Although gunshot injury to the head is usually mortal, survivors frequently show retained metal shrapnel or full bullet intracranially. An important though uncommon complication of retained bullet is that of spontaneous migration. A migrating intracranial bullet is a dilemma to neurosurgeons, as its management is challenging, since the removal of a deep-seated bullet may cause additional neurological deficit. Migration of a retained bullet may cause damage to vital structures and cranial nerves, producing significant neurological damage. We report the case of a 23-year-old man who received a bullet in the head and during one month, several CT scans showed multidirectional spontaneously migrating bullet within the intracranial space. The patient was conscious with a right hemianopsia but no other eloquent neurologic deficit, even after his single seizure episode. Neurosurgery consultant opted for not removing the bullet.
Brain injury, Bullet, Spontaneous migration
Gunshot head injuries are the most lethal types of the cranial traumas, frequently mortal. The mortality rate has been reported as ranging from 51 to 84% [1]. Factors that affect mortality include bullet velocity, distance of trajectory, expansive behavior, caliber, bullet migration, degree of initial brain damage and initial vascular injury [2]. One of the most important predictors of clinical outcome is the Glasgow Coma Scale (GCS) score of the patient at the time of the initial evaluation [1]. Bullet injuries to head need special attention in view of the ballistics and requirement of prompt decisions regarding surgical removal. The neurological status at time of presentation and the location of the bullet most often dictates the decision regarding surgical removal. However, an important though uncommon complication of retained missiles is that of spontaneous migration [3], being caused by understood mechanisms like gravity and primary wound tract effect. This phenomenon has been reported to occur in 0.06-4.2% of cases [4]. First described in 1916, the complications resulting from bullet migration are unpredictable [5]. Should a bullet move into a particularly important eloquent region of the brain, the neurologic sequelae may be devastating. In addition, movement in and of itself may suggest a complication, such as abscess formation or acute rehemorrhage. A migrating (and likely positionally unstable) bullet must be notified to the rehabilitation consultant during inpatient or outpatient rehabilitation to avoid further unusual complications of bullet migration [5]. We report a case of spontaneous migration of bullet in different directions, managed non-surgically due to good clinical state, and review the relevant literature.
A 23-year-old male admitted with firearm injury to his head in the left occipital region by a friend while playing video games. In his physical examination, there was a single entry wound situated on the left side of the occipital bone, the exit wound could not be found. In the first neurological examination, the patient had headache and GCS at the time of admission was 14. Pupils were equally reactive, and his vitals were stable. On physical exam, he was awake and alert, in no apparent distress. Patient had no speech disorders neither cognitive or ambulation impairment. The only symptom was right hemianopsia. Cranial computerized tomography (CT) (Figure 1) revealed gunshot wound through the posterior left parietal cranium and the underlying left parietal lobe, resulting in a comminuted fracture with multiple bone fragments and metal fragments within the left posterior parietal lobe. A metallic bullet (13.9 mm L × 10 mm T × 13.2 mm AP) within the left posterior parietal parenchyma and moderate volume subarachnoid hemorrhage throughout the parieto-occipital region. It also demonstrates few punctate foci of intraparenchymal contusions within the left parieto-occipital region and small volume left posterior parietal subdural hematoma. The entry wound was debrided and sutured. The patient was treated conservatively with antibiotics, antiepileptics, and anti-edema drugs.
 Figure 1: First CT revealed gunshot wound through the posterior left parietal cranium and the underlying left parietal lobe, resulting in a comminuted fracture with multiple bone fragments and metal fragments within the left posterior parietal lobe. A metallic bullet within the left posterior parietal parenchyma. A) Axial bone window; B) Sagittal brain window; C) 3D VR.
View Figure 1
Figure 1: First CT revealed gunshot wound through the posterior left parietal cranium and the underlying left parietal lobe, resulting in a comminuted fracture with multiple bone fragments and metal fragments within the left posterior parietal lobe. A metallic bullet within the left posterior parietal parenchyma. A) Axial bone window; B) Sagittal brain window; C) 3D VR.
View Figure 1
Repeat CT four days later after a single episode of seizure revealed bullet migration posteriorly, likely gravity directed within the injury track in the bed-ridden patient. Within the bullet tract, there is significant interval ballooning of intraparenchymal hemorrhage involving the medial posterior left frontal lobe and left parietal lobe. Three days later (one week after initial injury) the bullet has moved anteriorly appearing next to the left ventricular atrium (Figure 2). Two weeks later on initial follow up the bullet appeared in the anterior margin of the cistern of the lamina terminalis, along the medial surface of the left frontal lobe next to the frontal horn of the left lateral ventricle (Figure 3). Two weeks later (one month after initial injury) the bullet migrated medially and downwards, lodged in the left paramedian anterior cranial fossa floor under the left gyrus rectus, superior to the posterior cribriform plate margin (Figure 4). The patient was conscious with a right hemianopsia but no other eloquent neurologic deficit, even after his single seizure episode. The patient was discharged from the hospital after one month of observation. Surgical intervention was not considered, as the patient displayed no new neurological deficit during the follow-up. He was managed conservatively, no recurrent seizures reported. As he remained asymptomatic, continued conservative observation of this bullet was recommended. However, if he does have symptoms, including visual disturbances or uncontrollable seizures, and the bullet appears to be stable in position, retrieval may be an option in the future if he is symptomatic. He is now doing well and has made a great recovery (Figure 5 and Figure 6).
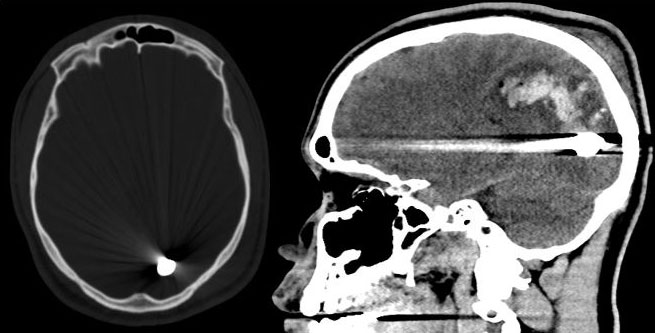 Figure 2: CT four days later after a single episode of seizure revealed bullet migration posteriorly. Within the bullet tract, there is significant interval ballooning of intraparenchymal hemorrhage involving the medial posterior left frontal lobe and left parietal lobe.
View Figure 2
Figure 2: CT four days later after a single episode of seizure revealed bullet migration posteriorly. Within the bullet tract, there is significant interval ballooning of intraparenchymal hemorrhage involving the medial posterior left frontal lobe and left parietal lobe.
View Figure 2
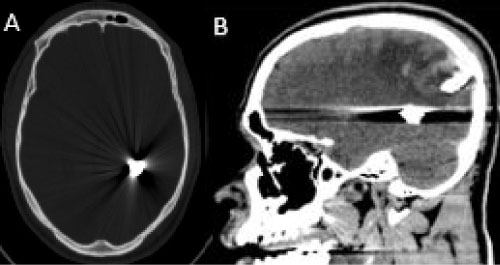 Figure 3: One week CT, the bullet has moved anteriorly appearing next to the left ventricular atrium. A) Axial bone window; B) Sagittal brain window.
View Figure 3
Figure 3: One week CT, the bullet has moved anteriorly appearing next to the left ventricular atrium. A) Axial bone window; B) Sagittal brain window.
View Figure 3
 Figure 4: Two week CT, the bullet appeared in the anterior margin of the cistern of the lamina terminalis, along the medial surface of the left frontal lobe next to the frontal horn of the left lateral ventricle. A) Axial bone window; B) Sagittal brain window.
View Figure 4
Figure 4: Two week CT, the bullet appeared in the anterior margin of the cistern of the lamina terminalis, along the medial surface of the left frontal lobe next to the frontal horn of the left lateral ventricle. A) Axial bone window; B) Sagittal brain window.
View Figure 4
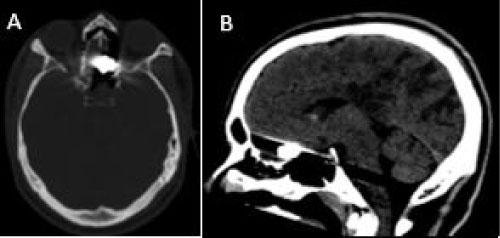 Figure 5: One month CT, the bullet migrated medially and downwards, lodged in the left paramedian anterior cranial fossa floor under the left gyrus rectus, superior to the posterior cribriform plate margin A) Axial bone window; B) Sagittal brain window.
View Figure 5
Figure 5: One month CT, the bullet migrated medially and downwards, lodged in the left paramedian anterior cranial fossa floor under the left gyrus rectus, superior to the posterior cribriform plate margin A) Axial bone window; B) Sagittal brain window.
View Figure 5
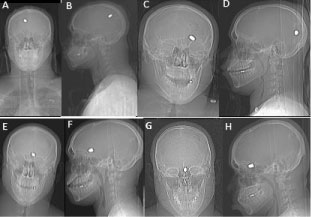 Figure 6: RX showing the position of the bullet. A) First day front; B) Sagittal projection; C) One week front; D) Sagittal projection; E) Two weeks front; F) Sagittal projection; G) One month front; H) Sagittal projection.
View Figure 6
Figure 6: RX showing the position of the bullet. A) First day front; B) Sagittal projection; C) One week front; D) Sagittal projection; E) Two weeks front; F) Sagittal projection; G) One month front; H) Sagittal projection.
View Figure 6
Firearm injuries have been studied in different settings and countries with different incidence, outcome, and management outlines. Although migration of an intracranial projectile is an uncommon condition, severity of complications associated with such events often contributes to poor prognostic implications [3]. The understanding of physics of missile injury explains the difference in severity and clinical presentation, the type of weapon and trajectory of bullet before and after brain penetration being the most likely distressing factors [6]. Penetrating brain injury from a high-velocity projectile creates a complex pattern of permanent tissue damage. The bullet track left in the wake of the missile creates a potential nidus for foreign body migration, local brain necrosis, and external contamination of devitalized wound tissues [7]. The management of these injuries needs to be studied in detail in order to intervene during the course of the treatment at the right moment. Removal of the bullet should be done for patients undergoing surgery for wound debridement or evacuation of intra or extra-axial fluid collection provided the bullet is in the vicinity and easily accessible. Removal should not lead to further deterioration in the neurological status due to its proximity to vital structures [3].
The presence of a bullet or metal missile fragment as a foreign body is associated with several complications, such as meningitis, abscess formation, CSF fistula, epilepsy, hematoma, hydrocephalus, altered level of consciousness, and confusion [7]. Secondary sequelae such as abscess formation, ventriculitis, focal seizures or migration are further indications warranting surgical intervention. Spontaneous migration of the projectile in the cerebral parenchyma is a rare complication of bullet injuries [3].
The first radiographic documentation of migration of a bullet in the brain was published in 1916. More recent case reports show that migration has been shown to be a relatively rare occurrence. Martin and Campbell 12 found five cases of migration in their series of 426 cases of penetrating head injuries [5].
The time course for migration ranges from 2 days to 3 months [8]. There are several hypotheses explaining the mechanism of migration of a retained metallic fragment within brain tissues. Higher gravidity of the bullet in comparison to the brain tissue, pulsatile force of the brain and cerebrospinal fluid (CSF), and softening of the brain tissue through fragment trajectory are among the most common mechanisms [7]. The movement of a bullet in the nervous system occurs mainly due to gravitational forces. Gravitational force acting on the bullet, which is denser than the surrounding medium, has been suggested as a cause for migration caudally by the effect of gravity related to the position of the body, especially in the absence of significant cranial swelling. Cerebrospinal fluid (CSF) flow and pulsation can also facilitate the bullet’s movement within the ventricles. Bullets reaching the CSF may migrate to a distant part of the brain or the spinal canal through the CSF. Penetration of the bullet leads to destruction in the white matter part of the parenchyma. This type of migration has been attributed to cerebral softening secondary to edema and local tissue damage, specific gravity of the bullet and gravitational factors. Bullets that cannot move within the brain after an initial movement are presumably walled off by gliosis and fibrotic scarring. These processes usually take from weeks to years.
Reports have described projectiles moving above, below, and through a defect in the tentorium cerebell, passing through the tentorial incisure, and moving inside the spinal canal and thecal sac. Overall, intact bullets, copper jackets, lead cores, and pellets can migrate through the body. Rapp, et al. [4] reviewed 213 neurosurgical patients with GSWs of the head and estimated that approximately 4.2% of the bullet fragments migrated; the earliest migration of a bullet fragment was discovered 36 hours post injury. Moreover, other authors have found that < 0.1% to 10% of bullets migrate inside the head [7,9,10].
In our case, cranial CT taken 4 days after the injury revealed that the bullet had migrated towards the left posterior occipital lobe when compared to the previous location, with caudal and posterior migration. In this case, movement of the intracranial bullet was ascribed to the specific gravity of the bullet, brain softening with loss of tissue resistance, white matter devitalization, and gravitational factors; however, gravity appears to be the most important factor responsible for the migration of the bullet [8]. The bullet migration continued but in the opposite direction till on one month the bullet was seen lying in the left paramedian gyrus rectus region, superior to the posterior cribriform plate. We think the migration of the bullet in this case was through the subarachnoid space due to pulsatile force of the brain and cerebrospinal fluid (CSF).
The indications for removal of an intracranial retained bullet are controversial and present a dilemma to the neurosurgeon [8]. Surgical treatment of bullet injuries needs to be decided on individual basis with intraoperative localization being essential. The management of these injuries needs to be studied in detail during the treatment procedure. Özkan and colleagues [5] advised that a bullet in the brain should be removed if it can be reasonably accessed and if it can be removed without causing additional neurological damage. Kumar, et al. [3] reported that removal of the bullet should be done in patients undergoing surgery for evacuation of a hematoma if it is easily accessible and removal does not lead to further deterioration of the neurological status due to its proximity to vital structures. Fujimoto, et al. [11] stated that presence of a retained bullet and bone fragments do not increase the rate of intracranial infection; therefore, in an effort to prevent infection, removal of the bullet is not necessary. Zafonte, et al. [5] reported two cases with neurological deterioration from spontaneous migration of a bullet; postoperatively, the patients demonstrated significant functional recovery. The study of Fujimoto noted that a bullet within the ventricular system should be removed because hydrocephalus can be caused by obstruction of the foramen of Monro or aqueduct of Sylvius; however, a bullet within the brain parenchyma should be removed only when it can be easily accessed. Intracranial retained bullets require neurological observation and serial CT because migration may result in additional neurological deficits, and removal of the migrated bullet is thus advisable [8]. Surgery tends to achieve debridement of devitalized tissue, removal of bone fragments, hemostasis, dural closure, and suturation of the entrance and exit wounds. In addition, antiepileptic and anti-edema agents and antibiotics should be administered [8]. Moreover, a retained bullet may cause potential complications, such as ventriculitis, toxicity, epilepsy, migration and hydrocephalus, which warrant surgical intervention. Migration of bullets may be also associated with abscess formation, which may be the result of skull or extracranial fragments propelled into the brain parenchyma by the force of the bullet [5]. However, removal of the bullet may cause iatrogenic damage to the brain parenchyma; therefore, if there is no evidence of infection or brain abscess formation or of additional neurological deficit during hospitalization, conservative management can be preferred [8].
In conclusion, the decision of surgical treatment of a bullet injury is difficult if it is in close proximity to vital structures, since removal of the bullet may cause significant neurological damage. However, despite it is a rare complication, we have to know there is a probability of spontaneous migration of the projectile in the cerebral parenchyma as it can sometimes lead to a worsening of the neurological status of the patient.