Background: Secondary Male Hypogonadism (SMH), described as dysfunction of the hypothalamic-pituitary-testicular axis, is commonly caused by obesity.
Objectives: To evaluate the effect of decreasing body weight and waist circumference (WC) on male sex hormones in obese men.
Methods: Retrospective study; reviewed the medical records: 42 male patients; ABC region, São Paulo state; aged between 28 and 69 years. Evaluated: body weight, height, WC, total cholesterol (TC) and fractions, liver enzymes, alkaline phosphatase (AP), total testosterone (TT), free testosterone (FT), sex hormone-binding globulin (SHBG), estradiol (E2), luteinizing hormone (LH), follicle-stimulating hormone (FSH), Body Mass Index (BMI); men previously diagnosed with obesity (BMI ≥ 30 kg/m2). A descriptive data analysis was performed. Quantitative variables were presented as measures of central tendency and variability according to the data distribution using the Shapiro-Wilk test. To compare the clinical variables before and after treatment, the paired t-test and Wilcoxon test were used to analyze the normality of the data.
Results: After the decrease in body weight: significant decrease in aspartate transaminase (SGOT/AST), pyruvic transaminase (SGPT/ALT), gamma glutamyl transferase (γGT), SHBG, weight, BMI, waist circumference (WC), TC, low-density lipoprotein (LDL) cholesterol, very low density lipoproteins (VLDL) cholesterol and E2 values. High-density lipoprotein (HDL) cholesterol, TT, and FT levels were significantly higher after the decrease in body weight. Conclusions: In men with obesity, SMH, and increased WC, the most recommended treatment is a reduction in body weight and patients are counseled to avoid the use of exogenous testosterone, which can lead to testicular atrophy and late infertility.
Obesity, Male hypogonadism, Testosterone, Estradiol, Cholesterol
Obesity is considered a global health problem [1]. In 2016, according to the World Health Organization (WHO), 39% of adults were overweight, of which 13% were obese [2].
In Brazil, obesity increased by 54% between 2006 and 2011, and it is estimated that by 2025, it will be the fifth country to have obesity problems [3].
The Body Mass Index (BMI), used to classify body mass, was developed in Belgium by the statistician, Adolphe Quetelet [4] and is calculated by dividing an individual's weight in kilograms by the square of their height in meters (BMI = weight (kg)/height 2 (m 2 )).
Obesity is defined as the abnormal or excessive accumulation of fat. The current definitions establishing the cut-offs were agreed upon in 1997 and were published in 2000 (WHO 2000) [5].
According to the WHO, a BMI greater than or equal to 25 kg/m 2 is classified as overweight, a BMI greater than 30 kg/m 2 is considered obese, and a BMI greater than 40 kg/m 2 is considered severe obesity [6].
Obesity is diagnosed clinically by calculating the BMI or using other anthropometric methods to analyze the distribution of body fat, such as measurements of skin folds, waist circumference (WC), waist-to-hip ratio, or sagittal diameter [7].
Obesity is associated with an increased risk of premature mortality [8] and an increased risk of comorbidities. Thus, obesity is associated with the development of other diseases, such as cardiovascular diseases, arterial hypertension, type 2 diabetes mellitus, respiratory diseases, orthopedic diseases, osteoarthritis, dermatological diseases, increased incidence of gallstones, hepatic steatosis, increased cholesterol and triglycerides, and male hypogonadism [9].
More severe obesity (BMI > 35-40 kg/m 2 ) is associated with reductions in testosterone (T) although obesity with a BMI of less than 35-40 kg/m 2 is also associated with a reduction in total testosterone (TT) and sex hormone-binding globulin (SHBG) [10].
In population-based studies, obesity was the single most important factor that resulted in T deficiency [11].
Physiologically, T is produced in the Leydig cells of the testicles and is stimulated by pituitary secretion of luteinizing hormone (LH). In serum, 50% of T is bound to albumin and free T (FT) represents 2% of TT [12]. T is converted to estradiol (E2) by the enzyme aromatase, which subsequently activates estrogen receptors ERa and ERb [13].
In the European Male Aging Study, obese men (BMI > 30 kg/m 2 ) had a 30% lower testosterone concentration, a reduction equivalent to nearly three decades of aging, and a 13-fold increase in the prevalence of late-onset hypogonadism (LOH) [14].
Many men with LOH suffer from chronic metabolic conditions, mainly obesity and diabetes mellitus, but LOH can result from certain medications and conditions such as glucocorticoids, opioids, tricyclic antidepressants, psychosocial stress, sleep apnea, and chronic obstructive pulmonary disease [15].
Clinical evidence suggests that low T levels are a risk factor for cardiovascular disease [16].
There is a bidirectional relationship between obesity and hypogonadism [17]. Thus, evidence highlights that male hypogonadism can lead to increased adiposity, whereas obesity can be a cause of male hypogonadism [18].
T deficiency is associated with visceral fat dysfunction, chronic inflammation, insulin resistance, and low levels of SHBG [19].
In obese individuals, increased amounts of aromatase enzymes produced by adipose tissue reduce T levels and increase estrogen hormone levels. T deficiency further facilitates adipocyte differentiation, inflammation, and insulin resistance. The resulting increase in estrogen, leptin, insulin, and inflammatory cytokines results in the suppression of the hypothalamic-pituitary-testicular (HPT) axis [20].
Male hypogonadism is characterized by inadequate testicular production of sex steroids and sperm [9]. The 2010 Endocrine Society guidelines define hypogonadism in men as “a clinical syndrome arising from failure of the testicles to produce physiological levels of T, androgen deficiency, and a normal number of sperm due to disruption of one or more levels of the HPT axis” [21].
Primary male hypogonadism occurs when there is testicular dysfunction [22] and secondary male hypogonadism (SMH) occurs when the HPT axis is dysfunctional [23]. The most common cause of SMH is obesity [21,22] and 60% of men are obese [24]. The increase induced by obesity in the levels of leptin, insulin, pro-inflammatory cytokines, and estrogen can cause functional hypogonadotropic hypogonadism with defects at the level of gonadotropin-releasing hormone (GnRH) hypothalamic neurons [25].
Male Obesity-associated Secondary Hypogonadism (MOSH) is becoming a public health problem and epidemiological studies suggest that prevalence rates are as high as 45.0-57.5% [9]. MOSH impairs fertility, sexual function, mineralization, and fat metabolism resulting in increased fat accumulation, muscle mass deterioration, and body composition alteration [18,26].
Obesity is one of the alarming health problems in modern societies that lead to infertility [27].
According to some authors [28], obesity can negatively impact sperm quality, and consequently, male fertility. It is estimated that 15% of couples are infertile, with male infertility contributing to 50% of the cases [29].
Inflammatory cytokines disrupt the HPT axis and steroidogenesis, causing hypogonadotropic hypogonadism and altered spermatogenesis, with poor semen parameters, including DNA fragmentation and epigenetic damage and modification [30].
Obesity often leads to non-alcoholic fatty liver disease (NAFLD), which covers a broad histological spectrum from simple steatosis to non-alcoholic steatohepatitis (NASH) and can progress to fibrosis, cirrhosis, and even hepatocellular carcinoma. Since sex steroids are metabolized in the liver and their serum levels depend in part on hepatic SHBG secretion, NAFLD may be related to the observed changes in sex steroid levels in obese men [31].
Hepatic steatosis is defined by the presence of fat encompassing 5% of the liver weight in the absence of inflammation [32] with a reduction in SHBG produced by the liver [33].
Non-alcoholic fatty liver disease (NAFLD) is considered a feature of the metabolic syndrome (MetS) and contributes to cardiovascular disease (CVD) and authors have evaluated the relationship of NAFLD with male sexual problems and infertility [34].
Obesity and metabolic syndrome (MetS) are currently considered epidemics worldwide, driven by an obesogenic pathology of the environment, in which chronic inflammation is an important etiological factor [30].
According to Grossmann [35], obesity is an increasing prevalence worldwide, is the clinical condition most strongly associated with reduced concentrations of T in men, and is one of the strongest predictors of receiving treatment with T.
The objective of this study is to evaluate the effect of decreasing body weight and WC on male sex hormones in obese men.
This was a retrospective review of medical records of patients seen between 2015 and 2018 at the Medical Clinic of Endocrinology in the municipality of Santo André, state of São Paulo, Brazil.
A total of 42 adult men, aged between 28 and 69 years, from the ABC Region and São Paulo City, State of São Paulo, presented to the Medical Clinic of Endocrinology, in the city of Santo André, State of São Paulo, Brazil for the treatment of obesity.
Data from the medical records of patients from the physical examination, such as blood pressure (BP), body weight, height, BMI, WC, and laboratory tests, including total cholesterol (TC), high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and very low density lipoproteins (VLDL) cholesterol; liver enzymes such as aspartate transaminase (SGOT/AST), pyruvic transaminase (SGPT/ALT), gamma glutamyl transferase (γGT), alkaline phosphatase (AP), total testosterone (TT), free testosterone (FT), sex hormone-binding globulin (SHBG), estradiol (E2), luteinizing hormone (LH), follicle-stimulating hormone (FSH). These data were collected before and after obesity treatment, lasting between 12 and 13 months, which consisted of guidance, dietary education, and regular physical activity to reduce body weight without the use of medication. LDL cholesterol treatment was performed using statins during the entire obesity treatment period.
The age of 42 patients was considered the first medical appointment. The averages of the results obtained by referring to the physical and laboratory examinations before and after treatment for obesity and cholesterol were considered for data analysis.
Patients with type 1 and 2 Diabetes Mellitus, increased triglyceride levels, excessive alcohol, medicines like glucocorticoids, opioids, tricyclic antidepressants were excluded.
The methods and reference values used for each laboratory test are listed in Table 1. All these parameters were analyzed in serum.
Table 1: Methods and references considered for laboratory tests measured in patient serum. View Table 1
A descriptive data analysis was performed. Quantitative variables were presented as measures of central tendency and variability according to data distribution using the Shapiro-Wilk test. To compare the clinical variables before and after treatment, the paired t-test and Wilcoxon test were used to analyze the normality of the data. The confidence level adopted was 95%, and the statistical program used was Stata version 14.0.
In this study, 42 adult male patients, aged 28-69 years, were evaluated.
The data obtained from medical records are presented in Table 2 and Table 3.
Table 2: Physical examination results and lipid profiles of patients. View Table 2
Table 3: Results of liver and hormone laboratory tests of patients. View Table 3
The statistical results are presented in Table 4 and Table 5, respectively. The treatments performed on the patients in this study were guidance, dietary education and regular physical activity to reduce body weight without the use of medication or\statins for LDL cholesterol during throughout the obesity treatment period. There was a significant decrease in SGOT, SGPT, γGT, SHBG, weight, BMI, WC, TC, LDL, VLDL and E2 values. HDL, TT, and FT levels were significantly higher after treatment than before treatment. The AP level did not change during this period. There was a decrease in FSH and an increase in LH levels, but this was not statistically significant.
Table 4: Statistical results of variables with a normal distribution. View Table 4
Table 5: Statistical results of variables with non-normal distributions. View Table 5
Table 4 shows the statistical results of variables with a normal distribution.
Table 5 shows the statistical results of variables with non-normal distributions.
Figure 1 shows the mean values of BMI results and sex hormones such as TT and FT, and E2 and LH before and after treatment. There was a decrease in BMI and E2 levels, and an increase in FT, TT, and LH levels after treatment.
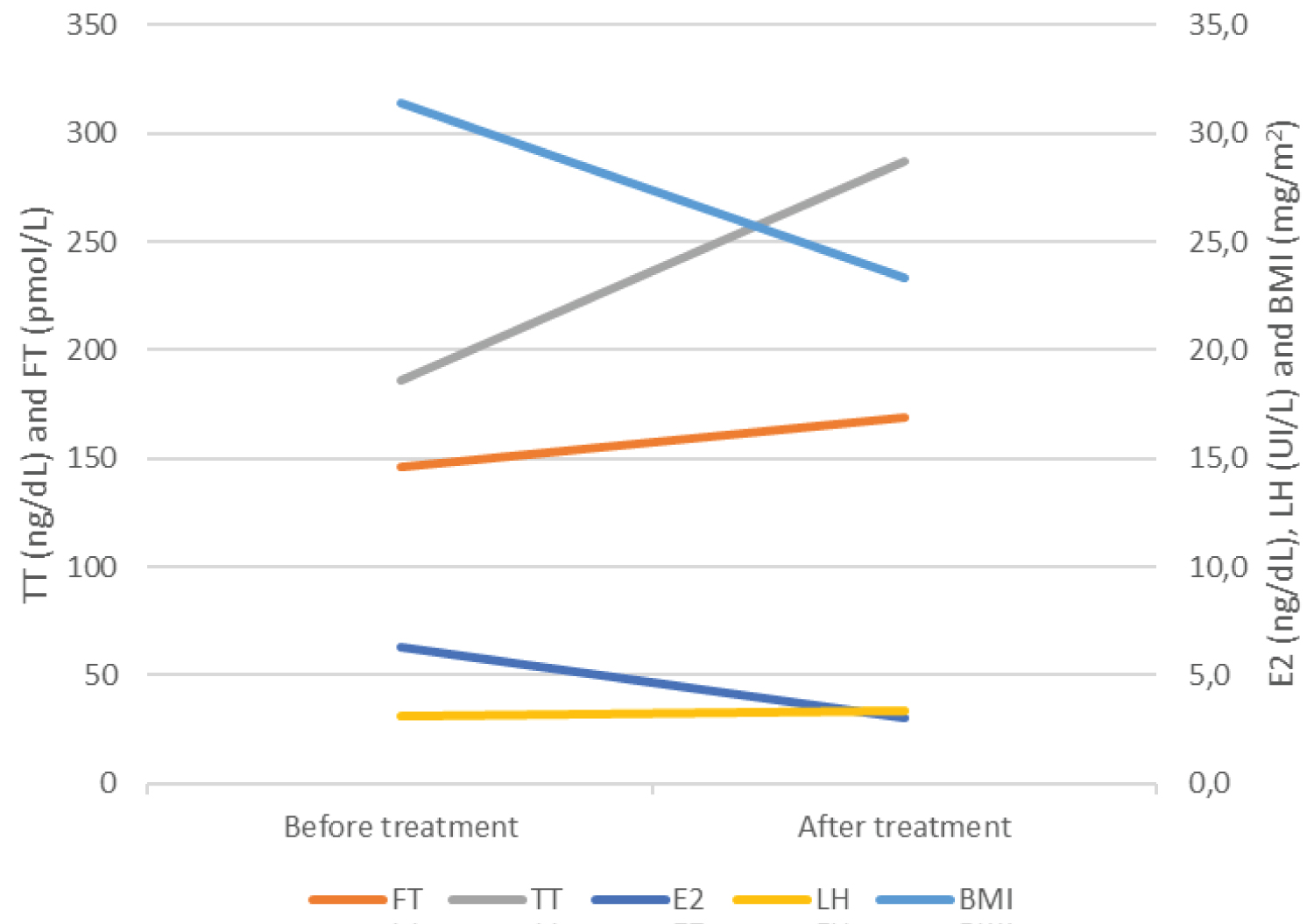 Figure 1: Mean values of BMI and sex hormones: TT, FT, E2, and LH, before and after treatment.
Figure 1: Mean values of BMI and sex hormones: TT, FT, E2, and LH, before and after treatment.
BMI: Body Mass Index; E2: Estradiol; FT: Free Testosterone; LH: Luteinizing Hormone; TT: Total Testosterone
View Figure 1
Figure 2 shows the mean values of the WC results, HDL cholesterol, LDL cholesterol, SGOT/AST, SGPT/ALT, and γGT levels before and after treatment. There was a reduction in WC, SGOT/AST, SGPT/ALT, γGT, and LDL cholesterol and an increase in HDL cholesterol after treatment.
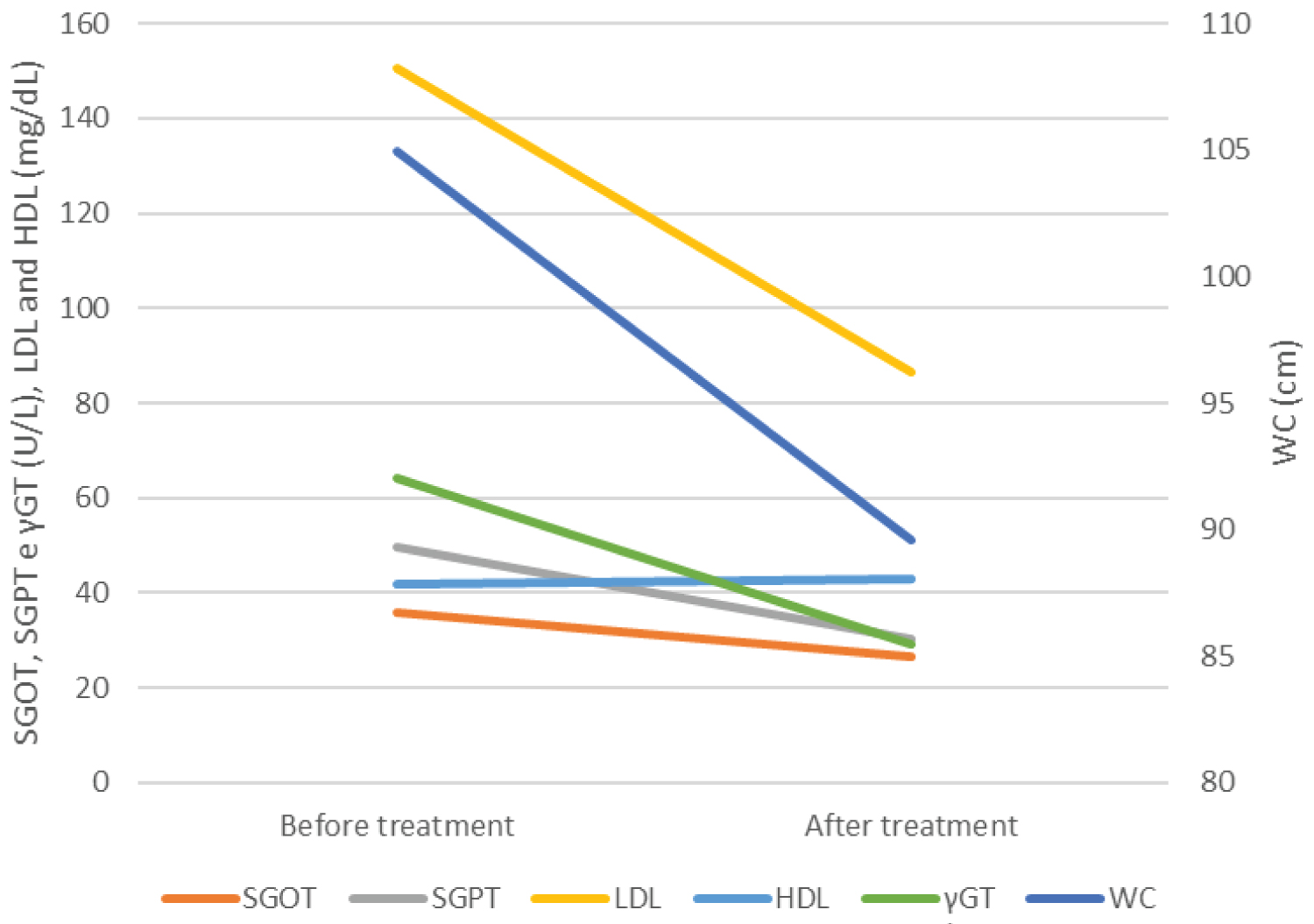 Figure 2: Mean values of WC, HDL cholesterol, LDL cholesterol, SGOT, SGPT and γGT before and after treatment.
Figure 2: Mean values of WC, HDL cholesterol, LDL cholesterol, SGOT, SGPT and γGT before and after treatment.
γGT: Gamma Glutamyl Transferase; SGOT: Glutamic Oxaloacetic Transaminase; SGPT: Pyruvic Transaminase; WC: Waist Circumference.
View Figure 2
Our results demonstrated that the decrease in BMI and WC led to a substantial improvement in TT and FT levels and a statistically significant decrease in E2 levels (Table 5).
According to some studies [36], obesity is the most important factor associated with low T levels, surpassing the effects of age and comorbidities. Furthermore, some authors [37] claim that the conversion of TT into E2 by aromatase is greater in the adipose tissue.
In adipose tissue, androgens are converted into estrogens in a reaction known as aromatization, which is catalyzed by the cytochrome P450 aromatase enzyme produced in Leydig cells. In obese men, estrone and E2 levels increase due to increased peripheral aromatization of androgens [38].
Data from the literature [38,39] report that obese men have higher levels of E2, which promotes the inhibition of the HPT axis, and causes a decrease in the stimulation of LH, which acts on the Leydig cells of the testicle, leading to the production of T and FSH, which acts on testicular Sertoli cells, stimulating spermatogenesis. Thus, there is a decrease in circulating T levels, which contributes to the development of hypogonadotropic hypogonadism.
Adipose tissue signals that interfere with hypothalamic function include the release of pro-inflammatory cytokines, increased conversion of T to E2, and release of the hormone leptin, which directly inhibits the stimulatory action of pituitary gonadotropins in testicular Leydig cells to further decrease T production. All of these signs can accentuate the expansion of fat deposits and lead to a state of hypogonadotropic hypogonadism, obesity, and metabolic syndrome [40].
In this study, we observed a decrease in FSH, an increase in LH (Table 4 and Table 5), and an increase in TT and FT with a decrease in BMI and WC (Table 5). GnRH stimulates the pituitary gland to release LH, which stimulates Leydig cells to produce T. The inverse relationship between T levels and adipose tissue expansion can affect the hypothalamus, resulting in a decrease in LH secretion by hypophysis.
Numerous epidemiological studies have shown a negative correlation between obesity and T levels, and several meta-analyses have shown that weight loss produces a proportional increase in T concentrations. It is generally accepted that hypogonadism secondary to obesity is functional, as it is reversible after weight loss [41].
De Lorenço, et al. [26] observed a significant increase in TT and a reduction of 17-β estradiol levels after nutritional intervention.
These data corroborate the results of our study, as we observed that after the treatment of obesity, in the period of 12 and 13 months, which consisted of guidance, nutritional education, and physical activity, without the use of medication, there was a decrease in E2 and an increase in TT and TL (Figure 1 and Table 5).
Androgens also play an important role in regulating body fat distribution in humans. They directly affect the differentiation, size, and expansion of the fat compartment of adipocytes. They also directly affect adipocyte function, including insulin signaling, lipid metabolism, fatty acid uptake, and adipokine production [42].
T reduces central fat deposition and in men, its deficiency is associated with increased visceral adipose tissue and insulin resistance, in addition to the dysregulation of lipid metabolism [43].
In a study by Rotter, et al. [44], in men with TT deficiency and presenting with sexual dysfunction, variables related to obesity were measured, such as BMI, waist/hip ratio, and visceral adiposity index, and it was found that in 40% of these cases, particularly for the visceral adiposity index, which was the strongest predictor of low TT among the non-diabetic male population.
In this study, diabetic men were excluded, and we observed that the mean BMI found before treatment indicated that these patients had grade I obesity, and the mean WC before treatment was above 90 cm, showing that they were at risk of metabolic complications increased substantially [45].
Many men with LOH suffer from chronic metabolic conditions, and LOH can result from certain medications such as glucocorticoids, opioids and tricyclic antidepressants [15], however, in this study, these drugs were excluded.
Regarding lipid parameters, we observed an increase in the mean values of SGPT and LDL cholesterol, with low mean values of HDL cholesterol (Table 2, Table 3, Table 4 and Table 5) before treatment with obesity and cholesterol.
After the decrease in BMI and WC with guidance, nutritional education, and regular physical activity, without the use of medication, and cholesterol treatment with statins (Table 2, Table 3, Table 4 and Table 5), we observed a significant decrease in the values of SGOT, SGPT, γGT, TC, LDL, and VLDL (Figure 2, Table 4 and Table 5), higher HDL values (Table 4), and no variations in AP (Table 4).
According to the authors [46], hypoandrogenism is associated with the reduction of HDL cholesterol and elevation of LDL cholesterol, TC, and triglycerides.
In a study of obese young men with MOSH (age ranging from 20 to 60 years, mean 38 ± 15 years), the authors evaluated, in addition to low TT and lipid levels, and observed an increase in TC, triglycerides and LDL [47].
In this study, men with increased triglycerides levels were excluded.
Obesity also reflects reduced concentrations of SHBG [35], which is secreted by hepatocytes, and sex steroids are metabolized in the liver.
According to some authors [48] inhibition of hepatic synthesis and SHBG release results in negative regulation of TT production.
According to Michalakis , et al. [49], a reduction in total TT and SHBG concentrations during a 9-year follow-up in overweight men compared to lean men in the Massachusetts Male Aging Study and did not observe differences in FT.
In this study, we observed a decrease in SHBG and E2 levels and an increase in TT and FT levels after a decrease in BMI and WC in obese patients (Figure 1, Table 4 and Table 5).
There is increasing evidence linking NAFLD to male sexual and reproductive dysfunction [34,50].
Some studies [51] have investigated whether the severity and histologic components of NAFLD are associated with sex steroid levels in obese men and among the histological components of NAFLD, only steatosis was independently associated with TT (rs = -0.331, p = 0.003) and FT levels (rs = -0.255, p = 0.025).
Imaging examinations and liver histological components were not observed after reviewing the medical records of this study. We observed a significant decrease in the values of SGOT, SGPT, and γGT after a decrease in BMI and WC with guidance, dietary education, and regular physical activity, without the use of medication (Figure 2, Table 4 and Table 5), and no variations in AP (Table 4). Therefore, we cannot consider that the patients in this study had NAFLD, although we excluded obese patients who excessively used alcohol.
Obesity negatively affects conventional and biofunctional sperm parameters and induces epigenetic changes that can be transferred to offspring. Furthermore, obesity-related diseases are linked to dysregulation of adipocyte function and microenvironmental inflammatory processes [52].
Recent studies have suggested an interaction between low testosterone and increased risk of mortality [53] as well as a possible cause of reproductive difficulties and infertility due to low sperm count [23].
According to Giagulli, et al. [41], diet with or without physical activity improves body weight and hypogonadism in obese adult and elderly men, with or without type 2 diabetes mellitus.
This study excluded patients with type 1 and 2 diabetes mellitus, but it also demonstrated that weight loss is an important factor for improving TT and FT levels (Table 4 and Table 5).
According to some authors [54] the treatment of primary male hypogonadism involves only exogenous T and although recent evidence does not indicate an increased risk of cardiovascular events, the use of exogenous T still raises doubts regarding its cardiovascular safety.
Other authors [55] have reported that the use of exogenous T affects the feedback mechanism of the HPT axis and, as a consequence, impairs spermatogenesis and testicular atrophy in the long term; thus, the use of exogenous T becomes a harmful option in young men with hypogonadism who wish to maintain fertility.
In 2015, the United States Food and Drug Administration issued a warning about potential cardiovascular risks from the use of exogenous T, and fertility preservation is another reason to look for viable alternatives [56]. Other side effects of the exogenous use of T have also been reported, such as erythrocytosis [57], male infertility, atrophy and gynecomastia [58].
Global increases in T prescriptions [59] and a marked increase in the prevalence of obesity, together with secular trends of reductions in circulating T, have likely contributed to an increasing number of obese men receiving T treatment.
In comments by authors Warrick J Inder & Mathis Grossmann on Obesity and “functional hypogonadism”- mechanisms and management: on EJE-22-1110 “leflutrozole in male obesity-associated hypogonadotropic hypogonadism: Ph 2b double-blind RCT”, published in the European Journal of Endocrinology, Jones, et al. [60], conducted a double-blind randomized controlled trial of weekly leflutrozole - an aromatase inhibitor, for the treatment of “functional hypogonadism” associated with obesity. These authors [60] showed a dose-dependent increase in serum TT, LH, and FSH, along with an improvement in semen volume and motile sperm count in the subset of participants who provided semen samples. Symptoms of sexual dysfunction were not alleviated, nor was there any improvement in fatigue or general health. Adverse effects have been observed, particularly at the highest weekly dose of 1.0 mg, most commonly elevated hematocrit, hypertension, headache and increased prostate specific antigen. Bone mineral density fell significantly in the lumbar spine at all doses compared to placebo.
In the context of obesity with a BMI, 30-40 kg/m 2 , TT and SHBG are low, but FT concentrations are maintained within the normal range [60].
According to Fernandez, et al. [25], obesity-induced hypogonadism is reversible with substantial weight loss. Lifestyle measures are the cornerstone of treatment.
In this study, we did not report the use of exogenous T as a treatment for male hypogonadism resulting from obesity. Dietary guidance and regular physical activity to decrease body weight and WC were the factors that contributed to the increase in TT and FT levels, decrease in E2 levels, and improvement in the patients' quality of life. In Conclusion our results demonstrate that obese men have low mean serum values of TT and FT, high E2, normal LH and FSH, high LDL cholesterol, and SGPT. After treatment for obesity, with guidance, dietary education, and physical activity, without the use of medication, and with a decrease in BMI and WC, there was an increase in the mean serum values of TT and FT and a decrease in E2. We observed a decrease in LDL cholesterol after statin treatment and a decrease in SGPT. We did not observe variations in AP before and after the obesity treatment. Thus, obesity-induced male hypogonadism is reversible with substantial weight loss.
Therefore, the treatment of obesity with proper nutrition and regular physical activity is recommended, thus avoiding the use of exogenous testosterone, which can lead to testicular atrophy and late infertility.
The authors are grateful to patients.
The objectives and methods of this study were clearly stated for all the patients. This study was approved by the Committee of Ethics in Research of the Medical School of the ABC Foundation, SP, Brazil, and registered under number 4.915.336.
The authors declare no conflict of interest.
All authors have contributed significantly and agree with the content of the manuscript. NGMC, JFMA, ADB, and OAMG prepared the study design, the data collection, wrote paper, literature review and manuscript review. MAZM performed acquisition of data, interpretation of the results, literature review and the coordination of the study. Besides, the manuscript had not been published elsewhere and is not under consideration in any journal. All authors have seen and given their approval for submission of the revised manuscript.