effective weight management behavior strategies. The implementation of the 5As model within primary care settings emerged as a promising approach to address this challenge. Through a systematic and evidence-based approach, healthcare providers could guide behavioral changes among adult patients grappling with overweight or obesity, fostering comprehensive weight management plans tailored to individual needs. This project sought to enhance obesity prevention and weight management services within a primary care clinic by methodically implementing the 5As model. The results demonstrated statistically significant improvements in patient-reported weight management behaviors (WCSS survey scores) and reductions in BMI scores following the intervention. Despite limitations such as the relatively brief implementation duration and modest sample size, these findings underscored the potential of the 5As model to positively impact patient outcomes and enhance the proficiency of healthcare providers in managing obesity within primary care settings. Moving forward, further research and implementation efforts were warranted to explore the long-term effectiveness and scalability of the 5As model in combating obesity on a broader scale.
Heartfelt appreciation is extended to the PCC for generously providing the opportunity to conduct the project. This acknowledgment not only appreciates the organizational support but also recognizes the dedicated staff members at the PCC, whose active participation was essential to the project's progress. Special thanks are reserved for the project participants whose generosity in volunteering their time and insights were paramount to the successful completion of this project. Their willingness to actively engage in the project not only enriched its content but also underscored the collaborative spirit that defined this project endeavor. Gratitude is extended to the College of Nursing at the University of South Florida for providing essential resources and facilitating crucial data access.