We presented a unique case of infantile type hemangioma corresponding with aortic stenosis. Therefore, we accepted this case as a PHACES syndrome. This case will be the 4th case of the literature. The most remarkable feature of PHACE syndrome is infantile hemangioma but abnormalities in the arteries which are not obvious on the clinical examination have considerable potential morbidity. We have certain diagnosis with pathology and no conflicts of interest disclosure.
Infantile hemangioma, Phaces syndrome, Posterior fossa hemangioma, Aortic stenosis
COVID-19: Corona virus disease-2019; GLUT-1: Glucose transporter-1; H: Hour; ICU: Intensive care unit; Kg: Kilogram; Mg: Milligram; MRA: Magnetic resonance angiography; MRI: Magnetic resonance imaging; PHACES: PHACE syndrome is an acronym of (Posterior fossa malformations, hemangioma, arterial anomalies, coarctation of aorta/cardiac defects, eye abnormalities); SMA: Smooth muscle actin
The most prevalent benign neoplasm of infancy is the infantile hemangioma [1] with an incidence of 5-10% in pediatric population [2]. These tumors usually do not present with systemic involvement. Primarily located in extracranial locations such as skin, whereas intracranial hemangiomas less frequently observed pathologies. We presented a unique case of posterior fossa hemangioma with aortic stenosis in a one-year-old infant. Including aortic stenosis as an aortic defect with a posterior fossa hemangioma we can count this condition as a PHACE syndrome. The most remarkable feature of PHACE syndrome is infantile hemangioma but abnormalities in the arteries which are not obvious on the clinical examination have considerable potential morbidity [3,4]. PHACE syndrome is an acronym of (Posterior fossa malformations, hemangioma, arterial anomalies, coarctation of aorta/cardiac defects, eye abnormalities). First described in 1978, by Pascual-Castroviejo [5]. In 1996, Frieden, et al. created acronym [6]. Subsequently, sternal malformations were added the acronym and became PHACES [7].
A one-year-old infant as a close follow-up patient of our hospital's pediatric cardiology department with an aortic stenosis planning a balloon-valvuloplasty. He was admitted pediatric emergency service with a 2-day onset of right hemiparesis without any traumatic injury. According to the patient's perinatal and medical history, he was born after 39 weeks pregnancy with a birth weight of 3125g. There was no positive family history of hemangiomas. On examination, he was awake, alert, positive pupillary reflexes, no facial paresis, with a 4/5 right hemiparesis. Neither syncope nor seizure was happened. The ophthalmological evaluation showed that both eyes were equal in size and eye motility was normal. No any symptoms of acute hydrocephaly and has subfebril fever of 37.8 °C, without neck stiffness.
Blood tests were evaluated, and no pathologic value was seen. Magnetic resonance imaging (MRI) and angiography (MRA) was obtained which revealed a pontin mass along the dorsal aspect of the posterior fossa. The lesion is heterogeneously hyperintense on T1 and T2 weighted sequences (Figure 1 and Figure 2). The mass was well-circumscribed and heterogeneous, and evidence of previous hemorrhage within it. He was consulted to our department with preliminary diagnosis of pontine cavernoma and hemangioma. The differential diagnoses of an intracranial vascular lesion in this one year-day old infant included hemangioma, hemangioblastoma, vascular malformation, and other neonatal tumor types, such as soft-tissue sarcoma [8].
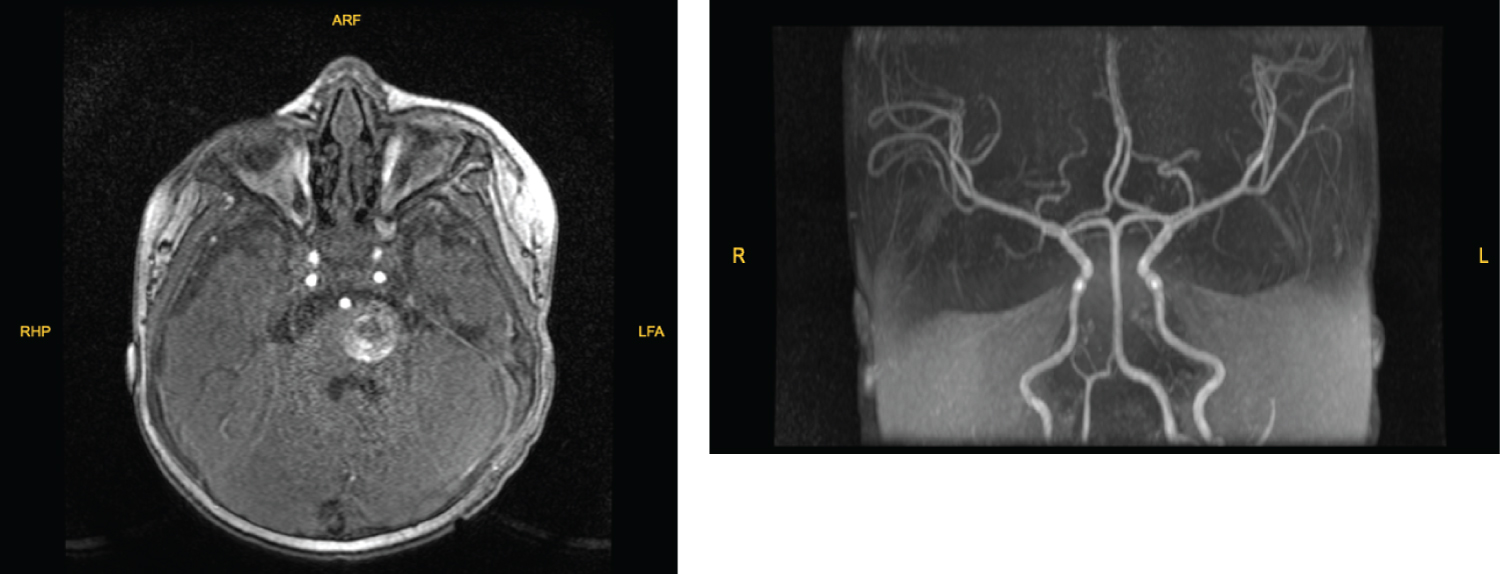 Figure 1: MR angiography showed a non-vascular lesion narrowing forth ventricle on the left part of pons. View Figure 1
Figure 1: MR angiography showed a non-vascular lesion narrowing forth ventricle on the left part of pons. View Figure 1
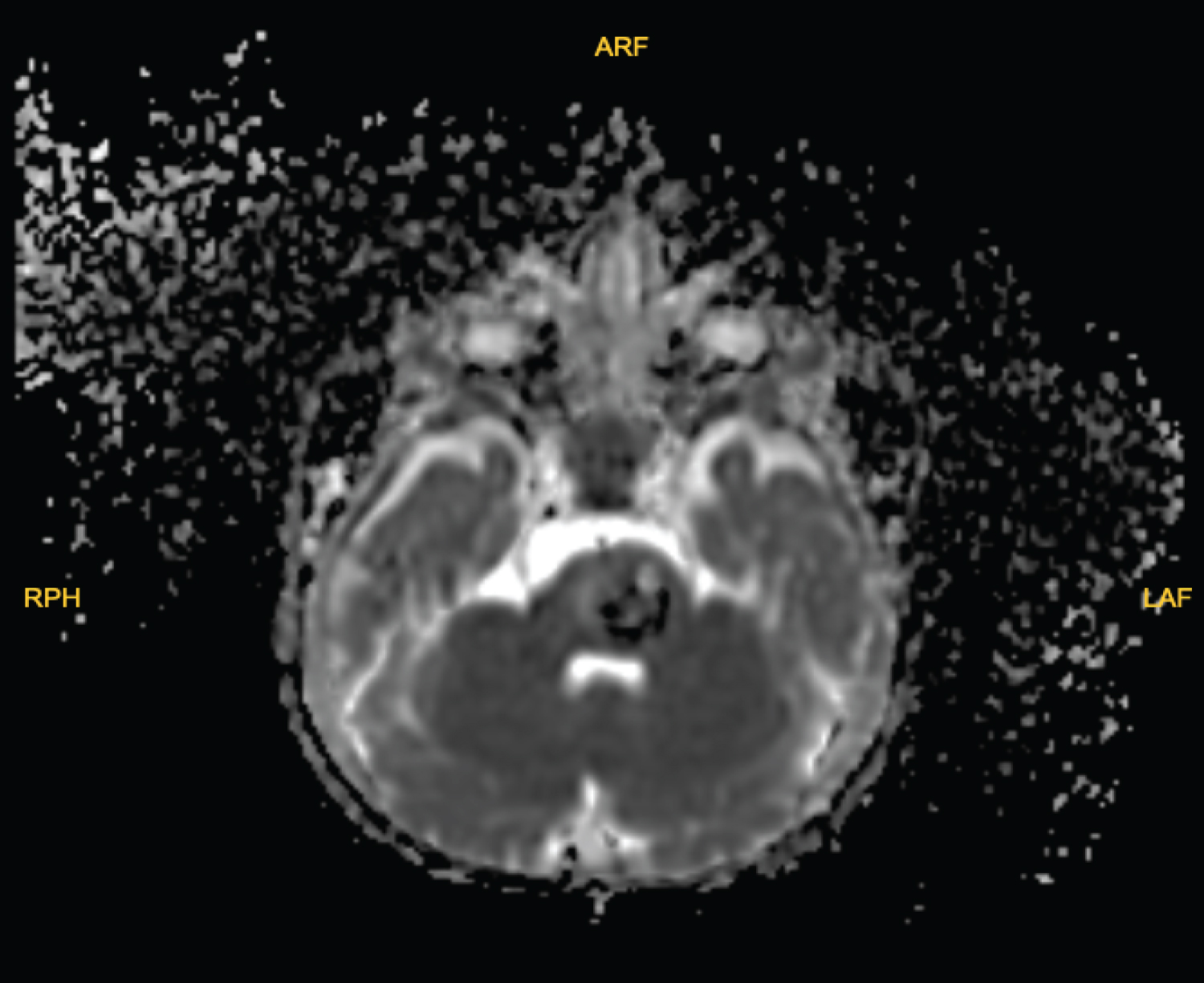 Figure 2: Diffusion sequence of the lesion. View Figure 2
Figure 2: Diffusion sequence of the lesion. View Figure 2
He was required hospitalization with focal neurologic deficit and admitted to pediatric ICU service to complete preoperative studies. After 12 hours of admission, our team was ready for surgery but on the operation table he has fever of 38.5 °C anesthesia wanted to exclude COVID-19 infection and sent him back to ICU. Blood cultures and urine cultures were made and nasopharyngeal swab culture for COVID-19 was sent to the public health laboratory of Turkish Health Ministry. Prophylactic antibiotics were started. Tests were revealed after 2 days and showed no infection and his fever was improved. 2 days later we operated patient. A suboccipital craniectomy was performed. The lesion appeared vascular and clearly separated from the normal glial tissue without involvement. Because of the patient's size and the low circulating blood volume, minimizing blood loss was imperative. Blood products were on standby but neither of was used. Hemangioma was gross totally resected and no complication was made. After surgery to exclude intracranial hemorrhage, a diffusion MRI was obtained and revealed the lesion was totally resected. No hemorrhage was seen (Figure 3 and Figure 4). On his post-operative day 1, his hemiparesis was 4+/5 but had a facial paresis so we immediately started 2 mg/kg/h prednisolone and continued for 24 hours. In his post-operative day 2, his facial paralysis was recovered and we stopped prednisolone infusion. He was transferred to infantile service, near his parents. We checked his neurologic examination on our daily routines and his right paresis was totally improved on post-operative day 5 and he discharged with outpatient polyclinic control.
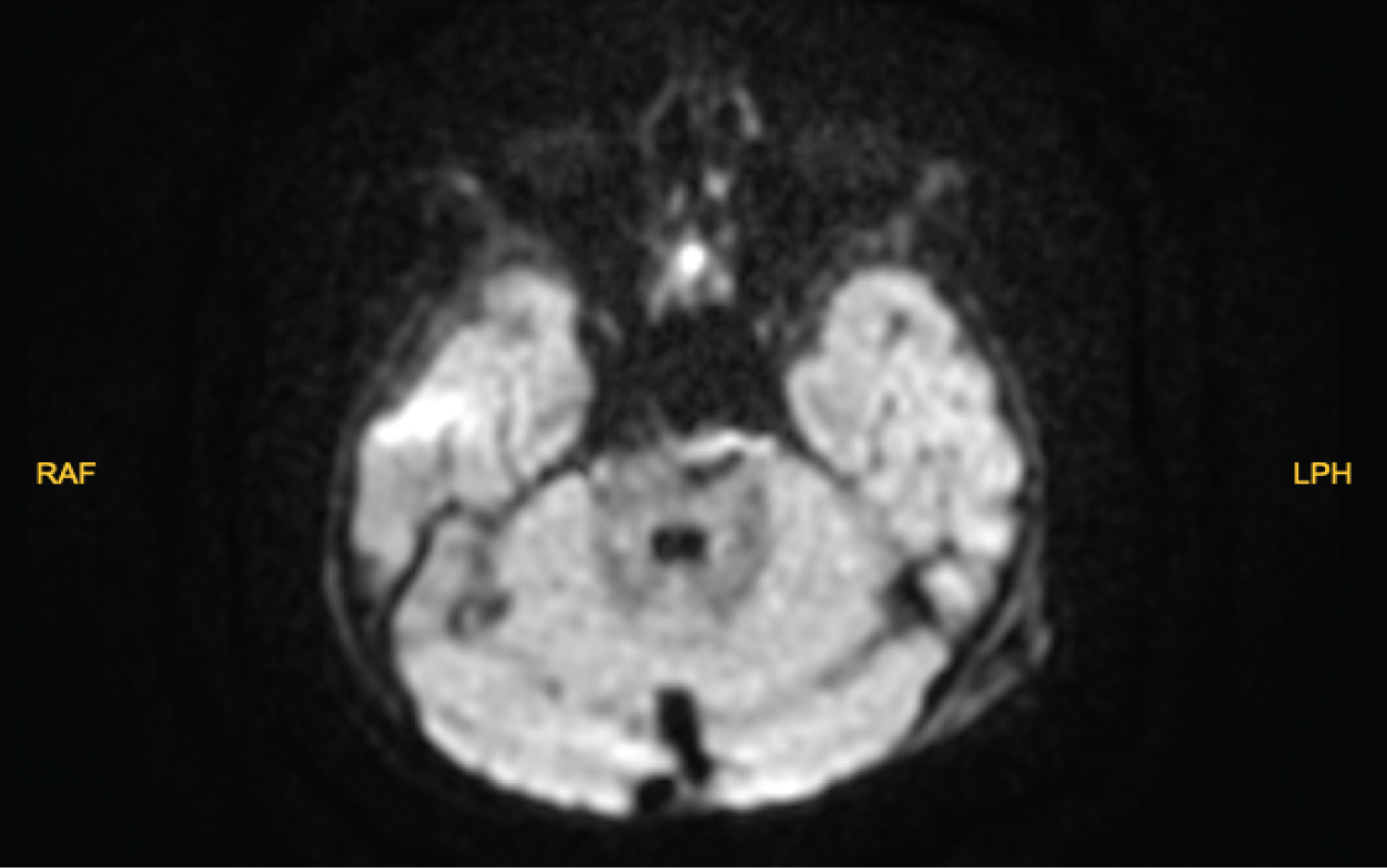 Figure 3: Postoperative 24 hour MRI, no hemorrhage was seen on the MRI. View Figure 3
Figure 3: Postoperative 24 hour MRI, no hemorrhage was seen on the MRI. View Figure 3
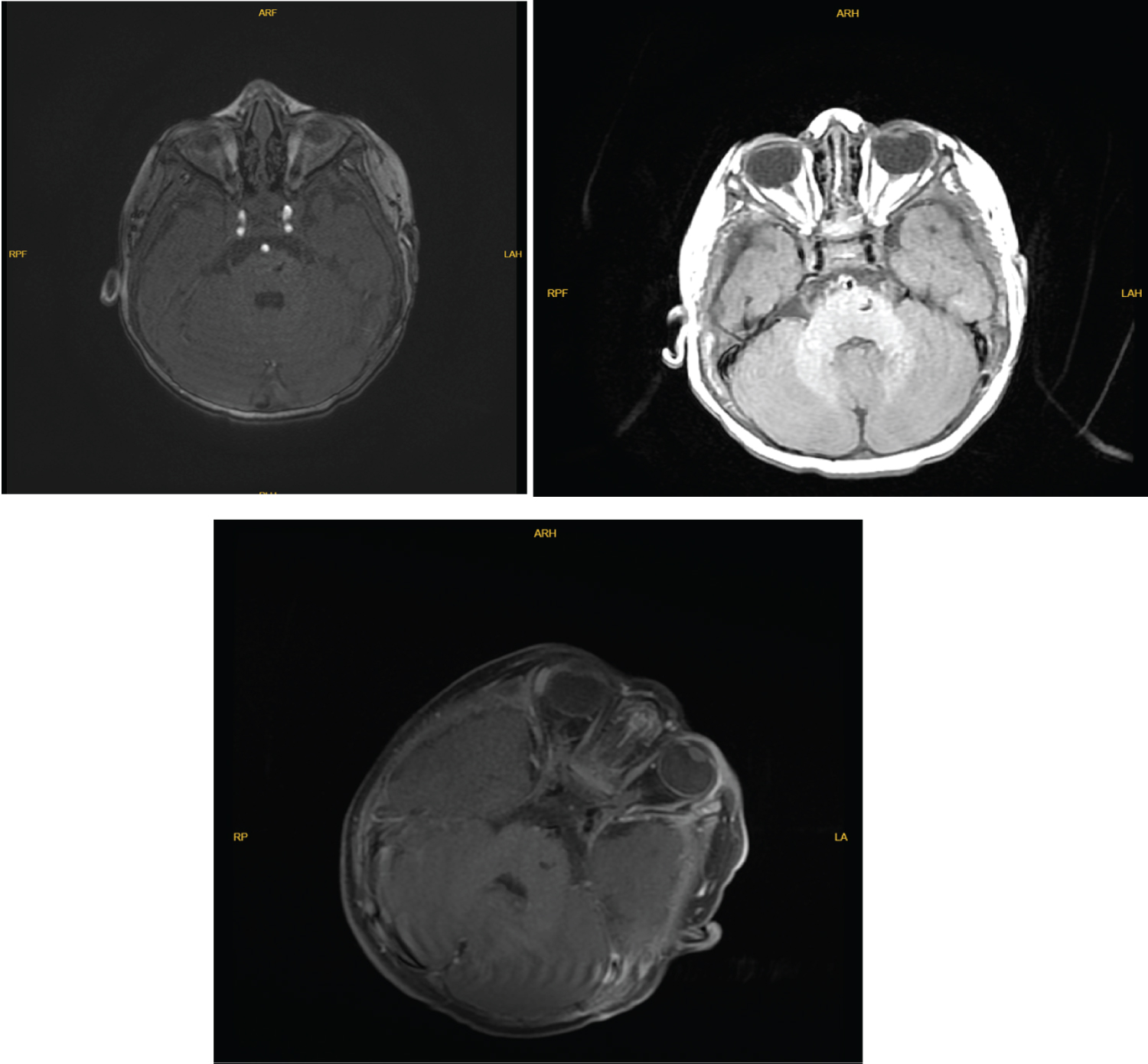 Figure 4: Postoperative Day 30 control MRI, lesion was totally removed. T1, TOF and T2 flair sequences of MRI images. View Figure 4
Figure 4: Postoperative Day 30 control MRI, lesion was totally removed. T1, TOF and T2 flair sequences of MRI images. View Figure 4
On his post-operative day 12 we took sutures and no cerebral spinal fluid collection was seen. We planned a control magnetic resonance angiography and obtained in his post-operative day 30 (Figure 4). No residue lesion was revealed.
One percent of infantile hemangiomas involve the central nervous system, and approximately half of these are intracranial [8]. Most intracranial infantile hemangiomas classically involve the extra-axial basal cisterns, subarachnoid and ventricular spaces, and cavernous sinus [9]. Our case was demonstrating classically findings of infantile hemangiomas (Figure 5), but confirmation of hemangioma was made by immunohistochemical staining. Pathologic specimen was positive staining with GLUT1 and SMA which are reliable markers for infantile hemangioma. GLUT1 (Figure 6 and Figure 7), a glucose transporter present in normal capillary endothelial cells constituting the blood-brain barrier, is a particularly useful marker of infantile hemangiomas because it differentiates those from other vascular tumors and malformations that have been shown to lack GLUT1 [10]. Several other associated abnormalities have been observed in infants with infantile hemangioma, including arterial anomalies, ipsilateral cerebellar hypoplasia, Dandy-Walker malformation, Moya Moya-like proliferation of the internal carotid artery terminus [11] (Figure 6 and Figure 7).
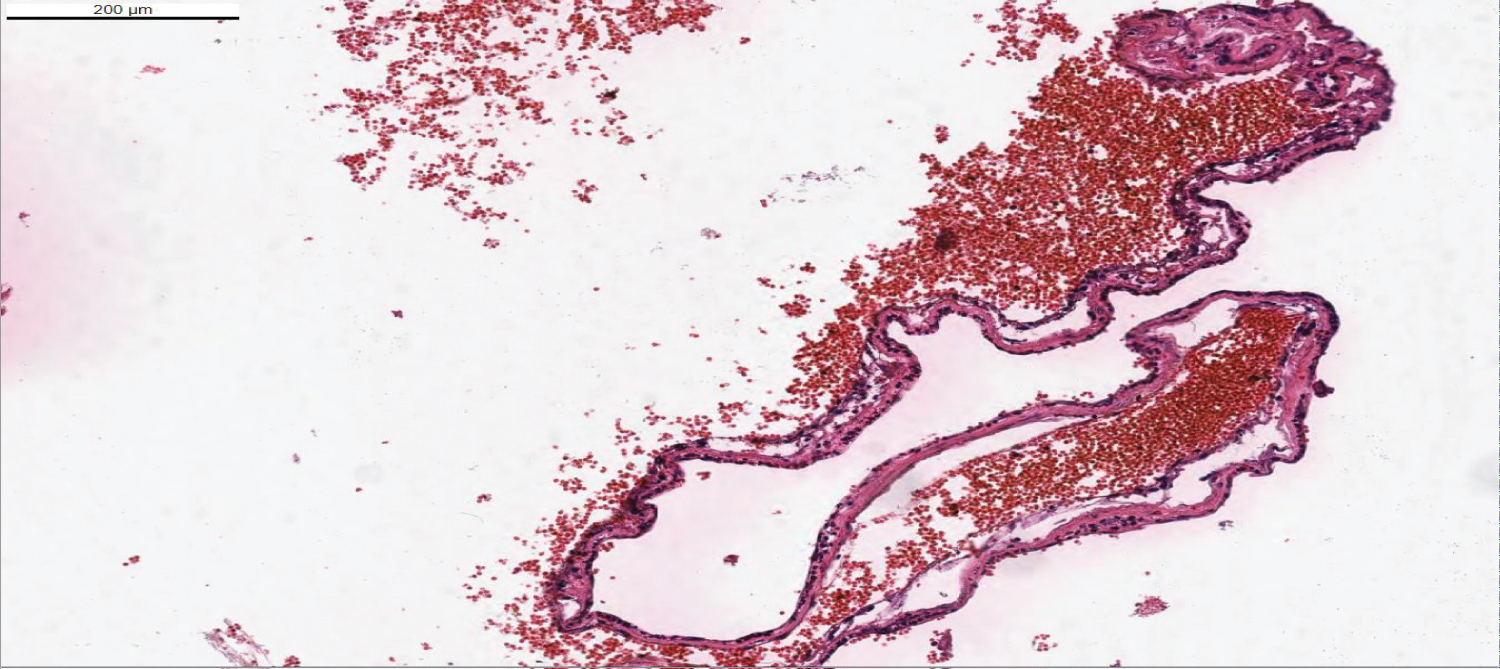 Figure 5: Pathology prepared slides showed congested vascular lesions which has thin walls with hematoxylin eosin dye. View Figure 5
Figure 5: Pathology prepared slides showed congested vascular lesions which has thin walls with hematoxylin eosin dye. View Figure 5
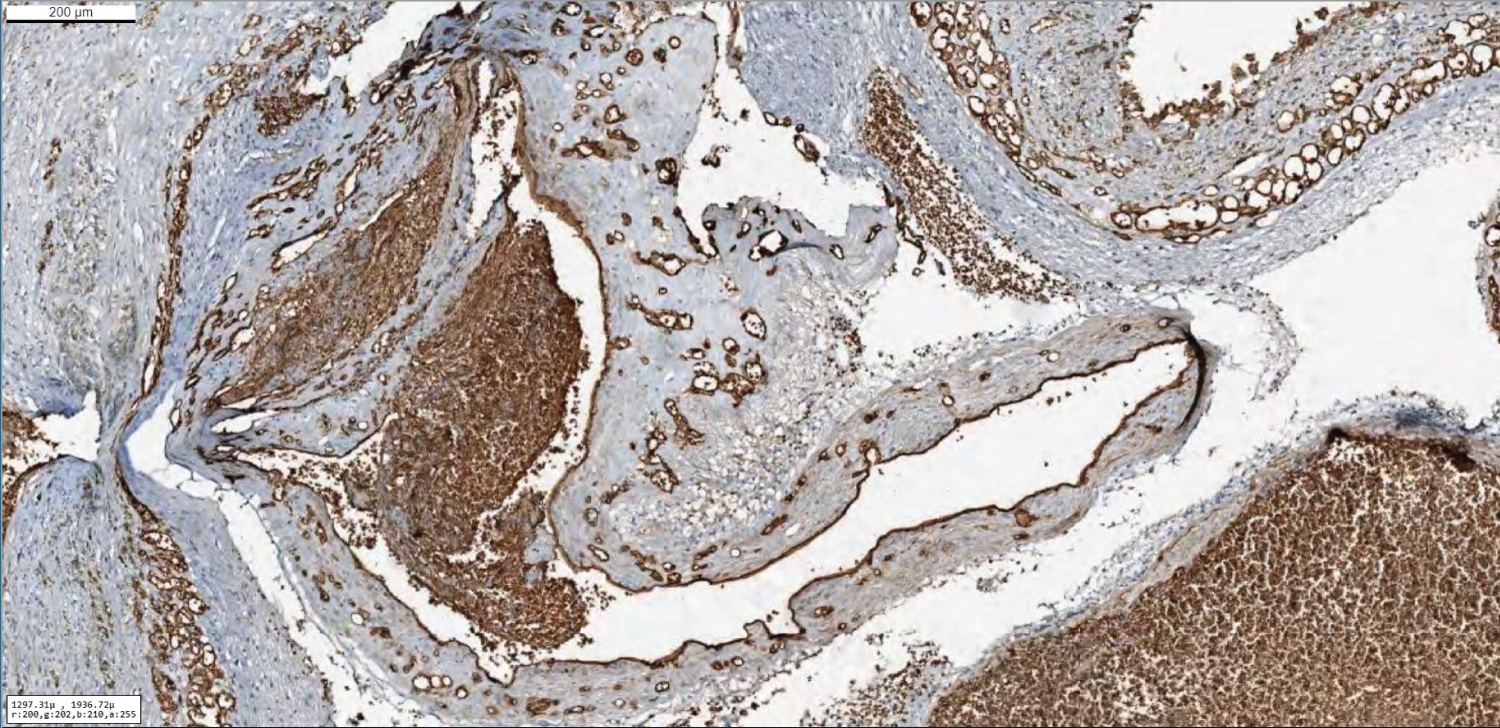 Figure 6: Hematoxylin Eosin dying of the pontine mass. Specimen showed a vascular lesion within slight walls. View Figure 6
Figure 6: Hematoxylin Eosin dying of the pontine mass. Specimen showed a vascular lesion within slight walls. View Figure 6
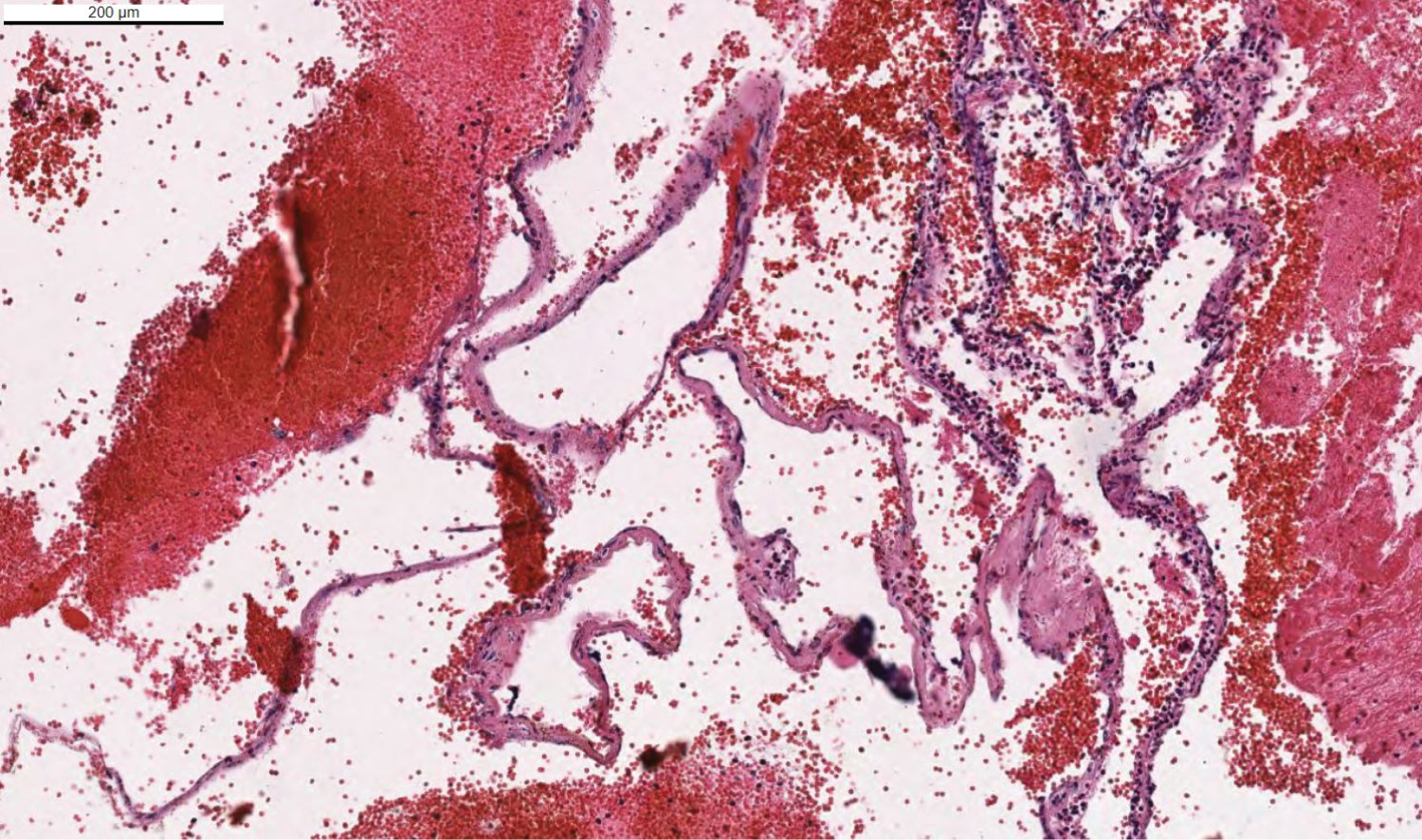 Figure 7: Immunohistochemically, Glut-1 dye showed expressions of the vascular wall and it's compatible with the infantile type hemangioma. View Figure 7
Figure 7: Immunohistochemically, Glut-1 dye showed expressions of the vascular wall and it's compatible with the infantile type hemangioma. View Figure 7
Despite the benign nature of infantile hemangioma, in our case patient has focal neurologic deficits because of the mass effect. These lesions can cause considerable and permanent injury to the developing brain. Therefore, intervention is required such as these mass effect lesions of infantile hemangiomas. Besides, Propanol is a common treatment protocol of infantile hemangiomas whereas extra-cranial lesions, there is no evidence of using it for intracranial lesions. On the other hand, as a second option of medical therapy steroids were generally use. Mostly using in benign skin lesions with biopsy confirmed. Regression of lesions were reported [1,8]. But also no evidence was found in the literature of using steroids for intracranial lesions. Embolization can be a additional therapy to surgical resection. But as an infant patient small vessel can be a handicap to make angiography without complication [11]. 3 of Dural-based infantile hemangiomas were reported in the literature [11]. Our case can be count for the 4th case of literature which was including PHASES symptoms (Table 1) [12].
Table 1: Case reports of Dural-based infantile hemangiomas Authors. View Table 1
We have no conflicts of interest to disclose.