Obesity is an American epidemic, affecting 35% of US adults, and 17% of US children [1]. These rates of obesity are above the Healthy People 2020 targets of 30.5% and 14.5%, respectively [2]. Obesity is defined as a Body Mass Index (BMI) ≥ 30 kg/m² [2].
Obesity costs hundreds of billions of dollars to the health care system annually, is associated or directly related to 60% of type 2 diabetes and is a well-recognized risk factor for high blood pressure, heart disease and stroke [3,4].
This article will review the causes, screening recommendations, and roles of diet, exercise, lifestyle counseling, pharmacotherapy and bariatric surgery related to obesity and its management. A simple overview of obesity management can be seen in Figure 1.
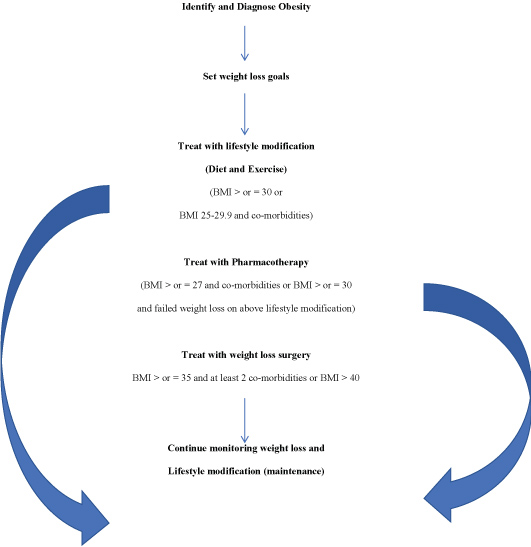 Figure 1: Management of obesity. View Figure 1
Figure 1: Management of obesity. View Figure 1
Obesity is a complex, multifactorial disease that develops from the interaction between genotype and the environment. Our understanding of how and why obesity occurs is incomplete; however, it involves the integration of social, behavioral, cultural, physiological, metabolic, and genetic factors [5]. Genetics has been a common variable researched among scientists, and the link has been proven between genetic predisposition and likelihood of developing obesity [6]. Multiple obesity-genes have been identified and confirmed to predispose to obesity and impair appetite and food regulation in the hypothalamus [6]. However, given the rapid rise of obesity in the past three decades in the United States and other Westernized countries, environmental factors are likely the major culprits in causing this unhealthy trend [7].
Sedentary lifestyle, such as time spent in front of media sources, shows a strong correlation with development of obesity [8,9]. Children are exposed to a large number of television advertising throughout childhood, including exposure to high-calorie, low nutrition-dense food ads. A study undertaken by the Kaiser Foundation confirmed the pervasive nature of media advertising and its link to the development of childhood obesity [10].
Socioeconomic status (SES) is often implicated as a risk factor for obesity. Disparity among socioeconomic groups is thought to be a primary cause of obesity, with the higher income groups enjoying lower rates of obesity in Westernized countries [11]. This link between SES and obesity is dependent upon geography. Lower rates of obesity exist among the lower SES groups in non-Westernized countries, likely due to poor nutrition, among other reasons [11].
Another less obvious but still likely cause of obesity includes sleep deficit [12]. Sleep deprivation induces hormonal changes that favor the development of obesity, including causing higher levels of ghrelin and lower levels of leptin [13,14].
The United States Preventive Services Task Force (USPSTF) recommends that clinicians screen all adults for obesity (B recommendation) [15]. The National Institutes of Health and the Canadian Task Force on Preventive Health Care also recommend the use of BMI and waist circumference to screen adults for obesity [16,17].
Which works better for achieving and maintaining weight loss, diet alone, exercise alone, or both? Interventions that included both reduced energy intake (eg, ≥ 500 kcal/d) and increased physical activity (eg, ≥150 minutes a week of walking), with traditional behavioral therapy, generally produced larger weight loss than interventions without all 3 specific components [18]. A meta-analysis of weight-loss clinical trials confirmed that interventions combining both diet and exercise achieved and maintained greater weight loss over a four-year period vs. either diet or exercise alone [19].
There is strong evidence that physical activity alone, i.e., aerobic exercise, in obese adults results in modest weight loss and that physical activity in overweight and obese adults increases cardiorespiratory fitness, independent of weight loss [16]. However, other evidence shows that nutrition counseling is more effective than physical activity counseling at achieving weight loss [20]. The American Association of Clinical Endocrinologists (AACE), in their latest obesity clinical practice guidelines, strongly recommend the triad of a healthy meal plan, physical activity, and behavioral interventions for all patients who are treated for obesity [21].
Various dietary strategies, including low carbohydrate, low fat, high fat, high protein, moderate carbohydrate, and Mediterranean-style have been studied for weight loss, with similar short/long-term weight loss outcomes [22-27]. Other dietary strategies are useful for treating obesity. Portion control, documenting what you eat, weighing oneself and planning meals all help in both weight loss and weight maintenance [19]. The regular use of portion-controlled servings of conventional foods improves the induction of weight loss in behavior-based approaches [28-30]. Meal replacement strategies have also been shown to improve outcomes in overweight and obese individuals [31].
Low Calorie Meal Plans (LCMPs) have been defined as meal plans that provide approximately a 500 to 1,000 kcal/day reduction from usual intake [32]. Very Low-Calorie Meal Plans (VLCMPs) are meal plans or liquid formulations that provide an energy level between 200 and 800 kcal/day [32]. These meal plans are designed to produce rapid weight loss in patients with BMI > 30 kg/m² who have other significant comorbidities or have failed other approaches [33]. Long term outcomes comparing VLCMPs and LCMPs do not clearly distinguish which dietary strategy works better [34,35].
Exercise and physical activity is the other part of the foundation for weight loss management. Numerous studies confirm that regular exercise and physical activity assist in weight loss, simply by burning more energy than consuming [16]. Exercise also improves many other aspects of health, enhancing focus and concentration, improving mood, reducing visceral fat, lowering blood pressure, and many other positive effects [16]. Regular physical activity lowers risk of obesity-related conditions and decreases mortality among obese individuals [36]. A Cochrane review confirmed that exercise is a useful intervention to enable weight loss [37]. Americans are trying - the most recent data indicate that the percentage of adults aged 18 or over engaging in aerobic physical activity and muscle strengthening activity has surpassed The Healthy People 2020 target for physical activity of 20.1% or more [2].
Use of weight loss drugs is potentially indicated in overweight patients with one or more obesity-related co-morbidities and in any obese patient [38]. Several prescription drugs are now Food and Drug Administration (FDA)-approved for both short- and/or long-term use in weight loss management [39]. Phentermine is the most popular appetite-suppressant (anorexiant) by prescription but is only approved for up to 12 weeks consecutive use by the FDA [39,40]. Other anorexiants are available, but their potential for side effects (physical/psychological addiction, hypertension, insomnia, palpitations, dry mouth, gastro-intestinal disturbance, etc.) makes them less optimal for use in obesity management [41]. Long-term pharmacotherapeutic agents, such as phentermine/topiramate, lorcaserin, naltrexone/bupropion, and liraglutide all have relatively similar efficacies over a 1-year period [39,42].
Side effects of these long-term agents vary and, along with typical dosing and weight-loss efficacy, are included in Table 1 [38,43,44].
Table 1: FDA-approved weight loss drugs. View Table 1
Orlistat is both available with or without a prescription and has modest weight loss maintenance over a 1-year period [42]. There is no indication that currently available anti-obesity medications are associated with pulmonary hypertension, valvular dysfunction or other cardiovascular abnormalities associated with earlier anti-obesity medications [38,42].
Table 2 below summarizes findings from a 2015 meta-analysis which examined common medications associated with secondary weight change [45]. Insulin therapy was not directly studied in the meta-analysis but is known to cause weight gain [46-49]. There are other classes of medications associated with weight gain, including beta-blockers, [50] antihistamines, [51] certain selective serotonin reuptake inhibitors (paroxetine, citalopram, escitalopram, and nortriptyline), [52] progestin-only contraceptives (implant, levonorgestrel-releasing intrauterine system, or injectable medroxyprogesterone), [53] and combined oral contraceptives, [54] but the 2015 meta-analysis found statistically insignificant or low-quality evidence to confirm or deny their effect on weight.
Table 2: Medications associated with weight gain/change. View Table 2
As discussed above, though it has been well established that modifications in nutrition and physical activity will yield weight loss, many patients do not implement these modifications. Family physicians can assist patients in achieving and maintaining weight loss (> or = to 5% of initial weight) by providing intensive, brief lifestyle counseling sessions on a scheduled basis [55]. The USPSTF also recommends high-intensity behavioral interventions, at a frequency of 12-26 sessions per year, as being the most likely form of intervention to achieve weight loss success [15].
Motivational interviewing, defined as "a client-centered, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence" is the cornerstone of effective weight loss counseling [56]. A review of various motivational interviewing studies confirms the effectiveness of this behavioral counseling technique in achieving and maintaining weight loss among adults [57]. Continued monitoring and counseling is necessary to assist with weight loss maintenance, otherwise weight regain is likely to occur [58].
Another model which has been effectively utilized by family physicians in the office setting is the "5 A's" model, which was modified for use in obesity management by Kolasa in 2010 (see Table 3) [59]. This model is best implemented when a patient lacks education surrounding a topic but may express existing readiness for change.
Table 3: The 5 A's of obesity evaluation and treatment.
Reprinted with permission from JFP "Weight loss strategies that work", Kolasa 2010 The 5 A's of Obesity Evaluation and Treatment.
View Table 3
Bariatric surgery, also known as weight loss surgery, has become safer and more effective over the past two decades [60]. A comparison of the most common weight loss surgical procedures in the United States and their long-term efficacy and cardiovascular risk is detailed elsewhere [61]. Sleeve gastrectomy, as it has evolved from the duodenal switch procedure, is now the most popular surgical procedure for weight loss [61]. Several studies and reviews confirm its short- and now longer-term efficacy at maintaining weight loss in adults, akin to its brethren weight loss surgical procedures [62-65]. Due to a relative lack of long-term data, direct comparison of the benefits between bariatric procedures and non-bariatric weight loss approaches beyond three years remains unclear [66]. However, one prospective longitudinal cohort study has shown efficacy of laparoscopic adjustable gastric banding (LAGB) in maintaining a 10-year mean weight loss of up to 47% from pre-surgical status [67].
Indications for bariatric surgery have been established and have evolved to be more inclusive in more recent years. (See Table 4 below) Contraindications to bariatric surgery include performing surgery specifically for only lowering lipids, cardiovascular risk or achieving glycemic control; untreated major depression or psychosis; binge eating disorder; active substance or alcohol abuse; severe cardiovascular disease; and an inability to adhere to nutritional supplementation [68].
Table 4: Indications for Bariatric Surgery [68,69]. View Table 4
In children and adolescents, weight loss surgery has not been well-studied. There is a lack of randomized controlled trials comparing weight loss surgery vs. non-surgical approach to weight loss and similarly a lack of long-term follow up to assess the impact of surgery as patients enter adulthood [70].
Cost effectiveness of weight loss surgery, in particular Roux-en-Y gastric bypass (RYGB) and LAGB has been established in several systematic reviews [71-75].
While not all studies have shown decreased health care costs associated with weight loss surgery [76-78], the rise in popularity of laparoscopic sleeve gastrectomy will likely prove it to be equally or even more cost-effective as a surgical option [79].
Co-morbidities among obese and the severely obese patients are the norm. In particular, more than 90% of type 2 diabetics are overweight or obese [80]. Weight loss surgery does induce long term remission of type 2 diabetes and is more effective than medication or lifestyle alone at inducing and maintaining remission, both in the short- and long-term [81-84].
Another common co-morbidity among pre-operative bariatric patients is depression. In a meta-analysis, depression was present in 19% of patients seeking and undergoing weight loss surgery [85]. Bariatric surgery was shown to be consistently associated with postoperative decreases in the prevalence of depression [85].
Finally, there are known morbidity and mortality risks to bariatric surgery, although the published mortality rate is 0.3% [86,87]. On the contrary, there is new data demonstrating lower mortality rates after five and ten years among patients having undergone bariatric surgery vs. controls, with an absolute risk reduction approaching 10% [88].
In pediatric patients, obesity cutoff points are different than in adults; they have remained the same, but the terminology has notably changed. A BMI of 95th percentile and 85th percentile, respectively, delineate cutoff points for what is now called pediatric obesity and overweight, which translate into risk categories related to body fat level. Exceptions to this rule are:
1. Adolescents, where the definition of obesity should be given either if BMI is at least 30 kg/m² or at or above the 95th percentile, whichever is lower; and
2. Children less than 2 years of age, where weight-for-height values rather than BMI are used [89,90].
In assessing children once obesity is diagnosed, family medicine practitioners should obtain history regarding nutrition and physical activity (just as in adults), and perform a physical exam; if risk factors (such as family history of obesity or its comorbidities, abnormal exam findings, or positive review of systems) are identified, laboratory screening including fasting glucose, lipid profile, and liver function tests should be performed [90,91]. Further testing and investigation for secondary causes of obesity (e.g. MC4R genetic mutation, hypothyroidism, syndromic causes, medication side effects) should be performed only when there are other abnormal findings on physical exam, particularly a height deficit [91].
In managing childhood obesity, the American Academy of Pediatrics (AAP) has released a helpful algorithm which outlines an escalating 4 stage approach depending on the severity of the child's obesity and the child's response to treatment [92]. The AAP's expert committee urges clinicians to be "supportive, empathetic, and nonjudgmental" when discussing weight with children [90].
Obesity is an ever-increasing condition seen among patients in the primary care setting. Family physicians are ideally suited to identify, evaluate, and manage this condition. Based on the current available research, and in tune with the family medicine style of providing comprehensive, continuous and compassionate care, setting short- and long-term goals and establishing appropriate and regular follow up with patients as they engage in lifestyle modification is the best approach to helping patients achieve weight loss and maintenance of weight loss. Adjunctive therapies, including FDA-approved weight loss drugs and/or bariatric surgery, are also potentially very useful tools in the treatment of obesity.