Skull�s morphology, a complex anatomical structure, has been widely described by renowned neurosurgeons worldwide. Evolutionary changes, phenotype, and science describe specific changes in the human body that have not, to date, been studied in depth in forensic anthropological studies.
Objective: To measure and describe variations of craniometry in Peruvian specimens through the measurement of craniometric points.
Methods: The study was carried out with unknown skulls donated to the NeuroZone3D Research Center using a soft and inelastic measuring tape as a tool. In our report, direct anthropometric measurement technique with data collection by a single investigator was considered.
Results: The averages of Peruvian craniometric measurements were from nasion to bregma of 11.27 cm, bregma to lambda of 11.35 cm, lambda and inion was 6.78 cm, inion to opisthion of 4.61 cm, nasion to inion of 29.4 cm, opisthion to basion of 3.41 cm, bregma to stephanion of 6.94 cm, stephanion to pterion of 3.49 cm, pterion and asterion 10.5 cm. Craniometry data were generally lower than literature data.
Conclusions: Values of the Peruvian craniometry were lower compared to other studies; In addition, the findings reflect that comparison of data with different nationalities is necessary to determine diverse structural characteristics in the anatomy.
Craniometry, Skull, Anthropometry, Forensic science
The cranial morphology described by Andreas Vesalius in his texts brought about the most innovative thinking of the last millennium, precisely illustrating his depictions illustrations with pictorial precision [1]. Creativity and ingenuity of great masters in neuroanatomy were necessary to describe the craniometric points that we currently know [2,3].
Widely recognized evolutionary changes depict a significant shift in the primitive morphology of modern humans, as biological reorganization has given rise to distinct anatomical entities [4]. Similarly, specific traits of the human lineage, represented through phenotypes, have led to anatomical and physiological changes that enhance our understanding of our evolutionary origins [5].
Craniometric analysis is defined as the combination of descriptive and metric approaches that quantifies observable features in the skull [6]. Observation of the human skull, within the realm of neuroscience, has sparked numerous hypotheses throughout history [7]. Application of these measurements in medicine holds relevance for surgical specialties, neuroimaging, forensic expertise and anthropological research [8-11].
In recent years, cranial measurements in neurosurgery have become indispensable for locating complex brain pathologies, undertaking neurosurgical approaches to brain disorders, and identifying Brodmann areas [12,16].
The significance of anthropometric studies holds global importance in deepening our understanding of anatomy. Currently, there is scarcity of studies on cranial analysis of skulls within the Latin American population. This current study describes, for the first time, craniometry in Peruvian cadaveric specimens, which will serve as a valuable source of information to establish normal values in our country.
Not applicable, in this study all specimens represents donations to NeuroZone3D Research Center.
The study sample is composed of ten cadaveric specimens extracted from institutional osteological collections in Peru. The vast majority represents donations to the initiative of the NeuroZone3D Research Center; the origin of each specimen is of a different geographical origin.
For the study's purposes, the NeuroZone3D Research Center and its collaborators classified the ten specimens without distinguishing by age and gender, given the complexities in tracking and the absence of evidence to demonstrate these features.
Conventional measurement techniques were used with a soft inelastic tape measure (Perfect Measuring Tape Company, USA). Each skull was evaluated by a single researcher Christian A. Yataco Wilcas, points were defined by the standardized nomenclature of osteometry, also assisted by the other authors [17]. Each definition, craniometry measurement, abbreviation and identification of the specimens used in the study is presented in Table 1, Table 2, Figure 1 and Figure 2.
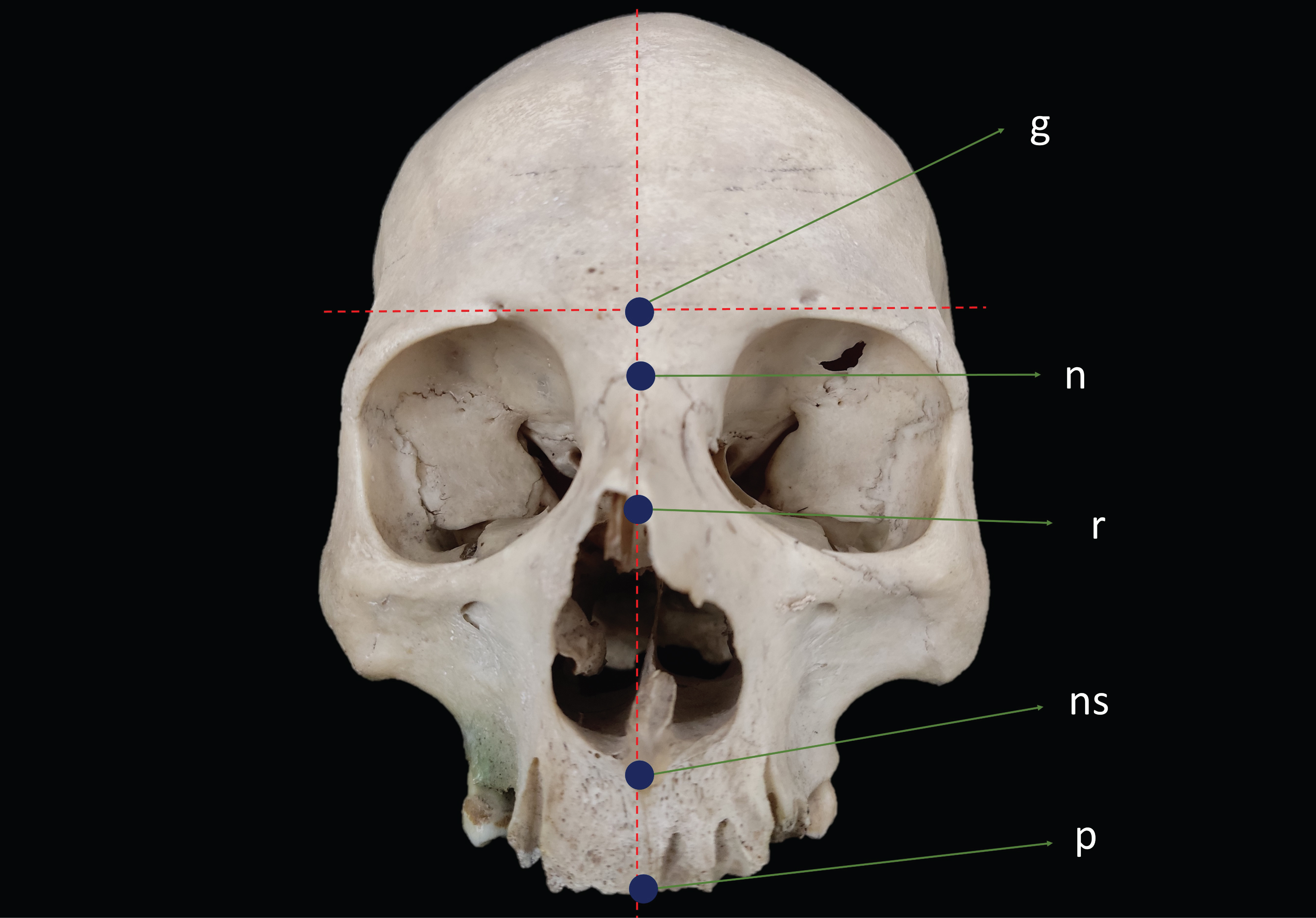 Figure 1: Anterior view of the Peruvian skull from medial craniometric points.
g: Glabella; n: Nasion; r: Rhinion; ns: Nasospinale; p: Prosthion
View Figure 1
Figure 1: Anterior view of the Peruvian skull from medial craniometric points.
g: Glabella; n: Nasion; r: Rhinion; ns: Nasospinale; p: Prosthion
View Figure 1
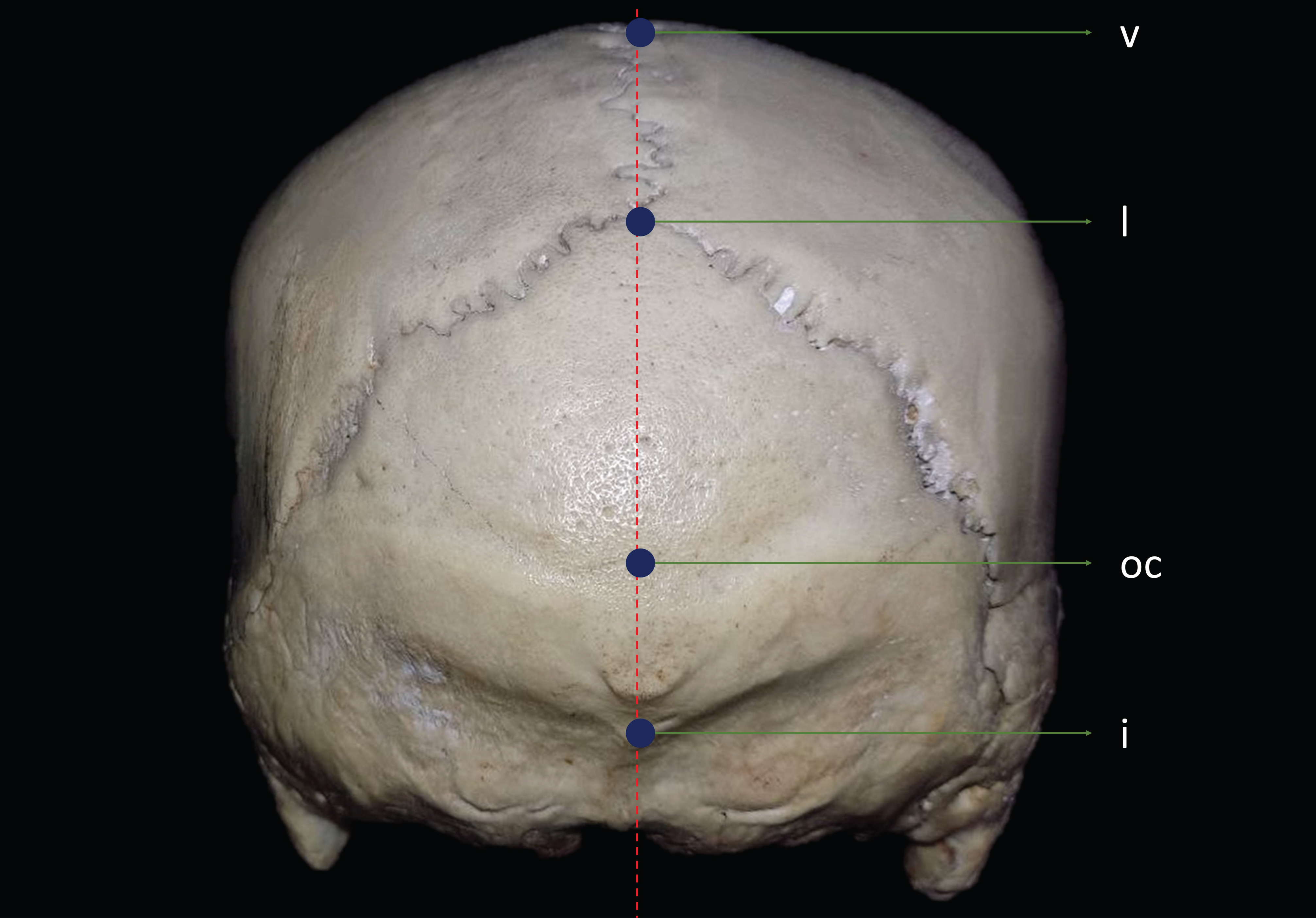 Figure 2: Posterior view of the Peruvian skull from medial craniometric points.
Figure 2: Posterior view of the Peruvian skull from medial craniometric points.
v: Vertex; l: Lambda; i: Inion; oc: Opisthocranion
View Figure 2
Table 1: Definition and abbreviation of craniometric points (Adaptation Caple 2015). View Table 1
Table 2: Medial and lateral craniometric measurements. View Table 2
The results of craniometric measurements are presented as mean, median, standard deviation, minimum values, and maximum values. The normality of the data of right and left hemicranium was evaluated using the Shapiro-Wilk test. Homogeneity of variance was evaluated with the Levene test. The level of significance was accepted as p < 0.05.
The evaluation of each specimen of the present study was collecting data three times to reduce measurement errors. The measurement began with bilateral craniometric points of the right hemicranium, continuing with the left hemicranium, followed by medial craniometric points, ending with the inferior face of the skull (Figure 3 and Figure 4).
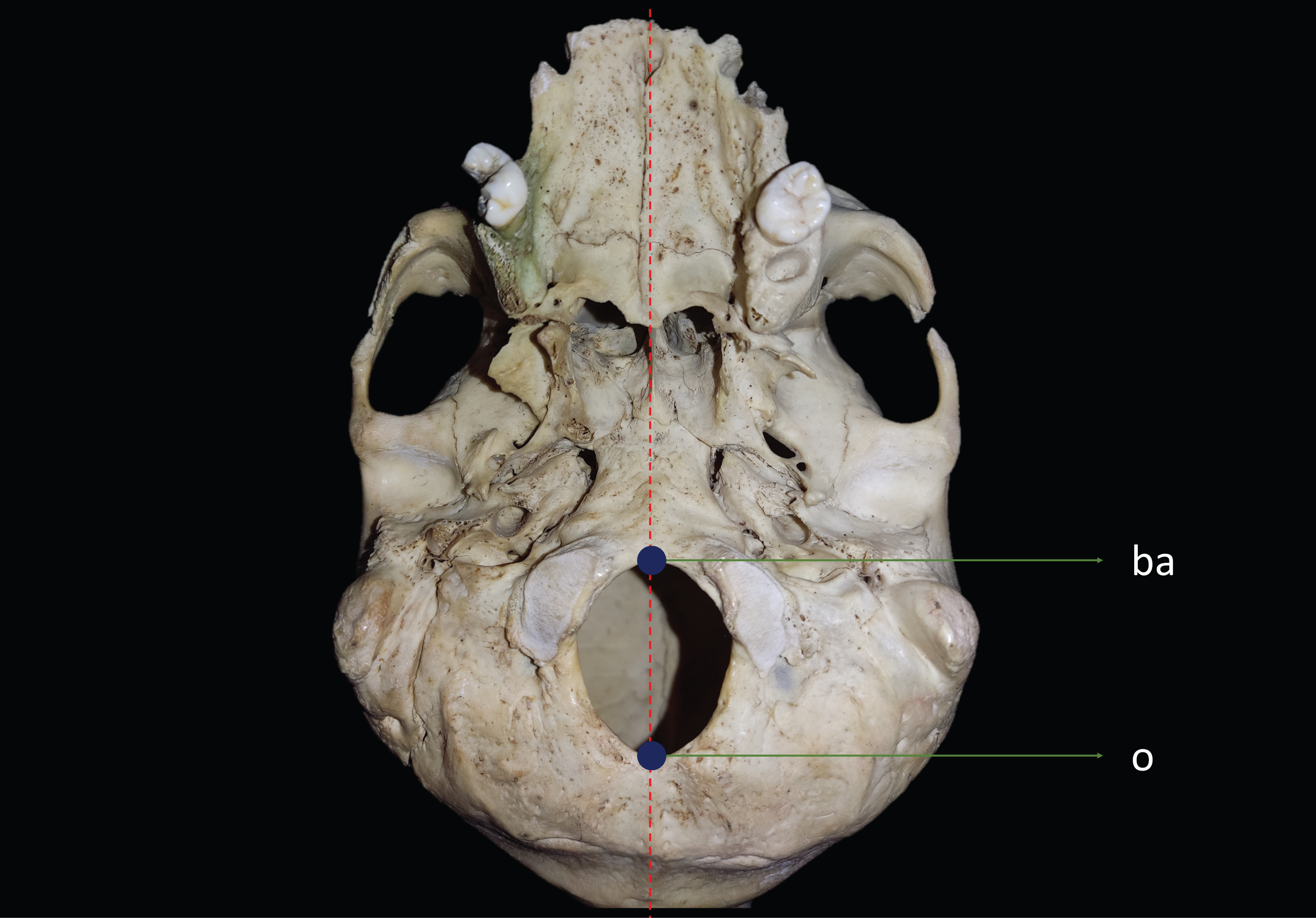 Figure 3: Inferior view of the Peruvian skull from medial craniometric points.
Figure 3: Inferior view of the Peruvian skull from medial craniometric points.
b: basion; o: Opisthion
View Figure 3
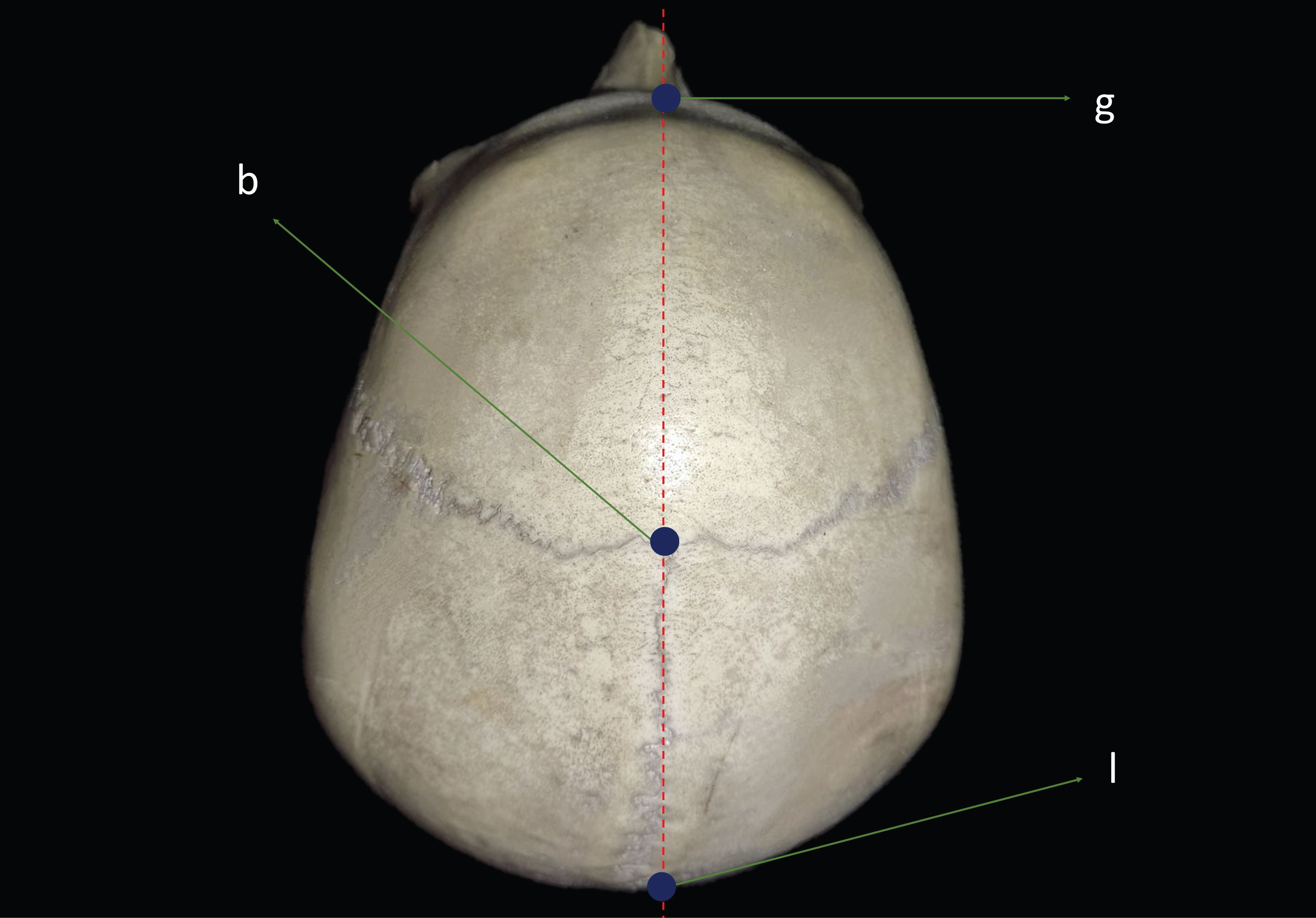 Figure 4: Superior view of the Peruvian skull from medial craniometric points.
Figure 4: Superior view of the Peruvian skull from medial craniometric points.
g: Glabella; b: Bregma; l: Lambda
View Figure 4
Measurements of bilateral craniometric points; bregma-stephanion-pterion and pterion-asterion did not have a statistically significant difference between the measurements of right and left hemicranium, since they showed a normal and homogeneous distribution with a p value > 0.05 (Table 3, Figure 5 and Figure 6). Therefore, the authors decided to choose the measurements obtained in the right hemicranium as analysis. The craniometric measurements of the Peruvian sample are described in Table 4. The mean values ± standard deviation and quiartiles of the craniometric measurements used in our study are shown in Table 5.
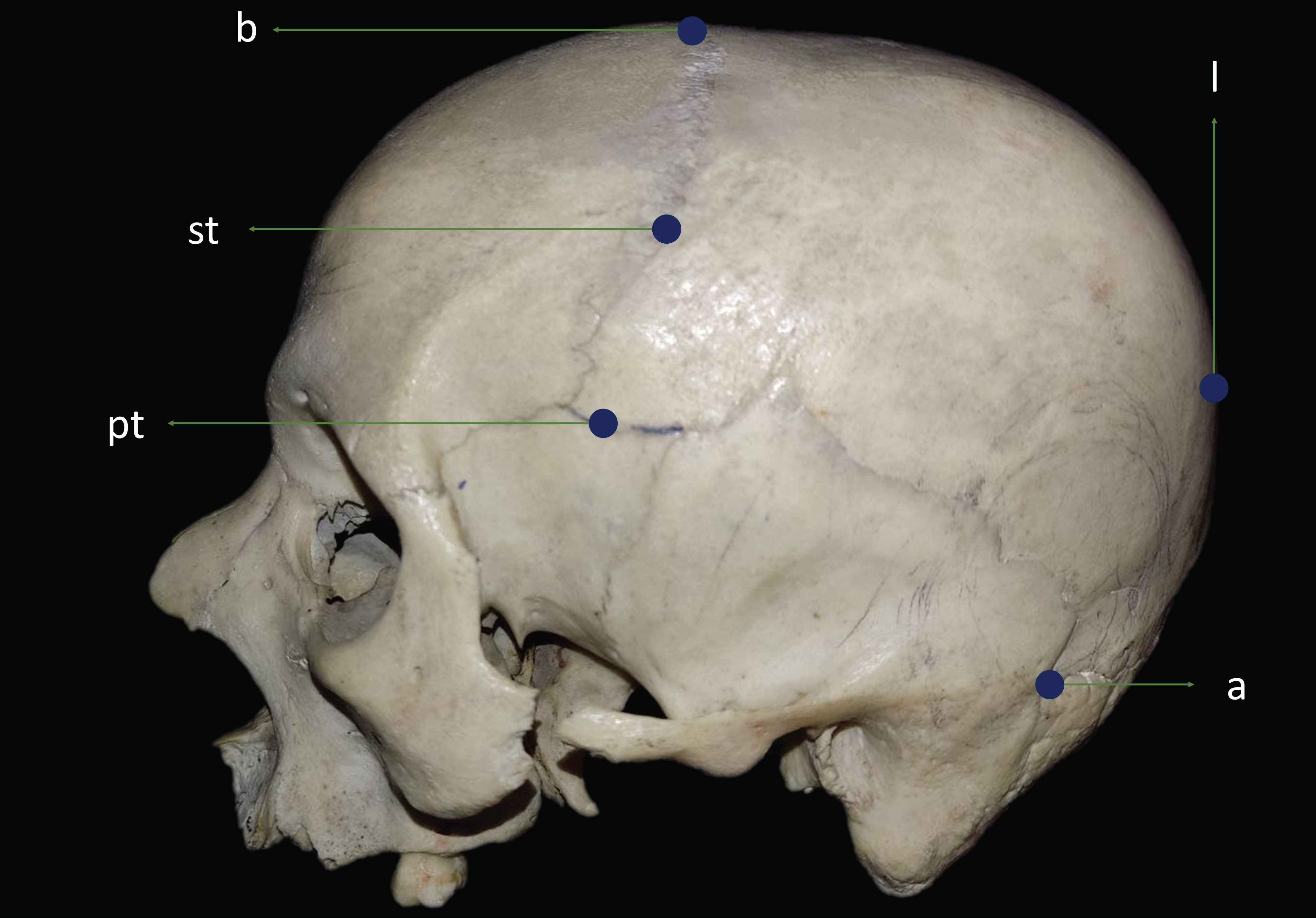 Figure 5: Left lateral view of the Peruvian skull from the medial craniometric points.
Figure 5: Left lateral view of the Peruvian skull from the medial craniometric points.
b: Brema; st: Stephanion; pt: Pterion; l: Lambda; a: Asterion
View Figure 5
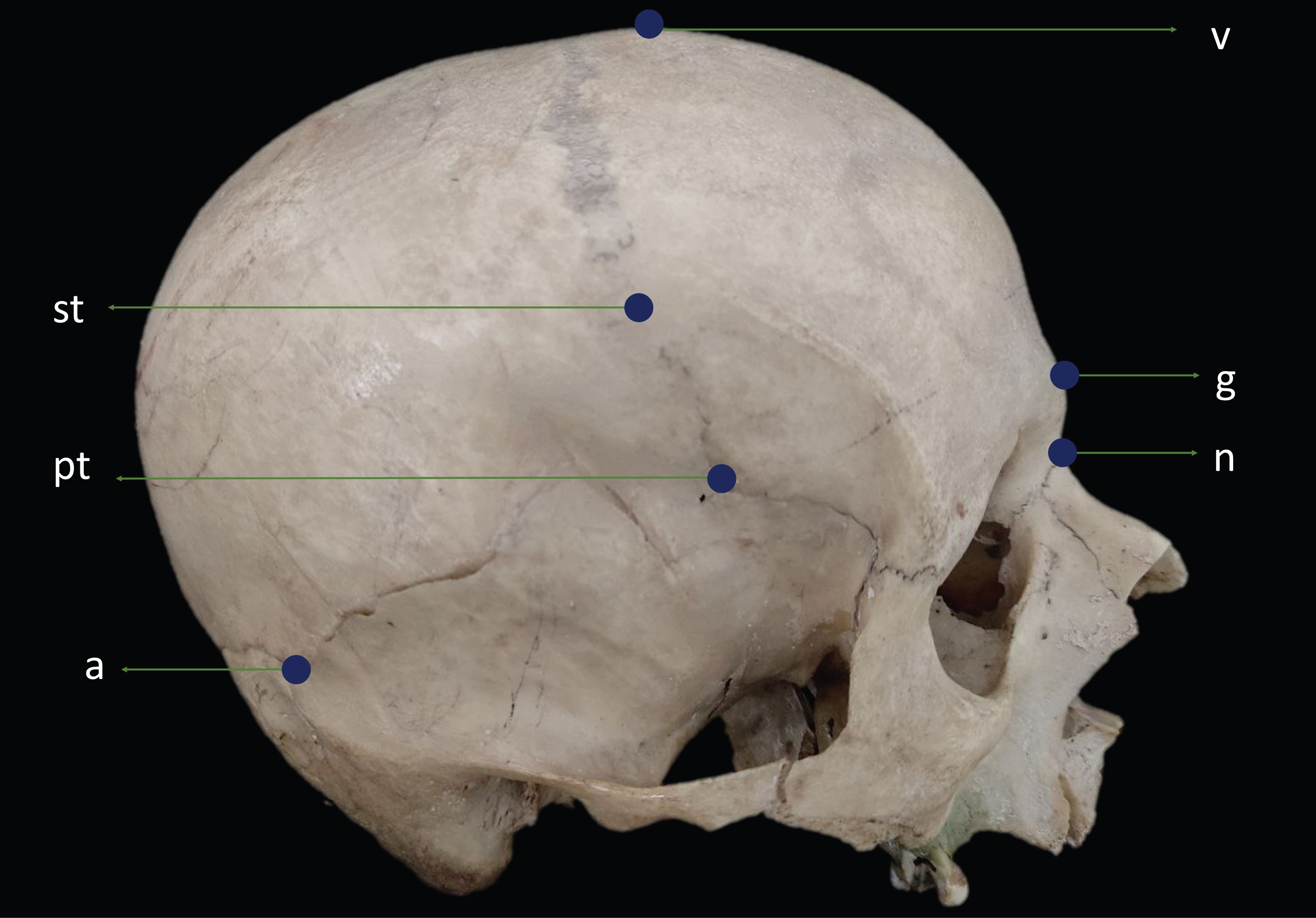 Figure 6: Right lateral view of the Peruvian skull from the medial craniometric points.
Figure 6: Right lateral view of the Peruvian skull from the medial craniometric points.
v: Vertex; st: Stephanion; g: Glabella; n: Nasion; pt: Pterion; a: Asterion
View Figure 6
Table 3: Craniometry measurement of the right and left hemicranium: Levene test. View Table 3
Table 4: Craniometric measurements of the Peruvian specimens. View Table 4
Table 5: Craniometry measurement: median, mean � standard deviation, minimum and maximum values (cm). View Table 5
The average craniometric measurement between nasion and bregma was 11.27 cm and between bregma and lambda, 11.35 cm. In relation to the posterior surface, the average distance between lambda and inion was 6.78 cm and between inion and opisthion of 4.61 cm. The mean measurements between the nasion-inion and opisthion-basion were 29.4 cm and 3.41 cm, respectively. The average vertical distance between the bregma-stephanion of 6.94 cm and the stephanion-pterion of 3.49 cm; and the mean horizontal distance between the pterion and the asterion was 10.5 cm.
In recent years, cranial morphometrics have become the most common analysis in anthropological sciences that aim to explain global patterns of cranial variation, which have given rise to multiple hypotheses [18]. Over time, the relationship between our cranial morphology and diversity of the human species has been studied. Consequently, current research reports allometric variations in facial proportions in relation to the total cranial size among Native American and Northeast Asian skulls size are currently reported in skulls of Native Americans and Northeast Asians [19]. Therefore, this study presents the characteristics of the Peruvian Andean phenotype to the scientific community for future cranial research.
The sample of 10 skulls is a widely representative base, aiming to establish a national precedent in anatomy education with cadavers, as this practice is sporadic in our country. In 2012, the International Federation of Associations of Anatomists (IFFA) recommended the teaching and research of anatomy using donated bodies [21]. However, undocumented challenges specific to our national context result in the absence of such academic work and research. Therefore, at the local level, IFFA proposes that anatomy departments encourage their faculties to introduce and manage local programs for the donation of cadaveric specimens. This would enable adherence to IFFA recommendations, thus enhancing public confidence [21]. Moreover, the Italian precedent regarding regulations outlined in the law for the donation of bodies and post-mortem tissues for educational purposes, offers guidance to lawmakers in countries where such policies have not yet been successfully implemented.
The extensive range of literature in neuroanatomy and anthropometry complicates the interpretation of cranometric analysis on a global scale. Through the review of 20 scientific articles concerning craniometry, the diversity in measurements becomes apparent, necessitating the extrapolation of data within the context of similar terms that refer to cranometric points. Authors Caple and Stephan (2015) have established a standardization of definitions that has played a pivotal role in this current study [17].
During a systematic literature review, it was observed that Peruvian cranial measurements exhibit distinct dimensions not only within Latin America but also on a global scale (Table 6). When comparing the data with Carreño et al. (2022) and Ribas et al. (2006), the measurements of nasion-bregma, nasion-lambda, and bregma-lambda were significantly larger compared to our findings. Furthermore, when comparing with the Thai and Indian populations studied by Ramamoorthy et al. (2016) and Mahakkanukrauh et al. (2015), respectively, it becomes evident that the nasion-bregma and bregma-lambda measurements are smaller compared with Peruvian craniometry. These observations hold practical implications, particularly in the field of neurosurgery, as they underscore the importance of considering the lengths of different cranial landmarks when planning a surgical approach on the skull. Therefore, it is essential for neurosurgeons, to take into account the positions of medial cranial landmarks for each patient before the surgical procedure [23-26].
Table 6: Measurement of medial craniometric points worldwide. View Table 6
Understanding dimensions of the posterior cranial fossa and the foramen magnum is essential to prevent potential complications during surgical procedures. Table 6 describes the seemingly larger opisthion-basion measurement values reported by Kranioti et al. (2008) in their analysis of extensive collections of American and South African cadaveric specimens values of the opistion-basión measurement are those described by Kranioti, et al, in their analysis of large collections of American and South African cadaveric pieces [27]. Currently, differences in the length of the foramen magnum are being identified. Therefore, the authors consider it important to delve deeper into future studies related to dimensions of the posterior cranial fossa, as these structures are relevant to pathologies involving the posterior fossa and the craniovertebral junction.
The cranial index is a widely recognized marker in anthropometry; however, its definition can introduce ambiguity in cranial dimensions. The cranial index, also referred to it as the cephalic index, assists in categorizing the shape of an individual's skull within a specific geographical area. In neurosurgery, it is employed to evaluate the correction of skull deformations [28]. Nevertheless, it also serves as an anthropometric tool that has contributed to the diversity of data analyzed in this review. The variety in dimensions, asymmetries, and cranial vault dysmorphology prompt us to reconsider the measurements of medial cranial landmarks, extending from the nasion to the opisthion. Consequently, cranial dimensions remain an enigma awaiting for resolution.
Efforts should be directed towards developing of clinical practice guidelines that are relevant to our national context. The 2020 edition of the severe traumatic brain injury management guide recommends a long frontotemporoparietal decompressive craniectomy, not exceeding 12 x 15 x 15 cm. (Level of recommendation IIA) [29]. However, this international consensus does not account for the unique challenges faced in Latin America. A decompressive craniectomy, as per our data collection; adhering to the American guideline might not be the optimal approach in our country, given the variations in the measurements of cranial landmarks within our population. Creating clinical practice guidelines tailored to the Peruvian population will indeed pose an additional challenge for young neurosurgeons, demanding their attention and adaptation.
The study's limitations are associated with the sample size, which is influenced by various challenges arising from national policies governing the use of anatomical specimens. Additionally, the authors emphasize that including demographic data for each skull would enhance the breadth of our description of Peruvian morphometry.
Understanding of Peruvian cranial measurements is crucial for young neurosurgeons when performing surgical procedures, as it helps prevent complications related to neural and anatomical structure injuries.
This study demonstrates that Peruvian craniometry were lower in comparison to other studies conducted in Latin America, while they were higher when compared to their counterparts in Thailand and India. Furthermore, the data analyzed in Peru encourages researchers to reconsider measurement approaches based on international consensus, with the aim of establishing global cranial vault dimensions of measurements based on international consensus to determine the dimensions of the cranial vault at a global level.
Our findings provide new insights into Peruvian morphometry, which can guide neuroanatomical knowledge within our country. In the long term, this knowledge has the potential to contribute to the reduction of morbidity and mortality associated with surgical interventions.