As our patient population grows older with improved health care technology and resources, chronic subdural hematoma (CSDH) is an increasingly common disease faced by the modern neurosurgeon. Despite good results with burr-hole irrigation and evacuation - the gold standard treatment for CSDH - recurrence rate remains high [1,2]. Recent advancements in endovascular management of this diagnosis via embolization of the middle meningeal artery (MMA), either alone or in conjunction with surgical evacuation, have yielded promising results [1]. We present the case of a patient with CSDH managed by combination management, with microscopically visualized embolization particles in the MMA, resulting in interesting pathology findings.
Subdural hematoma, Endovascular, Embolization, Middle meningeal artery
A 77-year-old with history of prior stroke was found to have a progressive decline in cognitive and motor function. On exam, he was confused but with a symmetric motor exam and no gross motor deficit. Computed tomography (CT) scan of the head revealed bilateral septated subdural hematomas, measuring 1.5 cm on the left and 0.6 cm on the right, with roughly 0.5 cm of midline shift towards the right (Figure 1). He was not on any antiplatelet or anticoagulation therapy pre-operatively, and had a normal laboratory coagulation profile. He was treated with antiepileptic therapy - using levetiracetam - without improvement prior to intervention.
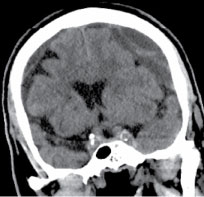 Figure 1: Coronal CT showing bilateral chronic subdural hematomas, the left causing sulcal effacement and midline shift.
View Figure 1
Figure 1: Coronal CT showing bilateral chronic subdural hematomas, the left causing sulcal effacement and midline shift.
View Figure 1
After extensive discussion with his family, decision was made to perform a preoperative embolization of the left subdural hematoma to reduce risk of recurrence, followed by craniotomy for evacuation of the mass-effect causing blood products, in a staged fashion.
The patient was taken to the angiogram suite, where conscious sedation was administered. An 80 cm Cook Shuttle was placed in the left common carotid artery via a Sim2 selection catheter. Subsequently, a Headway 21 microcatheter was used to select the middle meningeal artery via the left external carotid artery, using roadmap guidance.
Using live fluoroscopy, 100 µm Embozene particles mixed with contrast were introduced into the left middle meningeal artery, until the artery was occluded (Figure 2). Post-procedure CT revealed the presence of contrast in the left subdural hematoma, a common finding we have noted post-embolization, likely due to contrast infiltration into the CSDH through leaky capillaries during the embolization (Figure 3). Four days later, he underwent a craniotomy and evacuation of the hematoma via a mini-craniotomy, 3 cm in diameter. He tolerated the procedure quite well, and was significantly improved following the staged procedure. His confusion and lethargy improved, and he was discharged to rehab, remaining on antiepileptic therapy at discharge.
 Figure 2: A) Minimum intensity AP projection from left common carotid artery angiogram demonstrating compression of the brain parenchyma. Black arrow shows brain compression as a result of the CSDH. MMA is not well-visualized in this view; B) Lateral angiogram with headway 21 microcatheter advanced through the foramen spinosum and positioned just proximal to the bifurcation of the MMA (black arrowhead); C) Post-embolization lateral angiogram run from the external carotid artery showing complete occlusion of the MMA (dotted line).
View Figure 2
Figure 2: A) Minimum intensity AP projection from left common carotid artery angiogram demonstrating compression of the brain parenchyma. Black arrow shows brain compression as a result of the CSDH. MMA is not well-visualized in this view; B) Lateral angiogram with headway 21 microcatheter advanced through the foramen spinosum and positioned just proximal to the bifurcation of the MMA (black arrowhead); C) Post-embolization lateral angiogram run from the external carotid artery showing complete occlusion of the MMA (dotted line).
View Figure 2
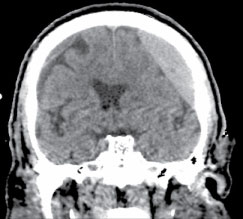 Figure 3: Coronal CT after embolization with contrast staining of the left chronic subdural hematoma.
View Figure 3
Figure 3: Coronal CT after embolization with contrast staining of the left chronic subdural hematoma.
View Figure 3
Post-operative pathological evaluation revealed the presence of embozene particles within the middle meningeal artery, and an absence of red blood cells filling the vessel (Figure 4).
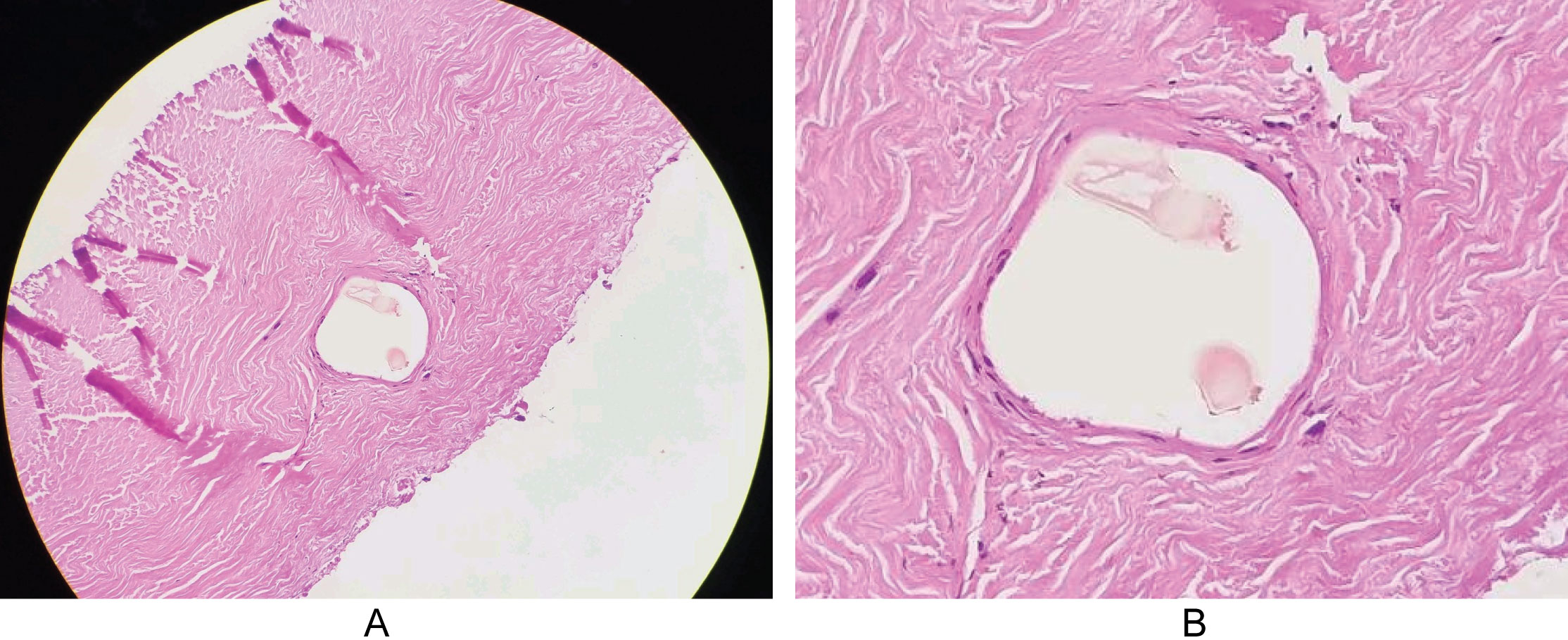 Figure 4: Pathology image of dura following MMA embolization and evacuation of hematoma, revealing classic appearance of collagen fibers in layers. Embozene particles can be seen in the middle meningeal artery, with no evidence of red blood cells within the embolizaed artery.
View Figure 4
Figure 4: Pathology image of dura following MMA embolization and evacuation of hematoma, revealing classic appearance of collagen fibers in layers. Embozene particles can be seen in the middle meningeal artery, with no evidence of red blood cells within the embolizaed artery.
View Figure 4
Refractory CSDH is reported to be as high as 5.5%. Management options include observation in asymptomatic patients and surgical management in those with symptoms or neurological deficit, including seizures. Burr-hole irrigation and evacuation and craniotomy (including mini-craniotomy) remain the most common surgical options, though additional options such as endoscopic surgery exist [1]. Conservative management options include anti-epileptic therapy and a course of steroid (currently under investigation via a randomized control trial), which may reduce inflammation and angiogenesis [3].
Embolization of the MMA is an exciting development in the management of this disease process. Contraindications to endovascular embolization are rare, and include renal failure and lack of safe arterial access to the MMA via the internal maxillary artery, a branch of the external carotid artery [1]. Caution should be applied to ensure there is not a connection between the MMA and the ophthalmic artery, a common anatomical finding. Otherwise, this procedure can be safely done with conscious sedation, and several case studies regarding its efficacy and safety are published.
Review of the literature by Tempaku, et al. [2] found 21 patients who had undergone MMA embolization for recurrent CSDH following surgical evacuation. None of these patients had recurrent hemorrhage following embolization, some of whom had undergone three or more surgical evacuations [2]. More recently, Link, et al. discussed five cases that underwent MMA embolization as primary treatment of CSDH without surgical evacuation, all with symptomatic relief and radiographic improvement [4]. We utilize MMA embolization in patients who are minimally symptomatic, elderly, and/or those who require more expedient resumption of antiplatelet or anticoagulant therapy. Our patient, given that he was elderly and there is a risk of recurrence, underwent embolization prior to evacuation.
The MMA supplies blood to the dura mater. Histopathological analysis has demonstrated that the arterial supply of CSDH's comes from the MMA nourishing the outer membrane, and imaging has showed enlargement of the vessel in association with this pathology [1,5,6]. Interruption of this arterial supply is thought to account for the success of this treatment strategy.
Histological visualization of the particles within the MMA in our patient, as well as the imaging finding of contrast in the subdural hematoma following the embolization support the anatomic and histological studies being performed to support this treatment. Embolization of the MMA in the treatment of CSDH, especially in patients where anticoagulation and comorbidities are a factor, is an exciting new treatment modality. Further research into its efficacy via a randomized control trial may be helpful in determining its true effectiveness, and is needed before a recommendation can be made regarding the efficacy of middle meningeal artery embolization as primary treatment for chronic subdural hematoma.
None.
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.